
Wed, May 20, 2026


Volume 14, Issue 1 (1-2026)
J. Pediatr. Rev 2026, 14(1): 37-52 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hajialibeig A, Enayati A A, Hosseinzadeh F, Taji M, Rezai M S. An Outline of Dengue Fever in Iran, Focusing on Pediatric Manifestations and Case Management: A Narrative Review. J. Pediatr. Rev 2026; 14 (1) :37-52
URL: http://jpr.mazums.ac.ir/article-1-722-en.html
URL: http://jpr.mazums.ac.ir/article-1-722-en.html
Azin Hajialibeig1 

 , Ahmad Ali Enayati2 , Fatemeh Hosseinzadeh3 , Marziyeh Taji3 , Mohammad Sadegh Rezai *4
, Ahmad Ali Enayati2 , Fatemeh Hosseinzadeh3 , Marziyeh Taji3 , Mohammad Sadegh Rezai *4
, Ahmad Ali Enayati2 , Fatemeh Hosseinzadeh3 , Marziyeh Taji3 , Mohammad Sadegh Rezai *4
1- Pediatric Infectious Diseases Research Center, Communicable Diseases Institute, Mazandaran University of Medical Sciences, Sari, Iran.
2- Health Sciences Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran.
3- Student Research Committee, Mazandaran University of Medical Sciences, Sari, Iran.
4- Pediatric Infectious Diseases Research Center, Communicable Diseases Institute, Mazandaran University of Medical Sciences, Sari, Iran. ,drmsrezaii@yahoo.com
2- Health Sciences Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran.
3- Student Research Committee, Mazandaran University of Medical Sciences, Sari, Iran.
4- Pediatric Infectious Diseases Research Center, Communicable Diseases Institute, Mazandaran University of Medical Sciences, Sari, Iran. ,
Full-Text [PDF 1447 kb]
(160 Downloads)
| Abstract (HTML) (322 Views)
Full-Text: (106 Views)
Introduction
The term “dengue” comes from a Swahili phrase, “Ka-dinga pepo,” which means a cramp-like seizure caused by an evil spirit. Dengue viral infection (DVI) is a debilitating disease transmitted by mosquitoes, primarily of the genus Aedes in the Culicidae family. The key species include Aedes aegypti, originally from Africa and now prevalent in tropical and subtropical regions, and Aedes albopictus, originally from Southeast Asia and now found in tropical, subtropical, and temperate areas. A. aegypti is generally a more efficient vector of the virus [1]. These mosquito species possess biological, behavioral, and ecological traits that enable them to serve as efficient vectors of arboviral disease (Table 1).
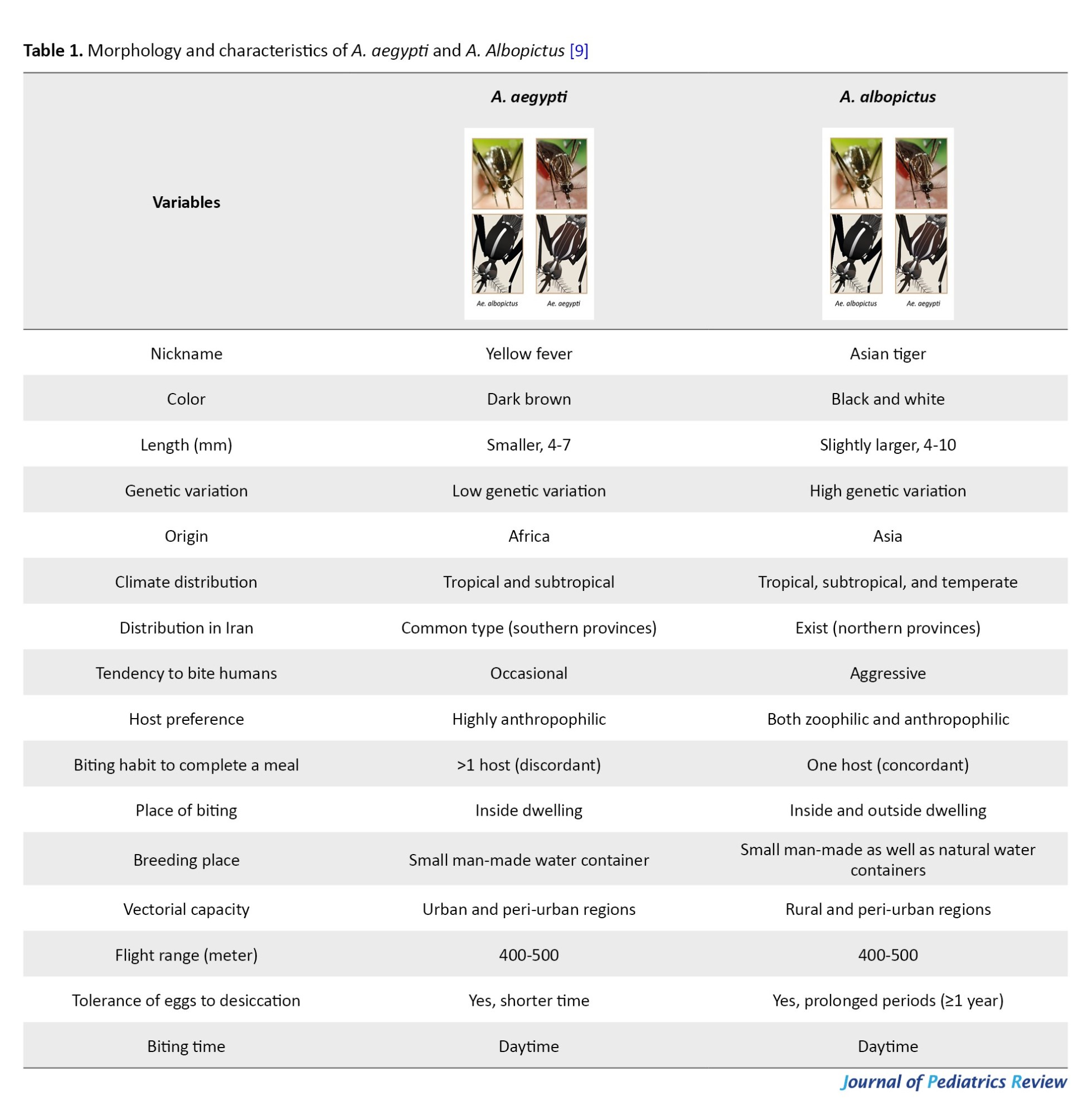
Existing literature reveals significant gaps in our understanding of pediatric dengue, as most studies focus on adult manifestations while underrepresenting children, who often exhibit atypical symptoms such as gastrointestinal distress and a propensity for rapid clinical deterioration. The lack of standardized diagnostic criteria and early warning markers for severe dengue in children hampers the development of effective, age-specific management protocols [2]. This narrative review aimed to provide a comprehensive overview of dengue fever in Iran with a particular focus on pediatric manifestations and case management strategies. This review seeks to synthesize current knowledge on the epidemiology, clinical features, and treatment approaches, highlighting gaps for future research and improving understanding among healthcare professionals.
Materials and Methods
This narrative review provides a comprehensive overview of dengue fever in Iran, with a particular focus on pediatric manifestations and approaches to case management. A broad literature search was carried out across major scientific databases, including ISI, PubMed, Scopus, and Google Scholar, using keywords such as “dengue fever,” “Iran,” “pediatric,” and “case management.” Articles published in English and Persian up to September 2025 were considered. Selected studies included original research, reviews, case reports, and national health reports relevant to the epidemiology, clinical features, and treatment strategies of pediatric dengue fever in Iran. The literature was organized thematically to synthesize current knowledge on the burden of disease, clinical presentations in children, and management guidelines. The review process prioritized depth of analysis and interpretation over exhaustive, systematic inclusion, consistent with the narrative review methodology.
Definitions of Clinical Syndromes
A. aegypti is a daytime-biting mosquito and a vector for several viral diseases, including dengue virus, yellow fever virus, chikungunya virus, and Zika virus, each with its own clinical syndrome [1]. The coexistence of A. aegypti and A. albopictus vectors in the same areas may increase the risk of human infection or co-infection [3].
Yellow fever
The yellow fever virus, an RNA flavivirus, is prevalent in tropical regions of Africa and South America. It is not commonly found in Asia, but could become an issue in Iran due to the potential return of unvaccinated travelers from outbreak areas [4]. The initial symptoms include acute-onset fever, headache, myalgia, low back pain, nausea, and vomiting, with nonspecific signs often appearing after a 3-10-day incubation period [3].
Yellow fever exhibits a wide range of clinical presentations, from asymptomatic or subclinical infections with no noticeable symptoms to severe and potentially life-threatening illness. Severe cases are marked by a classic triad of hemorrhage, jaundice, and albuminuria, indicating a high risk of mortality [5]. In these cases, symptoms may subside temporarily before recurring with severe manifestations such as high fever, headache, lower back (lumbosacral) pain, nausea, vomiting, abdominal pain, impaired consciousness, bradycardia, severe hepatitis, shock, and extensive hemorrhage, known as the “intoxication period” [6].
Chikungunya fever
Chikungunya fever is a short-duration fever, a dengue-like febrile syndrome with an incubation period of 2-4 days [7]. The clinical presentation and outcomes in children differ from those in adults [8]. Infants typically experience a sudden onset of fever followed by skin flushing, which may progress to a generalized maculopapular rash and lymphadenopathy after 3 to 5 days. Conjunctivitis and pharyngitis are also common, and some infants may exhibit a biphasic fever curve and arthralgia [7].
Older children may experience headache, myalgia, and arthralgia following a fever. Joint pain is usually polyarticular, bilateral, and symmetric, affecting the extremities and larger joints [8]. A macular blush appears early, followed by a maculopapular rash and pronounced lymphadenopathy. Hemorrhagic symptoms are rare in this age group. In adults, Chikungunya fever manifests with fever, followed by leukopenia, a maculopapular rash, and persistent arthralgia, which can progress to polyarthritis lasting for months [10].
Zika
The Zika virus is a single-stranded RNA flavivirus. Most acute Zika virus infections are asymptomatic, with 60%-80% of cases showing no symptoms. Symptoms are typically mild, last a few days to a week, and include fever, an itchy maculopapular rash, arthralgia and myalgia, and conjunctival hyperemia [11]. Other symptoms may include headache, extremity edema, vomiting, orbital pain, and lymphadenopathy. In rare conditions, laboratory abnormalities may present, including thrombocytopenia, leukopenia, and elevated liver enzymes. Neurological complications such as Guillain-Barré syndrome have been reported in rare cases [12].
Zika virus infection during pregnancy can lead to severe congenital malformations in the infants, such as microcephaly, hypertonia, abnormality in the eyes, and hearing disorder [13]. The long-term effects of Zika infection in children and adolescents are still being studied, emphasizing the need to understand its impact over a lifetime [14].
In patients with a history of recent travel to hyperendemic areas or with sexual partners who have recently traveled to such areas, Zika virus infection should be considered [15]. Because the symptoms of dengue and chikungunya virus infections are similar, patients should be evaluated for all three viruses [16].
Transmission
Due to the species’ sip-feeding behavior and biting a full blood meal, explosive transmission is expected. The transmission usually occurs during wet seasons. A. aegypti is highly domesticated and breeds in stored or freshwater containers, especially when they are not in use during dry seasons, and has implications for disease transmission [17]. Mosquitoes only need a small amount of water to lay eggs in any container that collects water, such as a used tire or can. Eggs are laid along the water line in the water container, stick to the container walls like glue, and can survive long periods of desiccation. Due to its limited flight range (400-500 m), which has epidemiological and interventional implications, A. albopictus is also a competent vector of dengue and, when present on its own in an area, acts as the main vector [18].
Dengue virus transmission occurs in two cycles: Enzootic (monkeys-Aedes-monkeys) and epidemic (human-Aedes-human) [19]. Dengue viruses can replicate in the gut, brain, and salivary glands of mosquitoes without harming adult mosquitoes. Mosquitoes remain capable of spreading the virus throughout their lifespans, which can extend up to 70 days under controlled experimental conditions. Due to their extended lifespan and need to take multiple blood meals, female mosquitoes are highly effective vectors. The dengue virus also infects the genital tract and can enter fully developed eggs during oviposition [20].
Initially, dengue is transmitted by the bites of infected mosquitoes. The virus can then spread to others through bites, with human-to-mosquito transmission occurring from viremic individuals, both symptomatic and asymptomatic, from two days before symptom onset to two days after fever resolution. Transmission through blood products, organ donation, and transfusions is rare.
Although the possibility of maternal transmission of dengue during pregnancy is low, pre-term labor, low birth weight, and fetal distress may occur. The virus is also transmitted during labor [21]. Dengue virus has been detected in breast milk, but because of the benefits of breastfeeding, it is still recommended even if a dengue infection is suspected [22].
Other transmission routes include blood transfusion, organ transplant, needlestick injuries, and possibly sexual contact, though these occurrences are rare [23]. Children, especially those under 15, are particularly vulnerable to dengue. Infants and young children are at a higher risk of developing severe complications, such as dengue shock syndrome (DSS) [20].
Epidemiology
Benjamin Rush documented the first dengue outbreak in Philadelphia, Pennsylvania, in 1780. Research indicates that dengue viruses likely originated in tropical regions of Asia. A. aegypti, a mosquito species native to Africa, is now widespread throughout tropical and subtropical regions [24]. Dengue is now prevalent in over 100 countries across the world regions of Africa, the Americas, the Eastern Mediterranean, Southeast Asia, and the Western Pacific. The most severely affected areas are the Americas, Southeast Asia, and the Western Pacific, with Asia bearing approximately 70% of the global disease burden. It is estimated that 390 million dengue infections occur each year, with 96 million people experiencing varying degrees of severity [25].
By April 30, 2024, World Health Organization (WHO) reported over 7.6 million dengue cases, including 3.4 million confirmed, >16,000 severe, and >3,000 deceased cases. Dengue cases have increased in the past 5 years, particularly in the Americas, with the highest number recorded in 2023, affecting over 80 countries. Many endemic countries lack adequate detection and reporting systems, leading to an underestimation of the true global burden of dengue [26]. Clinically apparent dengue can affect all age groups, but it is most frequently observed in children aged 5-15 years, with the highest mortality in children under 5 [27]. Dengue is among the top 10 leading causes of death in children under 15 years in tropical Asian countries [28].
Fewer than 20 imported dengue cases were reported annually in Iran before 2024. On June 14, 2024, the first 2 locally acquired dengue cases were reported. During 2024, Iran experienced a surge in imported dengue cases, and approximately 1127 cases of dengue fever were identified, of which 922 cases were attributed to local transmission, and 20% of the infected patients were children (4% between 1-10 years and 16% between 11-20 years old) [29]. The highest incidence was reported in Chabahar and Bandar Lengeh. Furthermore, from the beginning of 2025 through September 14, 434 new cases were documented nationally, and 20% were in the pediatric population (3% between 1-10 years and 17% between 11-20 years old) [3, 30].
Clinical Manifestations
Dengue fever in children can present with a range of clinical manifestations from mild to severe [31]. The duration and severity of the fever can vary widely. Following an intrinsic incubation period of 3-14 days (typically 4-7 days), the dengue virus progresses through three main phases: The febrile phase lasting 2-7 days, the critical phase within 1-2 days, and the recovery phase between 2-7 days [32]. Most children will only experience the febrile phase. However, some children may experience the critical phase, which is not easily predicted [33].
Febrile phase
The febrile phase of dengue fever in children is similar to that in adults, typically lasting 2-7 days. Symptoms begin with a sudden onset of a high fever ranging from 39 to 40 °C. During this time, children may experience generalized symptoms such as headache, myalgia, and sometimes abdominal pain, accompanied by a maculopapular rash and mild hemorrhagic manifestations like epistaxis, petechiae, and purpura, ecchymosis, hematuria, and gastrointestinal bleeding may occur [34]. In children, the febrile stage is often complicated by gastrointestinal symptoms like vomiting and anorexia, which can sometimes mask the classic clinical picture seen in adults, making early diagnosis challenging [35]. Based on the fever’s degree, bradycardia is expected [36].
Hematologic studies during this phase often reveal characteristic changes, including thrombocytopenia, hyponatremia, elevated liver enzymes, and leukopenia, which, when interpreted alongside clinical features such as fever and rash, bolster the diagnostic suspicion of dengue [37]. Complications such as dehydration, febrile seizures, and neurological manifestations, including encephalitis and aseptic meningitis, may occur [38]. During the acute febrile period, dengue viruses circulate in the peripheral blood, potentially infecting other mosquitoes 2 days before the fever onset and 5 days after [39]. The virus spreads systemically over 8-12 days. After this incubation period, the virus can be transmitted to humans by subsequent mosquito bites [40]. Adults are more commonly affected by classic dengue fever than children. Management of the febrile phase involves supportive care, including hydration, rest, and antipyretics to manage fever and pain [41]. This phase lays the groundwork for subsequent stages of the disease, and its proper recognition is crucial for effective monitoring and timely supportive intervention [35].
Critical or leakage phase
In children, the leakage phase begins following the febrile phase, marking the onset of the critical phase, usually between 3 and 7 days of fever, around the time of defervescence, and lasts 24-48 hours. There is a marked increase in capillary permeability, leading to plasma leakage into interstitial spaces. Children in this phase may also experience intense abdominal pain and persistent vomiting (>3 times in one hour or >4 times in 6 hours), which serve as warning signs of imminent circulatory compromise and possible shock [31].
The critical phase is characterized by a fluid shift, resulting in thrombocytopenia following leukopenia, hemoconcentration, and hematocrit (HCT) elevation, along with clinical signs such as narrowing of pulse pressure, tachycardia, cool or clammy extremities, and, in some cases, altered consciousness [42]. Approximately 1-2 days following defervescence, a generalized maculopapular morbilliform rash appears, sparing the palms and soles, and disappears within 1-5 days [41]. In some cases, extremity edema and desquamation may occur [43]. During the second rash period, fever may recur, indicating a biphasic fever pattern [41]. Coagulation disorders, including gastrointestinal bleeding, menorrhagia, and bleeding from some organs, are reported following dengue fever outbreaks [43]. Given that pediatric patients often have less robust compensatory mechanisms compared to adults, prompt recognition and aggressive, tailored fluid management are essential to prevent further deterioration. Intravenous fluids and electrolytes may be necessary, especially if there are signs of shock or severe dehydration. Hospitalization is often required during this phase to manage symptoms and prevent complications [44]. Careful monitoring, with frequent assessments of vital signs, fluid balance, and laboratory markers, is important to direct timely intervention and improve outcomes in this vulnerable population [33].
In most cases, plasma leakage results in minimal or transient circulatory changes. However, in severe cases, this condition can lead to shock, organ failure, and disseminated intravascular coagulation, characterized by increased activated partial thromboplastin time and decreased fibrinogen levels. Major complications include severe hemorrhage and encephalopathy [45]. Also, large pleural effusions and ascites can cause respiratory distress. Other potential complications include hypervolemia, congestive heart failure, acute pulmonary edema, ischemic hepatitis, and hepatic encephalopathy [46].
Convalescence phase
The convalescence phase of dengue fever in children marks the recovery period following the resolution of the critical leakage phase. During this stage, which begins 2 to 3 days after defervescence, patients experience gradual improvement in clinical status, with stabilization of vital signs, resolution of gastrointestinal symptoms, and normalization of hematological parameters such as platelet count and HCT [44]. After the critical phase, extravascular fluid is gradually reabsorbed during recovery [47]. The patient remains hemodynamically stable and diuresis, although general weakness and fatigue can persist for several weeks. Clinical manifestations in this phase include a transient rash with small circular islands of unaffected skin, known as “white islands in a sea of red” [23]. Bradycardia and electrocardiographic changes are frequently observed. HCT levels stabilize or slightly decrease due to hemodilution, while leukocytosis and thrombocytosis may occur [44]. Supportive care during this period focuses on nutritional rehabilitation, hydration, gradual resumption of physical activity, and continued monitoring to ensure complete recovery and to rule out any late complications [23].
Dengue case classification
In 1997, World Health Organization (WHO) classified dengue infection into asymptomatic (95% of cases) and symptomatic infection, including dengue fever, dengue hemorrhagic fever (DHF), and DSS. Dengue fever is the milder form, characterized by high fever, rash, and muscle and joint pain. DHF is a more severe manifestation of the disease, involving bleeding, plasma leakage, and thrombocytopenia. DHF is categorized into four distinct grades [28, 48]: Grade I presented with fever, rash, and minor bleeding; grade II presented with spontaneous bleeding, positive tourniquet test, and low platelets; grade III characterized with signs of circulatory failure such as weak pulse, cold clammy skin, and restlessness; and grade IV characterized with severe circulatory failure leading to shock (DSS). The most severe form of dengue is known as DSS, characterized by profound shock with a rapid drop in blood pressure, leading to organ failure and potentially death [49].
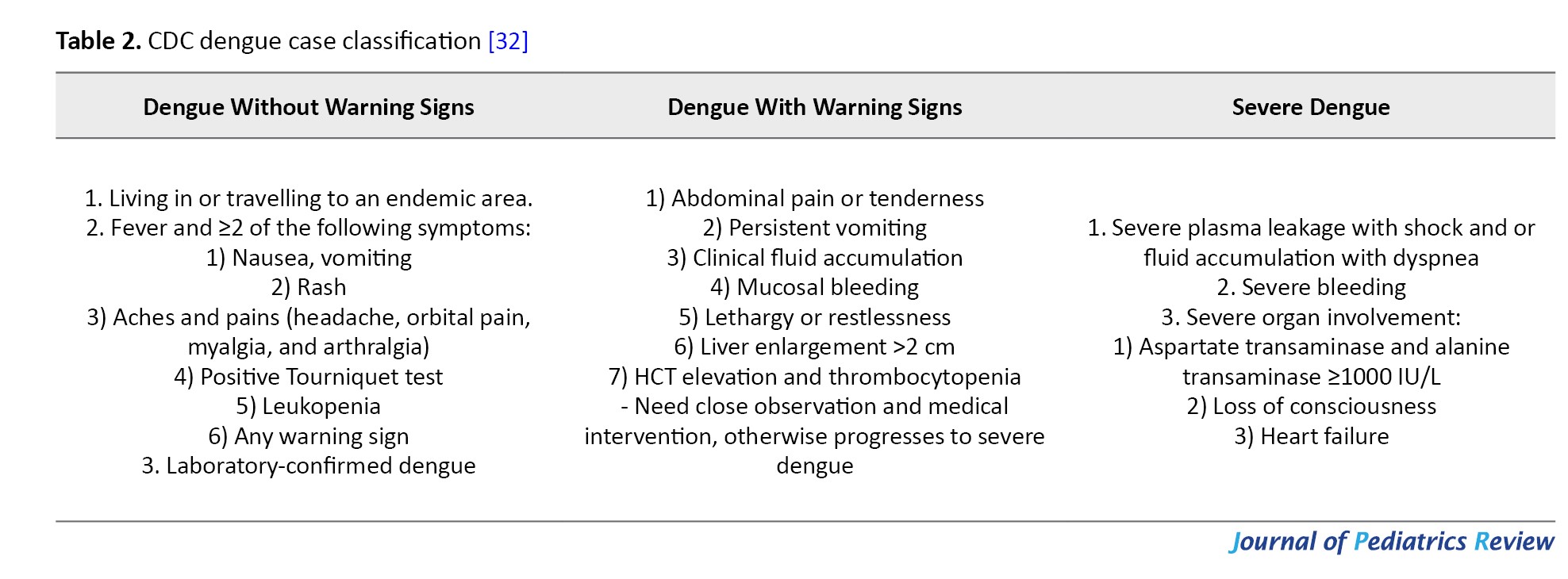
WHO introduced the term “expanded dengue syndrome” (EDS) for cases that do not meet the criteria for DHF or DSS but exhibit abnormal manifestations in various organs, including the cardiovascular, nervous, renal, gastrointestinal, and hematological systems. These unusual manifestations have been increasingly reported and are collectively referred to as EDS. According to the WHO 2009 definition, dengue is classified into three main categories to facilitate clinical management: dengue without warning signs, dengue with warning signs, and severe dengue [32, 48] (Table 2).
Recently, the centers for disease control and prevention (CDC) categorized dengue infections into dengue, dengue-like illness, and severe dengue. Dengue-like illness, characterized by fever, has been added to the list of notifiable infectious conditions [23].
DHF, DSS, and severe dengue
The WHO’s criteria for diagnosing DHF encompass the following items: fever; minor or major hemorrhagic manifestations, including a positive tourniquet test and thrombocytopenia (≤100000 /μL); and increased capillary permeability signs (HCT≥20%), pleural effusion, ascites, or hypoalbuminemia [28]. Identifying warning signs in an individual suspected of having dengue may indicate a need for hospitalization [32].
In severe dengue, increased vascular permeability leads to significant plasma leakage, which can cause hypotension, circulatory collapse, and organ dysfunction [29, 46]. The incubation period of severe dengue and dengue fever is similar. However, the progression of the illness has unique characteristics in infants and children [50].
There is a sudden onset of fever in the initial phase of dengue fever, followed by malaise, vomiting, headache, loss of appetite, abdominal pain, and upper respiratory symptoms, which may progress within 2 to 5 days [51]. Around the time of defervescence, symptoms such as cold extremities, slow capillary filling, warm trunk, facial flushing, cyanosis, sweating, irritability and restlessness, abdominal pain, oliguria, and hypovolemia may appear [52]. Forehead and extremities petechiae, spontaneous ecchymosis, and easy bruising and bleeding at venipuncture sites are common [51]. Tachypnea, tachycardia, and weak heart sounds may also be observed. Systolic pressure may remain stable or even increase initially; however, once hypotension develops, both systolic and diastolic pressures may drop to low or unmeasurable levels, potentially resulting in irreversible shock and fatality despite intensive resuscitation measures [52]. Firm and tender hepatomegaly, 4-6 cm below the costal margin, may occur [51].
Right unilateral or bilateral pleural effusions are the most common ultrasonographic indicator of plasma leakage on chest radiographs. Thickening of the gallbladder wall and ascites are less frequently detected and resolve more quickly than pleural effusions [53]. Up to 10% of patients may experience gross ecchymosis or gastrointestinal bleeding. Clinicians must be vigilant for warning signs during the shift from the febrile to the critical phase [52]. In children who recover, convalescence is usually rapid within 24-36 hours. The body temperature might normalize before or during the shock stage. It is important to note that dengue vascular permeability syndrome frequently occurs in infants aged 5 to 10 months in regions where multiple dengue virus strains are hyper-endemic. These infants are born to mothers with two or more lifetime dengue infections, making diagnosis more challenging and resulting in higher fatality rates [51].
Diagnosis
Diagnosis of dengue fever in children is a multifaceted process that relies on clinical evaluation, specific laboratory tests, and consideration of the geographic distribution to distinguish it from other febrile illnesses. Clinically, children may present with high fever, headache, myalgia, and a rash. Still, the onset can be more subtle than in adults, often accompanied by gastrointestinal symptoms such as nausea or abdominal pain [48].
DSS and DHF have similar diagnostic criteria, including hypotension, tachycardia, narrow pulse pressure (≤20 mmHg), and cold extremities. To confirm the diagnosis early in the febrile phase, clinicians frequently use virologic tests, including serologic tests, serum virus isolation, and detection of dengue virus viral RNA or non-structural protein 1 (NS1) [54]. Serologic diagnosis relies on a ≥4-fold increase in antibody titer, and IgM/IgG antibody detection confirms the infection [55].
In both primary and secondary infections, after 5 days, IgM antibodies are detected and typically disappear within 60 days (sensitivity: 61.5-100%; Specificity: 52-100%). Rapid IgM test strips, which have lower sensitivity, can also be used within the same duration. IgG antibody concentrations rise in secondary infection and are detectable 10 days following symptom onset in primary infection and 3 days following symptoms in secondary infection (Sensitivity: 46.4-99%; Specificity: 80%-100%). Consequently, during the initial 5 days of symptoms, IgM and IgG tests are typically negative [28].
The IgM/IgG ratio is >1.2 in primary infection and <1.2 in secondary infection. These proportions can vary based on the disease type. Point-of-care tests using IgM-capture ELISA and NS1 detection are available to diagnose acute infections, particularly useful from the third day of infection up to the seroconversion period, which can extend to 14 days (Sensitivity: 89.9-92.9%; Specificity: 75-100%). NS1 and IgM/IgG combo kits work similarly. If both NS1 and IgM are non-reactive while IgG is reactive, it indicates a secondary infection (Sensitivity: 93%; Specificity: 100%) [48]. Viral detection tests, including cell culture, RT-PCR of the RNA, and NS1, detect viral RNA from 1-5 days after symptom onset in primary infections and 1-4 days in secondary infections (Sensitivity: 40.5%; Specificity: 100%) [33] (Figure 1).
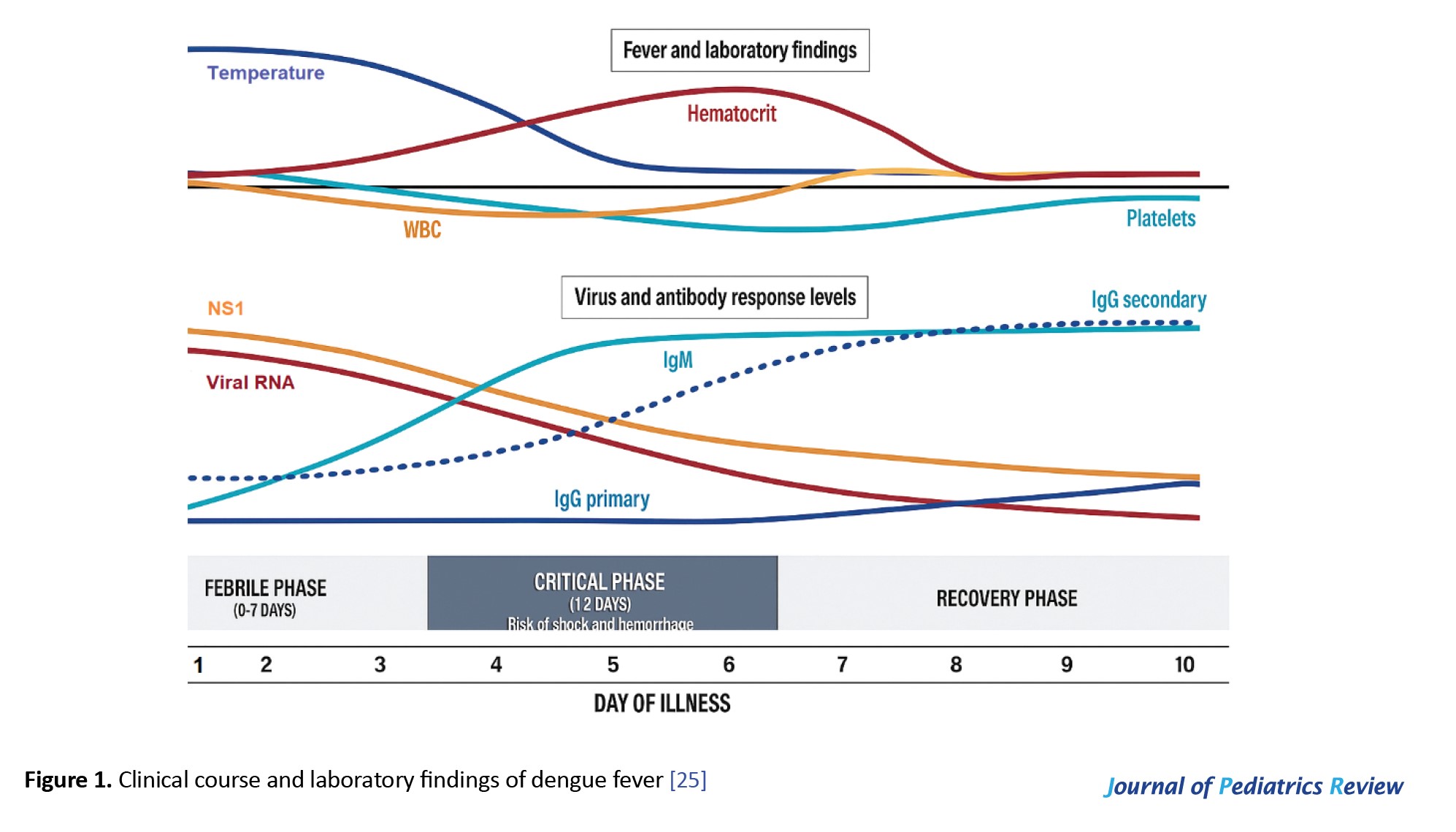 Additionally, hematologic tests typically reveal thrombocytopenia, leukopenia, and an elevated HCT due to plasma leakage, which are key indicators to assess disease severity in children. Combining clinical findings with targeted laboratory assessments enables timely and accurate diagnosis, which is critical for initiating appropriate supportive care and monitoring for potential complications in pediatric patients, where rapid disease progression is commonly observed [16, 48, 50].
Additionally, hematologic tests typically reveal thrombocytopenia, leukopenia, and an elevated HCT due to plasma leakage, which are key indicators to assess disease severity in children. Combining clinical findings with targeted laboratory assessments enables timely and accurate diagnosis, which is critical for initiating appropriate supportive care and monitoring for potential complications in pediatric patients, where rapid disease progression is commonly observed [16, 48, 50].
Differential Diagnosis
In children, the differential diagnosis of dengue virus infection is broad due to its clinical features overlapping with those of several other infectious diseases [56]. During the febrile phase, the differential diagnosis should include other arboviral infections, such as measles, rubella, enteroviruses, and adenoviruses, as well as influenza. Additionally, bacterial infections like leptospirosis or sepsis can mimic dengue, especially when gastrointestinal symptoms and hemorrhagic signs occur [52].
Febrile children presenting with rash and myalgia may also be evaluated for viral illnesses, such as chikungunya, measles, rubella, or erythema infectiosum, which can present with fever and rash. However, joint pain is more prominent with chikungunya [57].
In areas where multiple arboviruses might be endemic, O’nyong-nyong fever, West Nile fever, Oropouche, and Zika should be considered. Colorado tick fever, sandfly fever, Ross River fever, and mild Rift Valley fever are similar to DHF but do not present with rash. Malaria is the most common nonviral acute infectious disease that resembles DHF [57].
Diagnosis of dengue, chikungunya, and Zika is primarily clinical. Chikungunya is frequently observed in the same populations. It produces a dengue fever-like syndrome with a more abrupt onset and shorter duration as well as more frequent maculopapular rash, conjunctivitis, and myalgia or arthralgia [58].
Laboratory evaluation, including tests for the NS1 antigen, RT-PCR, and subsequent IgM/IgG serology, along with hematological findings like thrombocytopenia and hemoconcentration, is essential to distinguish dengue from these other entities [47].
Prevention and Vector Control
Based on the biology, ecology, and behaviour of A. aegypti and A. albopictus, as well as the epidemiology of the diseases they transmit, WHO has developed many strategic approaches to control these mosquito vectors. These strategies aim to prevent their establishment and distribution, as well as control epidemics [59].
Methods to prevent mosquito bites
Personal protection measures include wearing long protective clothing and sleeping under mosquito nets, especially for infants and young children, to minimize skin exposure. Additionally, applying repellents containing DEET, picaridin, IR 3535, and lemon eucalyptus oil to exposed skin and staying indoors during peak mosquito activity at dawn and dusk are effective prevention methods [20].
Home and Environment
Prophylaxis includes killing vector mosquitoes, avoiding mosquito bites, and solid waste management [28]. Control efforts should focus on the most productive and epidemiologically important habitats. These measures include eliminating standing water by removing stagnant areas where mosquitoes can breed, such as flowerpots, buckets, and old tires, and setting up mosquito traps around the home to reduce the mosquito population. Installing window and door screens to keep mosquitoes out and using indoor insecticides to eliminate mosquitoes in the home are also effective measures [54].
Community engagement
Community engagement is crucial for dengue prevention, as it involves educating residents about the Aedes mosquito’s life cycle and eliminating breeding sites through regular cleanup campaigns and source-reduction efforts. By promoting insect repellents, bed nets, and monitoring systems, communities can protect themselves from mosquito bites and swiftly report potential outbreaks. Collaboration with local authorities and training community health workers further enhances the effectiveness of vector control measures, fostering a proactive, united approach to reducing dengue transmission. Research and development of novel control strategies, including Wolbachia, sterile insect technique, and genetically modified mosquitoes, should also be promoted and funded [59-61].
As Iran is not yet in a hyperendemic area for dengue, vaccine administration is not currently warranted. In the absence of a viable dengue vaccine for Iran, a multifaceted integrated vector management strategy emerges as both feasible and urgently needed. Alternative approaches include deploying biological controls, such as releasing Wolbachia-infected Aedes mosquitoes, which interfere with the virus’s replication and naturally reduce the vector population over successive generations [62]. Alongside these measures, environmentally focused approaches, such as the use of plant-based larvicides and community-led initiatives to eliminate or manage breeding sites, promise a sustainable reduction in mosquito density while mitigating concerns about chemical insecticide resistance [63]. Moreover, innovative genetic methods such as gene-drive strategies and sterile insect techniques offer potential for long-term suppression of vector populations. However, they require rigorous field evaluation to ensure safety and effectiveness [62].
Vaccination
Currently, there are two licensed dengue vaccines. Dengvaxia (CYD-TDV), a live recombinant tetravalent vaccine developed by Sanofi Pasteur, has received FDA approval and integrates the structural regions of the four DENV serotypes. It is approved for use in 16 countries and is administered as a series of three doses, with each dose spaced 6 months apart. The vaccine is recommended for individuals aged 9-45 years (or 9-60 years, depending on country-specific regulatory approvals) who have had a prior dengue infection. WHO does not recommend it for patients with negative serum. Pre-vaccination screening for previous dengue infection is required [64]. A large, well-designed, multi-country clinical trial of Dengvaxia shows that nearly all vaccinated individuals develop tetravalent neutralizing antibodies [65].
Developed by Takeda and designed by the CDC, Qdenga (TAK-003) is a live-attenuated vaccine composed of weakened dengue virus serotypes 1-4. It is used as a 2-dose series with a 3-month interval and is recommended for children aged 6-16 years in areas with high dengue transmission. In clinical trials, vaccinated seronegative individuals showed positive outcomes [65, 66].
Current dengue fever management in Iran
Iran’s current dengue fever management policies emphasize vector control, capacity building, and intersectoral collaboration in efforts to curb disease transmission, as outlined in recent national systematic reviews [59]. However, compared with the WHO guidelines, which emphasize integrated surveillance, early case detection, standardized diagnostic protocols, and rigorous clinical management, especially for severe dengue, the Iranian approach appears less comprehensive and less uniformly implemented [32, 67]. While endemic countries have refined their strategies by establishing robust early warning systems and optimizing fluid management protocols to reduce mortality, Iran’s policies still face challenges, including gaps in rapid-response mechanisms and inconsistent clinical practices across regions. Strengthening these areas and aligning more closely with WHO standards could enhance the overall effectiveness of dengue management in Iran, particularly as the threat of local transmission escalates.
Treatment and Disease Management
Treatment for dengue is supportive, including bed rest, antipyretics, analgesics, sedation, and fluid and electrolyte replacement therapy [32] (Table 3).
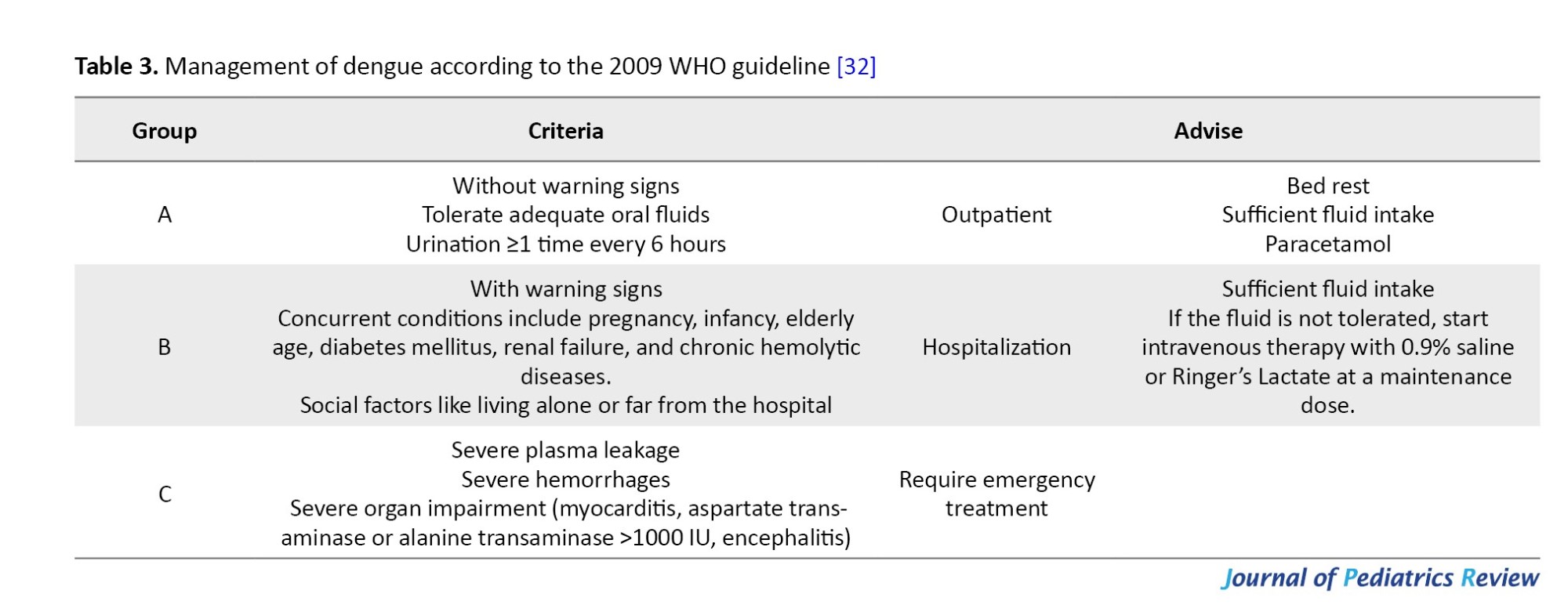
Aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) should be avoided because they increase the risk of Reye’s syndrome and dengue hemorrhagic disease. Corticosteroids are not routinely indicated due to their adverse effects [65]. A baseline HCT should be checked.
Patients with mild DHF or warning signs
Blood pressure below 90/60 mmHg, HCT greater than 50%, thrombocytopenia (PLT<50000/mm³), and evidence of bleeding other than petechiae are key indicators [28]. Oral fluid intake, such as fruit juice and electrolyte and dextrose solutions, is essential and preferred over plain water. Salicylates should be avoided for fever control due to the risk of bleeding and acidosis. Administer acetaminophen at the following doses: Less than 1 year, 60 mg; 1-3 years, 60-120 mg; 3-6 years, 120 mg; and 6-12 years, 240 mg [68].
DHF (compensated shock)
Critical care management of vascular permeability is necessary for patients with compensated shock. Shock may develop in approximately one-third of patients, making a baseline hemoglobin measurement essential [28]. Close observation for signs of bleeding and circulatory compromise, along with prompt supportive treatment, is crucial in the management of the patients, as the severity of shock may change within 48 hours. Volume depletion is often a consequence of fever, inadequate oral intake, bleeding, and plasma leakage [53].
Intravenous fluid resuscitation with an isotonic crystalloid solution at a rate of 5-10 mL/kg/h over 1 hour is recommended. However, this must be carefully adjusted to maintain adequate circulation, as serious complications such as pulmonary edema and respiratory failure may occur due to excessive fluid administration [53].
If the patient’s condition improves, gradually reduce intravenous fluids to 5-7 mL/kg/h for 1-2 hours, followed by 3-5 mL/kg/h for 2-4 hours, and then to 2-3 mL/kg/h, adjusting further based on hemodynamic status. If vital signs remain unstable after the initial bolus, check the HCT. If it increases or is > 50%, infuse a second bolus at 10-20 mL/kg/h for 1 hour. If there is improvement after the second bolus, reduce the rate to 7-10 mL/kg/h for 1-2 hours. If the HCT decreases from the baseline level, significant hemorrhage may be present, and a blood transfusion may be necessary. Additional boluses of crystalloid solutions might be necessary over the following 1-2 days [25, 69].
DSS
In cases of shock, crystalloid fluid is administered as a bolus of 10-20 mL/kg over 15 minutes to maintain blood pressure [33], and, in cases with poor response, colloid fluid is administered [53]. If the patient’s condition improves, continue the crystalloid/colloid infusion at 10 mL/kg/h for 1 hour. Subsequently, continue the infusion and slowly reduce the rate to 5-7 mL/kg/h for 1-2 hours, then to 3-5 mL/kg/h for 2-4 hours, and finally to 2-3 mL/kg/h or less, which can be maintained for up to 24 to 48 hours. A common question for healthcare personnel managing dengue patients is whether to transfuse platelet products [33]. Bleeding tendency and platelet counts are not always correlated and can be present in children with normal platelet counts [70]. This condition underscores the need to clarify the indications for platelet transfusion in thrombocytopenic dengue patients without overt hemorrhage [33].
If vital signs are unstable, the first HCT determines the need for a blood transfusion. In cases with HCT above baseline, a second bolus of colloid at 10-20 mL/kg/h is administered within 30 minutes to 1 hour, and the patient is reassessed. After improvement, reduce the rate to 7-10 mL/kg/h for 1-2 hours, then replace it with a crystalloid solution and gradually reduce the infusion rate. If the condition remains unstable after the second bolus, recheck the HCT and transfuse blood if it decreased. If it has elevated or remains very high, infuse colloid solutions at 10-20 mL/kg/h as a third bolus over 1 hour and then reduce the rate to 7-10 mL/kg/h for 1-2 hours, then return to a crystalloid solution and gradually reduce the infusion rate. Additional boluses might be required over the following 24 hours [32].
In unresponsive shock patients, up to 40-60 mL/kg of fluid, 5-10 mL/kg of fresh red blood cells, or 10-20 mL/kg of fresh whole blood should be transfused, especially in the presence of severe bleeding. If the equipment is available, place an arterial catheter for frequent blood pressure monitoring and blood sampling. It is important to monitor EKG and pulse oximetry, and to check urine output and HCT (before and after administering fluid boluses, and then every 4-6 hours). Also, arterial or venous blood gases, lactate, total CO2 and HCO3, and blood glucose levels should be checked every 30 minutes to 1 hour until stable. Patients with prolonged, refractory, or hypotensive shock, renal or liver insufficiency, persistent metabolic acidosis, preexisting peptic ulcer disease, trauma, or those treated with nonsteroidal anti-inflammatory or anticoagulant agents are at high risk for hemorrhage [25].
Discharge Criteria
Patients with dengue who do not exhibit warning signs, tolerate adequate oral fluids, urinate at least once every 6 hours, and do not have associated diseases, chronic conditions, or social risk factors can be discharged with supportive treatment. Also, those with improved appetite, normal vital signs and breathing, no evidence of bleeding, increased platelet counts, and stable HCT can be discharged. They should be followed up on every 24–48 hours until they have been afebrile for 48 hours [71].
These patients should have normal or near-normal hemoglobin/HCT and platelet levels. They should not have concurrent conditions as mentioned in Table 3. Fever management should involve acetaminophen, and aspirin and NSAIDs should be avoided [33].
Social and Psychological Challenges
Dengue fever can significantly impact both children and their families psychologically and socially. Children may experience anxiety, fear, and stress due to the illness and its symptoms, which can affect their emotional well-being and academic performance. Families may face social isolation as they make an effort to prevent the spread, and caregivers often experience stress and anxiety from the added responsibilities and financial burden of medical care. Overall, the impact can lead to a decreased quality of life and increased emotional strain on the entire family [72].
Education and Awareness in Children
Educating children about dengue and raising awareness are crucial to preventing its spread. Effective strategies include school-based programs with interactive lessons, role-playing, demonstrations, and field activities to identify and eliminate mosquito breeding sites. Educational materials such as posters, charts, board games, activities, storybooks, and comics can also convey key messages [73]. Community involvement through parental engagement, community cleanup campaigns, and participation in public health initiatives is essential. Additionally, digital tools such as educational apps and social media can be used to share educational content. Health-promoting schools can provide health kits and train teachers to deliver dengue prevention education effectively. By implementing these strategies, children can learn to protect themselves and their communities from dengue [34].
Follow-up
Follow-up care for children recovering from dengue fever involves regular check-ups to monitor progress, track vital signs, and perform blood tests. Symptom management includes providing pain relief, ensuring hydration, and encouraging rest. Educating parents about the warning signs of severe dengue and encouraging them to seek immediate medical care is crucial. During the recovery phase, children should gradually return to activities and maintain a balanced diet. It is also important to emphasize mosquito bite prevention measures to prevent reinfection [26].
Conclusion
The establishment of A. aegypti in southern Iran and the increasing presence of A. albopictus in the north heralds a pivotal shift in the epidemiology of dengue fever, particularly affecting pediatric populations. Given that children are highly vulnerable to severe dengue manifestations and account for approximately one-fifth of all infections in Iran, they represent a significant at-risk demographic that warrants specific public health and clinical consideration. This review highlights how children often present with atypical manifestations, such as prominent abdominal pain, vomiting, rash, and a rapid progression to vascular leakage and shock, which differ markedly from adult presentations. These nuances underscore the need for pediatric-specific case management protocols emphasizing early recognition and aggressive intervention. Moreover, given the dynamic spread of the disease, control strategies must combine targeted vector control and ongoing, specialized education for healthcare providers to ensure timely, effective responses in clinical settings. For these initiatives to succeed, robust national policies underscored by strong political will and intersectoral collaboration are essential.
Future research must prioritize well-designed, multicenter epidemiological studies and randomized controlled trials with a focus on refining pediatric guidelines for early diagnostic and prognostic biomarkers, evaluating tailored fluid management and treatment regimens, and assessing the efficacy, safety, and optimal dosing of emerging vaccines specifically in pediatric populations to reduce dengue morbidity and mortality among Iran’s most vulnerable populations.
Ethical Considerations
Compliance with ethical guidelines
This article is a narrative review, with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank the Iran Centers for Disease Control and Prevention (CDC) and the Ministry of Health and Medical Education for providing national epidemiological data and official statistics that contributed to this narrative review.
References
The term “dengue” comes from a Swahili phrase, “Ka-dinga pepo,” which means a cramp-like seizure caused by an evil spirit. Dengue viral infection (DVI) is a debilitating disease transmitted by mosquitoes, primarily of the genus Aedes in the Culicidae family. The key species include Aedes aegypti, originally from Africa and now prevalent in tropical and subtropical regions, and Aedes albopictus, originally from Southeast Asia and now found in tropical, subtropical, and temperate areas. A. aegypti is generally a more efficient vector of the virus [1]. These mosquito species possess biological, behavioral, and ecological traits that enable them to serve as efficient vectors of arboviral disease (Table 1).
Existing literature reveals significant gaps in our understanding of pediatric dengue, as most studies focus on adult manifestations while underrepresenting children, who often exhibit atypical symptoms such as gastrointestinal distress and a propensity for rapid clinical deterioration. The lack of standardized diagnostic criteria and early warning markers for severe dengue in children hampers the development of effective, age-specific management protocols [2]. This narrative review aimed to provide a comprehensive overview of dengue fever in Iran with a particular focus on pediatric manifestations and case management strategies. This review seeks to synthesize current knowledge on the epidemiology, clinical features, and treatment approaches, highlighting gaps for future research and improving understanding among healthcare professionals.
Materials and Methods
This narrative review provides a comprehensive overview of dengue fever in Iran, with a particular focus on pediatric manifestations and approaches to case management. A broad literature search was carried out across major scientific databases, including ISI, PubMed, Scopus, and Google Scholar, using keywords such as “dengue fever,” “Iran,” “pediatric,” and “case management.” Articles published in English and Persian up to September 2025 were considered. Selected studies included original research, reviews, case reports, and national health reports relevant to the epidemiology, clinical features, and treatment strategies of pediatric dengue fever in Iran. The literature was organized thematically to synthesize current knowledge on the burden of disease, clinical presentations in children, and management guidelines. The review process prioritized depth of analysis and interpretation over exhaustive, systematic inclusion, consistent with the narrative review methodology.
Definitions of Clinical Syndromes
A. aegypti is a daytime-biting mosquito and a vector for several viral diseases, including dengue virus, yellow fever virus, chikungunya virus, and Zika virus, each with its own clinical syndrome [1]. The coexistence of A. aegypti and A. albopictus vectors in the same areas may increase the risk of human infection or co-infection [3].
Yellow fever
The yellow fever virus, an RNA flavivirus, is prevalent in tropical regions of Africa and South America. It is not commonly found in Asia, but could become an issue in Iran due to the potential return of unvaccinated travelers from outbreak areas [4]. The initial symptoms include acute-onset fever, headache, myalgia, low back pain, nausea, and vomiting, with nonspecific signs often appearing after a 3-10-day incubation period [3].
Yellow fever exhibits a wide range of clinical presentations, from asymptomatic or subclinical infections with no noticeable symptoms to severe and potentially life-threatening illness. Severe cases are marked by a classic triad of hemorrhage, jaundice, and albuminuria, indicating a high risk of mortality [5]. In these cases, symptoms may subside temporarily before recurring with severe manifestations such as high fever, headache, lower back (lumbosacral) pain, nausea, vomiting, abdominal pain, impaired consciousness, bradycardia, severe hepatitis, shock, and extensive hemorrhage, known as the “intoxication period” [6].
Chikungunya fever
Chikungunya fever is a short-duration fever, a dengue-like febrile syndrome with an incubation period of 2-4 days [7]. The clinical presentation and outcomes in children differ from those in adults [8]. Infants typically experience a sudden onset of fever followed by skin flushing, which may progress to a generalized maculopapular rash and lymphadenopathy after 3 to 5 days. Conjunctivitis and pharyngitis are also common, and some infants may exhibit a biphasic fever curve and arthralgia [7].
Older children may experience headache, myalgia, and arthralgia following a fever. Joint pain is usually polyarticular, bilateral, and symmetric, affecting the extremities and larger joints [8]. A macular blush appears early, followed by a maculopapular rash and pronounced lymphadenopathy. Hemorrhagic symptoms are rare in this age group. In adults, Chikungunya fever manifests with fever, followed by leukopenia, a maculopapular rash, and persistent arthralgia, which can progress to polyarthritis lasting for months [10].
Zika
The Zika virus is a single-stranded RNA flavivirus. Most acute Zika virus infections are asymptomatic, with 60%-80% of cases showing no symptoms. Symptoms are typically mild, last a few days to a week, and include fever, an itchy maculopapular rash, arthralgia and myalgia, and conjunctival hyperemia [11]. Other symptoms may include headache, extremity edema, vomiting, orbital pain, and lymphadenopathy. In rare conditions, laboratory abnormalities may present, including thrombocytopenia, leukopenia, and elevated liver enzymes. Neurological complications such as Guillain-Barré syndrome have been reported in rare cases [12].
Zika virus infection during pregnancy can lead to severe congenital malformations in the infants, such as microcephaly, hypertonia, abnormality in the eyes, and hearing disorder [13]. The long-term effects of Zika infection in children and adolescents are still being studied, emphasizing the need to understand its impact over a lifetime [14].
In patients with a history of recent travel to hyperendemic areas or with sexual partners who have recently traveled to such areas, Zika virus infection should be considered [15]. Because the symptoms of dengue and chikungunya virus infections are similar, patients should be evaluated for all three viruses [16].
Transmission
Due to the species’ sip-feeding behavior and biting a full blood meal, explosive transmission is expected. The transmission usually occurs during wet seasons. A. aegypti is highly domesticated and breeds in stored or freshwater containers, especially when they are not in use during dry seasons, and has implications for disease transmission [17]. Mosquitoes only need a small amount of water to lay eggs in any container that collects water, such as a used tire or can. Eggs are laid along the water line in the water container, stick to the container walls like glue, and can survive long periods of desiccation. Due to its limited flight range (400-500 m), which has epidemiological and interventional implications, A. albopictus is also a competent vector of dengue and, when present on its own in an area, acts as the main vector [18].
Dengue virus transmission occurs in two cycles: Enzootic (monkeys-Aedes-monkeys) and epidemic (human-Aedes-human) [19]. Dengue viruses can replicate in the gut, brain, and salivary glands of mosquitoes without harming adult mosquitoes. Mosquitoes remain capable of spreading the virus throughout their lifespans, which can extend up to 70 days under controlled experimental conditions. Due to their extended lifespan and need to take multiple blood meals, female mosquitoes are highly effective vectors. The dengue virus also infects the genital tract and can enter fully developed eggs during oviposition [20].
Initially, dengue is transmitted by the bites of infected mosquitoes. The virus can then spread to others through bites, with human-to-mosquito transmission occurring from viremic individuals, both symptomatic and asymptomatic, from two days before symptom onset to two days after fever resolution. Transmission through blood products, organ donation, and transfusions is rare.
Although the possibility of maternal transmission of dengue during pregnancy is low, pre-term labor, low birth weight, and fetal distress may occur. The virus is also transmitted during labor [21]. Dengue virus has been detected in breast milk, but because of the benefits of breastfeeding, it is still recommended even if a dengue infection is suspected [22].
Other transmission routes include blood transfusion, organ transplant, needlestick injuries, and possibly sexual contact, though these occurrences are rare [23]. Children, especially those under 15, are particularly vulnerable to dengue. Infants and young children are at a higher risk of developing severe complications, such as dengue shock syndrome (DSS) [20].
Epidemiology
Benjamin Rush documented the first dengue outbreak in Philadelphia, Pennsylvania, in 1780. Research indicates that dengue viruses likely originated in tropical regions of Asia. A. aegypti, a mosquito species native to Africa, is now widespread throughout tropical and subtropical regions [24]. Dengue is now prevalent in over 100 countries across the world regions of Africa, the Americas, the Eastern Mediterranean, Southeast Asia, and the Western Pacific. The most severely affected areas are the Americas, Southeast Asia, and the Western Pacific, with Asia bearing approximately 70% of the global disease burden. It is estimated that 390 million dengue infections occur each year, with 96 million people experiencing varying degrees of severity [25].
By April 30, 2024, World Health Organization (WHO) reported over 7.6 million dengue cases, including 3.4 million confirmed, >16,000 severe, and >3,000 deceased cases. Dengue cases have increased in the past 5 years, particularly in the Americas, with the highest number recorded in 2023, affecting over 80 countries. Many endemic countries lack adequate detection and reporting systems, leading to an underestimation of the true global burden of dengue [26]. Clinically apparent dengue can affect all age groups, but it is most frequently observed in children aged 5-15 years, with the highest mortality in children under 5 [27]. Dengue is among the top 10 leading causes of death in children under 15 years in tropical Asian countries [28].
Fewer than 20 imported dengue cases were reported annually in Iran before 2024. On June 14, 2024, the first 2 locally acquired dengue cases were reported. During 2024, Iran experienced a surge in imported dengue cases, and approximately 1127 cases of dengue fever were identified, of which 922 cases were attributed to local transmission, and 20% of the infected patients were children (4% between 1-10 years and 16% between 11-20 years old) [29]. The highest incidence was reported in Chabahar and Bandar Lengeh. Furthermore, from the beginning of 2025 through September 14, 434 new cases were documented nationally, and 20% were in the pediatric population (3% between 1-10 years and 17% between 11-20 years old) [3, 30].
Clinical Manifestations
Dengue fever in children can present with a range of clinical manifestations from mild to severe [31]. The duration and severity of the fever can vary widely. Following an intrinsic incubation period of 3-14 days (typically 4-7 days), the dengue virus progresses through three main phases: The febrile phase lasting 2-7 days, the critical phase within 1-2 days, and the recovery phase between 2-7 days [32]. Most children will only experience the febrile phase. However, some children may experience the critical phase, which is not easily predicted [33].
Febrile phase
The febrile phase of dengue fever in children is similar to that in adults, typically lasting 2-7 days. Symptoms begin with a sudden onset of a high fever ranging from 39 to 40 °C. During this time, children may experience generalized symptoms such as headache, myalgia, and sometimes abdominal pain, accompanied by a maculopapular rash and mild hemorrhagic manifestations like epistaxis, petechiae, and purpura, ecchymosis, hematuria, and gastrointestinal bleeding may occur [34]. In children, the febrile stage is often complicated by gastrointestinal symptoms like vomiting and anorexia, which can sometimes mask the classic clinical picture seen in adults, making early diagnosis challenging [35]. Based on the fever’s degree, bradycardia is expected [36].
Hematologic studies during this phase often reveal characteristic changes, including thrombocytopenia, hyponatremia, elevated liver enzymes, and leukopenia, which, when interpreted alongside clinical features such as fever and rash, bolster the diagnostic suspicion of dengue [37]. Complications such as dehydration, febrile seizures, and neurological manifestations, including encephalitis and aseptic meningitis, may occur [38]. During the acute febrile period, dengue viruses circulate in the peripheral blood, potentially infecting other mosquitoes 2 days before the fever onset and 5 days after [39]. The virus spreads systemically over 8-12 days. After this incubation period, the virus can be transmitted to humans by subsequent mosquito bites [40]. Adults are more commonly affected by classic dengue fever than children. Management of the febrile phase involves supportive care, including hydration, rest, and antipyretics to manage fever and pain [41]. This phase lays the groundwork for subsequent stages of the disease, and its proper recognition is crucial for effective monitoring and timely supportive intervention [35].
Critical or leakage phase
In children, the leakage phase begins following the febrile phase, marking the onset of the critical phase, usually between 3 and 7 days of fever, around the time of defervescence, and lasts 24-48 hours. There is a marked increase in capillary permeability, leading to plasma leakage into interstitial spaces. Children in this phase may also experience intense abdominal pain and persistent vomiting (>3 times in one hour or >4 times in 6 hours), which serve as warning signs of imminent circulatory compromise and possible shock [31].
The critical phase is characterized by a fluid shift, resulting in thrombocytopenia following leukopenia, hemoconcentration, and hematocrit (HCT) elevation, along with clinical signs such as narrowing of pulse pressure, tachycardia, cool or clammy extremities, and, in some cases, altered consciousness [42]. Approximately 1-2 days following defervescence, a generalized maculopapular morbilliform rash appears, sparing the palms and soles, and disappears within 1-5 days [41]. In some cases, extremity edema and desquamation may occur [43]. During the second rash period, fever may recur, indicating a biphasic fever pattern [41]. Coagulation disorders, including gastrointestinal bleeding, menorrhagia, and bleeding from some organs, are reported following dengue fever outbreaks [43]. Given that pediatric patients often have less robust compensatory mechanisms compared to adults, prompt recognition and aggressive, tailored fluid management are essential to prevent further deterioration. Intravenous fluids and electrolytes may be necessary, especially if there are signs of shock or severe dehydration. Hospitalization is often required during this phase to manage symptoms and prevent complications [44]. Careful monitoring, with frequent assessments of vital signs, fluid balance, and laboratory markers, is important to direct timely intervention and improve outcomes in this vulnerable population [33].
In most cases, plasma leakage results in minimal or transient circulatory changes. However, in severe cases, this condition can lead to shock, organ failure, and disseminated intravascular coagulation, characterized by increased activated partial thromboplastin time and decreased fibrinogen levels. Major complications include severe hemorrhage and encephalopathy [45]. Also, large pleural effusions and ascites can cause respiratory distress. Other potential complications include hypervolemia, congestive heart failure, acute pulmonary edema, ischemic hepatitis, and hepatic encephalopathy [46].
Convalescence phase
The convalescence phase of dengue fever in children marks the recovery period following the resolution of the critical leakage phase. During this stage, which begins 2 to 3 days after defervescence, patients experience gradual improvement in clinical status, with stabilization of vital signs, resolution of gastrointestinal symptoms, and normalization of hematological parameters such as platelet count and HCT [44]. After the critical phase, extravascular fluid is gradually reabsorbed during recovery [47]. The patient remains hemodynamically stable and diuresis, although general weakness and fatigue can persist for several weeks. Clinical manifestations in this phase include a transient rash with small circular islands of unaffected skin, known as “white islands in a sea of red” [23]. Bradycardia and electrocardiographic changes are frequently observed. HCT levels stabilize or slightly decrease due to hemodilution, while leukocytosis and thrombocytosis may occur [44]. Supportive care during this period focuses on nutritional rehabilitation, hydration, gradual resumption of physical activity, and continued monitoring to ensure complete recovery and to rule out any late complications [23].
Dengue case classification
In 1997, World Health Organization (WHO) classified dengue infection into asymptomatic (95% of cases) and symptomatic infection, including dengue fever, dengue hemorrhagic fever (DHF), and DSS. Dengue fever is the milder form, characterized by high fever, rash, and muscle and joint pain. DHF is a more severe manifestation of the disease, involving bleeding, plasma leakage, and thrombocytopenia. DHF is categorized into four distinct grades [28, 48]: Grade I presented with fever, rash, and minor bleeding; grade II presented with spontaneous bleeding, positive tourniquet test, and low platelets; grade III characterized with signs of circulatory failure such as weak pulse, cold clammy skin, and restlessness; and grade IV characterized with severe circulatory failure leading to shock (DSS). The most severe form of dengue is known as DSS, characterized by profound shock with a rapid drop in blood pressure, leading to organ failure and potentially death [49].
WHO introduced the term “expanded dengue syndrome” (EDS) for cases that do not meet the criteria for DHF or DSS but exhibit abnormal manifestations in various organs, including the cardiovascular, nervous, renal, gastrointestinal, and hematological systems. These unusual manifestations have been increasingly reported and are collectively referred to as EDS. According to the WHO 2009 definition, dengue is classified into three main categories to facilitate clinical management: dengue without warning signs, dengue with warning signs, and severe dengue [32, 48] (Table 2).
Recently, the centers for disease control and prevention (CDC) categorized dengue infections into dengue, dengue-like illness, and severe dengue. Dengue-like illness, characterized by fever, has been added to the list of notifiable infectious conditions [23].
DHF, DSS, and severe dengue
The WHO’s criteria for diagnosing DHF encompass the following items: fever; minor or major hemorrhagic manifestations, including a positive tourniquet test and thrombocytopenia (≤100000 /μL); and increased capillary permeability signs (HCT≥20%), pleural effusion, ascites, or hypoalbuminemia [28]. Identifying warning signs in an individual suspected of having dengue may indicate a need for hospitalization [32].
In severe dengue, increased vascular permeability leads to significant plasma leakage, which can cause hypotension, circulatory collapse, and organ dysfunction [29, 46]. The incubation period of severe dengue and dengue fever is similar. However, the progression of the illness has unique characteristics in infants and children [50].
There is a sudden onset of fever in the initial phase of dengue fever, followed by malaise, vomiting, headache, loss of appetite, abdominal pain, and upper respiratory symptoms, which may progress within 2 to 5 days [51]. Around the time of defervescence, symptoms such as cold extremities, slow capillary filling, warm trunk, facial flushing, cyanosis, sweating, irritability and restlessness, abdominal pain, oliguria, and hypovolemia may appear [52]. Forehead and extremities petechiae, spontaneous ecchymosis, and easy bruising and bleeding at venipuncture sites are common [51]. Tachypnea, tachycardia, and weak heart sounds may also be observed. Systolic pressure may remain stable or even increase initially; however, once hypotension develops, both systolic and diastolic pressures may drop to low or unmeasurable levels, potentially resulting in irreversible shock and fatality despite intensive resuscitation measures [52]. Firm and tender hepatomegaly, 4-6 cm below the costal margin, may occur [51].
Right unilateral or bilateral pleural effusions are the most common ultrasonographic indicator of plasma leakage on chest radiographs. Thickening of the gallbladder wall and ascites are less frequently detected and resolve more quickly than pleural effusions [53]. Up to 10% of patients may experience gross ecchymosis or gastrointestinal bleeding. Clinicians must be vigilant for warning signs during the shift from the febrile to the critical phase [52]. In children who recover, convalescence is usually rapid within 24-36 hours. The body temperature might normalize before or during the shock stage. It is important to note that dengue vascular permeability syndrome frequently occurs in infants aged 5 to 10 months in regions where multiple dengue virus strains are hyper-endemic. These infants are born to mothers with two or more lifetime dengue infections, making diagnosis more challenging and resulting in higher fatality rates [51].
Diagnosis
Diagnosis of dengue fever in children is a multifaceted process that relies on clinical evaluation, specific laboratory tests, and consideration of the geographic distribution to distinguish it from other febrile illnesses. Clinically, children may present with high fever, headache, myalgia, and a rash. Still, the onset can be more subtle than in adults, often accompanied by gastrointestinal symptoms such as nausea or abdominal pain [48].
DSS and DHF have similar diagnostic criteria, including hypotension, tachycardia, narrow pulse pressure (≤20 mmHg), and cold extremities. To confirm the diagnosis early in the febrile phase, clinicians frequently use virologic tests, including serologic tests, serum virus isolation, and detection of dengue virus viral RNA or non-structural protein 1 (NS1) [54]. Serologic diagnosis relies on a ≥4-fold increase in antibody titer, and IgM/IgG antibody detection confirms the infection [55].
In both primary and secondary infections, after 5 days, IgM antibodies are detected and typically disappear within 60 days (sensitivity: 61.5-100%; Specificity: 52-100%). Rapid IgM test strips, which have lower sensitivity, can also be used within the same duration. IgG antibody concentrations rise in secondary infection and are detectable 10 days following symptom onset in primary infection and 3 days following symptoms in secondary infection (Sensitivity: 46.4-99%; Specificity: 80%-100%). Consequently, during the initial 5 days of symptoms, IgM and IgG tests are typically negative [28].
The IgM/IgG ratio is >1.2 in primary infection and <1.2 in secondary infection. These proportions can vary based on the disease type. Point-of-care tests using IgM-capture ELISA and NS1 detection are available to diagnose acute infections, particularly useful from the third day of infection up to the seroconversion period, which can extend to 14 days (Sensitivity: 89.9-92.9%; Specificity: 75-100%). NS1 and IgM/IgG combo kits work similarly. If both NS1 and IgM are non-reactive while IgG is reactive, it indicates a secondary infection (Sensitivity: 93%; Specificity: 100%) [48]. Viral detection tests, including cell culture, RT-PCR of the RNA, and NS1, detect viral RNA from 1-5 days after symptom onset in primary infections and 1-4 days in secondary infections (Sensitivity: 40.5%; Specificity: 100%) [33] (Figure 1).
Differential Diagnosis
In children, the differential diagnosis of dengue virus infection is broad due to its clinical features overlapping with those of several other infectious diseases [56]. During the febrile phase, the differential diagnosis should include other arboviral infections, such as measles, rubella, enteroviruses, and adenoviruses, as well as influenza. Additionally, bacterial infections like leptospirosis or sepsis can mimic dengue, especially when gastrointestinal symptoms and hemorrhagic signs occur [52].
Febrile children presenting with rash and myalgia may also be evaluated for viral illnesses, such as chikungunya, measles, rubella, or erythema infectiosum, which can present with fever and rash. However, joint pain is more prominent with chikungunya [57].
In areas where multiple arboviruses might be endemic, O’nyong-nyong fever, West Nile fever, Oropouche, and Zika should be considered. Colorado tick fever, sandfly fever, Ross River fever, and mild Rift Valley fever are similar to DHF but do not present with rash. Malaria is the most common nonviral acute infectious disease that resembles DHF [57].
Diagnosis of dengue, chikungunya, and Zika is primarily clinical. Chikungunya is frequently observed in the same populations. It produces a dengue fever-like syndrome with a more abrupt onset and shorter duration as well as more frequent maculopapular rash, conjunctivitis, and myalgia or arthralgia [58].
Laboratory evaluation, including tests for the NS1 antigen, RT-PCR, and subsequent IgM/IgG serology, along with hematological findings like thrombocytopenia and hemoconcentration, is essential to distinguish dengue from these other entities [47].
Prevention and Vector Control
Based on the biology, ecology, and behaviour of A. aegypti and A. albopictus, as well as the epidemiology of the diseases they transmit, WHO has developed many strategic approaches to control these mosquito vectors. These strategies aim to prevent their establishment and distribution, as well as control epidemics [59].
Methods to prevent mosquito bites
Personal protection measures include wearing long protective clothing and sleeping under mosquito nets, especially for infants and young children, to minimize skin exposure. Additionally, applying repellents containing DEET, picaridin, IR 3535, and lemon eucalyptus oil to exposed skin and staying indoors during peak mosquito activity at dawn and dusk are effective prevention methods [20].
Home and Environment
Prophylaxis includes killing vector mosquitoes, avoiding mosquito bites, and solid waste management [28]. Control efforts should focus on the most productive and epidemiologically important habitats. These measures include eliminating standing water by removing stagnant areas where mosquitoes can breed, such as flowerpots, buckets, and old tires, and setting up mosquito traps around the home to reduce the mosquito population. Installing window and door screens to keep mosquitoes out and using indoor insecticides to eliminate mosquitoes in the home are also effective measures [54].
Community engagement
Community engagement is crucial for dengue prevention, as it involves educating residents about the Aedes mosquito’s life cycle and eliminating breeding sites through regular cleanup campaigns and source-reduction efforts. By promoting insect repellents, bed nets, and monitoring systems, communities can protect themselves from mosquito bites and swiftly report potential outbreaks. Collaboration with local authorities and training community health workers further enhances the effectiveness of vector control measures, fostering a proactive, united approach to reducing dengue transmission. Research and development of novel control strategies, including Wolbachia, sterile insect technique, and genetically modified mosquitoes, should also be promoted and funded [59-61].
As Iran is not yet in a hyperendemic area for dengue, vaccine administration is not currently warranted. In the absence of a viable dengue vaccine for Iran, a multifaceted integrated vector management strategy emerges as both feasible and urgently needed. Alternative approaches include deploying biological controls, such as releasing Wolbachia-infected Aedes mosquitoes, which interfere with the virus’s replication and naturally reduce the vector population over successive generations [62]. Alongside these measures, environmentally focused approaches, such as the use of plant-based larvicides and community-led initiatives to eliminate or manage breeding sites, promise a sustainable reduction in mosquito density while mitigating concerns about chemical insecticide resistance [63]. Moreover, innovative genetic methods such as gene-drive strategies and sterile insect techniques offer potential for long-term suppression of vector populations. However, they require rigorous field evaluation to ensure safety and effectiveness [62].
Vaccination
Currently, there are two licensed dengue vaccines. Dengvaxia (CYD-TDV), a live recombinant tetravalent vaccine developed by Sanofi Pasteur, has received FDA approval and integrates the structural regions of the four DENV serotypes. It is approved for use in 16 countries and is administered as a series of three doses, with each dose spaced 6 months apart. The vaccine is recommended for individuals aged 9-45 years (or 9-60 years, depending on country-specific regulatory approvals) who have had a prior dengue infection. WHO does not recommend it for patients with negative serum. Pre-vaccination screening for previous dengue infection is required [64]. A large, well-designed, multi-country clinical trial of Dengvaxia shows that nearly all vaccinated individuals develop tetravalent neutralizing antibodies [65].
Developed by Takeda and designed by the CDC, Qdenga (TAK-003) is a live-attenuated vaccine composed of weakened dengue virus serotypes 1-4. It is used as a 2-dose series with a 3-month interval and is recommended for children aged 6-16 years in areas with high dengue transmission. In clinical trials, vaccinated seronegative individuals showed positive outcomes [65, 66].
Current dengue fever management in Iran
Iran’s current dengue fever management policies emphasize vector control, capacity building, and intersectoral collaboration in efforts to curb disease transmission, as outlined in recent national systematic reviews [59]. However, compared with the WHO guidelines, which emphasize integrated surveillance, early case detection, standardized diagnostic protocols, and rigorous clinical management, especially for severe dengue, the Iranian approach appears less comprehensive and less uniformly implemented [32, 67]. While endemic countries have refined their strategies by establishing robust early warning systems and optimizing fluid management protocols to reduce mortality, Iran’s policies still face challenges, including gaps in rapid-response mechanisms and inconsistent clinical practices across regions. Strengthening these areas and aligning more closely with WHO standards could enhance the overall effectiveness of dengue management in Iran, particularly as the threat of local transmission escalates.
Treatment and Disease Management
Treatment for dengue is supportive, including bed rest, antipyretics, analgesics, sedation, and fluid and electrolyte replacement therapy [32] (Table 3).
Aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) should be avoided because they increase the risk of Reye’s syndrome and dengue hemorrhagic disease. Corticosteroids are not routinely indicated due to their adverse effects [65]. A baseline HCT should be checked.
Patients with mild DHF or warning signs
Blood pressure below 90/60 mmHg, HCT greater than 50%, thrombocytopenia (PLT<50000/mm³), and evidence of bleeding other than petechiae are key indicators [28]. Oral fluid intake, such as fruit juice and electrolyte and dextrose solutions, is essential and preferred over plain water. Salicylates should be avoided for fever control due to the risk of bleeding and acidosis. Administer acetaminophen at the following doses: Less than 1 year, 60 mg; 1-3 years, 60-120 mg; 3-6 years, 120 mg; and 6-12 years, 240 mg [68].
DHF (compensated shock)
Critical care management of vascular permeability is necessary for patients with compensated shock. Shock may develop in approximately one-third of patients, making a baseline hemoglobin measurement essential [28]. Close observation for signs of bleeding and circulatory compromise, along with prompt supportive treatment, is crucial in the management of the patients, as the severity of shock may change within 48 hours. Volume depletion is often a consequence of fever, inadequate oral intake, bleeding, and plasma leakage [53].
Intravenous fluid resuscitation with an isotonic crystalloid solution at a rate of 5-10 mL/kg/h over 1 hour is recommended. However, this must be carefully adjusted to maintain adequate circulation, as serious complications such as pulmonary edema and respiratory failure may occur due to excessive fluid administration [53].
If the patient’s condition improves, gradually reduce intravenous fluids to 5-7 mL/kg/h for 1-2 hours, followed by 3-5 mL/kg/h for 2-4 hours, and then to 2-3 mL/kg/h, adjusting further based on hemodynamic status. If vital signs remain unstable after the initial bolus, check the HCT. If it increases or is > 50%, infuse a second bolus at 10-20 mL/kg/h for 1 hour. If there is improvement after the second bolus, reduce the rate to 7-10 mL/kg/h for 1-2 hours. If the HCT decreases from the baseline level, significant hemorrhage may be present, and a blood transfusion may be necessary. Additional boluses of crystalloid solutions might be necessary over the following 1-2 days [25, 69].
DSS
In cases of shock, crystalloid fluid is administered as a bolus of 10-20 mL/kg over 15 minutes to maintain blood pressure [33], and, in cases with poor response, colloid fluid is administered [53]. If the patient’s condition improves, continue the crystalloid/colloid infusion at 10 mL/kg/h for 1 hour. Subsequently, continue the infusion and slowly reduce the rate to 5-7 mL/kg/h for 1-2 hours, then to 3-5 mL/kg/h for 2-4 hours, and finally to 2-3 mL/kg/h or less, which can be maintained for up to 24 to 48 hours. A common question for healthcare personnel managing dengue patients is whether to transfuse platelet products [33]. Bleeding tendency and platelet counts are not always correlated and can be present in children with normal platelet counts [70]. This condition underscores the need to clarify the indications for platelet transfusion in thrombocytopenic dengue patients without overt hemorrhage [33].
If vital signs are unstable, the first HCT determines the need for a blood transfusion. In cases with HCT above baseline, a second bolus of colloid at 10-20 mL/kg/h is administered within 30 minutes to 1 hour, and the patient is reassessed. After improvement, reduce the rate to 7-10 mL/kg/h for 1-2 hours, then replace it with a crystalloid solution and gradually reduce the infusion rate. If the condition remains unstable after the second bolus, recheck the HCT and transfuse blood if it decreased. If it has elevated or remains very high, infuse colloid solutions at 10-20 mL/kg/h as a third bolus over 1 hour and then reduce the rate to 7-10 mL/kg/h for 1-2 hours, then return to a crystalloid solution and gradually reduce the infusion rate. Additional boluses might be required over the following 24 hours [32].
In unresponsive shock patients, up to 40-60 mL/kg of fluid, 5-10 mL/kg of fresh red blood cells, or 10-20 mL/kg of fresh whole blood should be transfused, especially in the presence of severe bleeding. If the equipment is available, place an arterial catheter for frequent blood pressure monitoring and blood sampling. It is important to monitor EKG and pulse oximetry, and to check urine output and HCT (before and after administering fluid boluses, and then every 4-6 hours). Also, arterial or venous blood gases, lactate, total CO2 and HCO3, and blood glucose levels should be checked every 30 minutes to 1 hour until stable. Patients with prolonged, refractory, or hypotensive shock, renal or liver insufficiency, persistent metabolic acidosis, preexisting peptic ulcer disease, trauma, or those treated with nonsteroidal anti-inflammatory or anticoagulant agents are at high risk for hemorrhage [25].
Discharge Criteria
Patients with dengue who do not exhibit warning signs, tolerate adequate oral fluids, urinate at least once every 6 hours, and do not have associated diseases, chronic conditions, or social risk factors can be discharged with supportive treatment. Also, those with improved appetite, normal vital signs and breathing, no evidence of bleeding, increased platelet counts, and stable HCT can be discharged. They should be followed up on every 24–48 hours until they have been afebrile for 48 hours [71].
These patients should have normal or near-normal hemoglobin/HCT and platelet levels. They should not have concurrent conditions as mentioned in Table 3. Fever management should involve acetaminophen, and aspirin and NSAIDs should be avoided [33].
Social and Psychological Challenges
Dengue fever can significantly impact both children and their families psychologically and socially. Children may experience anxiety, fear, and stress due to the illness and its symptoms, which can affect their emotional well-being and academic performance. Families may face social isolation as they make an effort to prevent the spread, and caregivers often experience stress and anxiety from the added responsibilities and financial burden of medical care. Overall, the impact can lead to a decreased quality of life and increased emotional strain on the entire family [72].
Education and Awareness in Children
Educating children about dengue and raising awareness are crucial to preventing its spread. Effective strategies include school-based programs with interactive lessons, role-playing, demonstrations, and field activities to identify and eliminate mosquito breeding sites. Educational materials such as posters, charts, board games, activities, storybooks, and comics can also convey key messages [73]. Community involvement through parental engagement, community cleanup campaigns, and participation in public health initiatives is essential. Additionally, digital tools such as educational apps and social media can be used to share educational content. Health-promoting schools can provide health kits and train teachers to deliver dengue prevention education effectively. By implementing these strategies, children can learn to protect themselves and their communities from dengue [34].
Follow-up
Follow-up care for children recovering from dengue fever involves regular check-ups to monitor progress, track vital signs, and perform blood tests. Symptom management includes providing pain relief, ensuring hydration, and encouraging rest. Educating parents about the warning signs of severe dengue and encouraging them to seek immediate medical care is crucial. During the recovery phase, children should gradually return to activities and maintain a balanced diet. It is also important to emphasize mosquito bite prevention measures to prevent reinfection [26].
Conclusion
The establishment of A. aegypti in southern Iran and the increasing presence of A. albopictus in the north heralds a pivotal shift in the epidemiology of dengue fever, particularly affecting pediatric populations. Given that children are highly vulnerable to severe dengue manifestations and account for approximately one-fifth of all infections in Iran, they represent a significant at-risk demographic that warrants specific public health and clinical consideration. This review highlights how children often present with atypical manifestations, such as prominent abdominal pain, vomiting, rash, and a rapid progression to vascular leakage and shock, which differ markedly from adult presentations. These nuances underscore the need for pediatric-specific case management protocols emphasizing early recognition and aggressive intervention. Moreover, given the dynamic spread of the disease, control strategies must combine targeted vector control and ongoing, specialized education for healthcare providers to ensure timely, effective responses in clinical settings. For these initiatives to succeed, robust national policies underscored by strong political will and intersectoral collaboration are essential.
Future research must prioritize well-designed, multicenter epidemiological studies and randomized controlled trials with a focus on refining pediatric guidelines for early diagnostic and prognostic biomarkers, evaluating tailored fluid management and treatment regimens, and assessing the efficacy, safety, and optimal dosing of emerging vaccines specifically in pediatric populations to reduce dengue morbidity and mortality among Iran’s most vulnerable populations.
Ethical Considerations
Compliance with ethical guidelines
This article is a narrative review, with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank the Iran Centers for Disease Control and Prevention (CDC) and the Ministry of Health and Medical Education for providing national epidemiological data and official statistics that contributed to this narrative review.
References
- Moniruddin A. Alarming trends of Dengue in 2023. KYAMC J. 2023; 14(02):62-3. [DOI:10.3329/kyamcj.v14i02.68523]
- Abbasi E. Aedes aegypti and dengue: Insights into transmission dynamics and viral lifecycle. Epidemiol Infect. 2025; 153:e88. [DOI: 10.1017/S0950268825100320] [PMID]
- Heydarifard Z, Heydarifard F, Mousavi FS, Zandi M. Dengue fever: A decade of burden in Iran. Front Public Health. 2024; 12:1484594. [DOI:10.3389/fpubh.2024.1484594] [PMID]
- Wilson-Bahun TA, Kamgang B, Lenga A, Wondji CS. Larval ecology and infestation indices of two major arbovirus vectors, Aedes aegypti and Aedes albopictus (Diptera: Culicidae), in Brazzaville, the capital city of the Republic of the Congo. Parasit Vectors. 2020; 13:1-18. [DOI:10.1186/s13071-020-04374-x] [PMID]
- Muktar Y, Tamerat N, Shewafera A. Aedes aegypti as a Vector of Flavivirus. J Trop Dis. 2016; 4(223):2. [DOI:10.4172/2329-891X.1000223]
- Diniz LMO, de Castro Romanelli RM, Bentes AA, da Silva NLC, Cruzeiro FRS, Marcial TM, et al. Yellow fever in children and adolescents previously immunized in Minas Gerais State, Brazil. Vaccine. 2020; 38(44):6954-8. [DOI:10.1016/j.vaccine.2020.08.042] [PMID]
- Gardner CL, Ryman KD. Yellow fever: A reemerging threat. Clin Lab Med. 2010; 30(1):237-60. [DOI:10.1016/j.cll.2010.01.001] [PMID]
- Balmaseda A, Gordon A, Gresh L, Ojeda S, Saborio S, Tellez Y, et al. Clinical attack rate of chikungunya in a cohort of Nicaraguan children. Am J Trop Med Hygiene. 2016; 94(2):397. [DOI:10.4269/ajtmh.15-0413] [PMID]
- Naik KD, Delhi Kumar C, Abimannane A, Dhodapkar R, Biswal N. Chikungunya infection in children: clinical profile and outcome. J Trop Pediatr. 2025; 71(1):fmae057. [DOI:10.1093/tropej/fmae057] [PMID]
- Sutaria AH, Solanki KM. Fever with rash in an adult patient. In: Padhiyar J, Patel N, editors. Approach and observation in clinical dermatology. New Delhi: Jaypee Brothers Medical Publishers Pvt Limited; 2023. [Link]
- Kimata YM. Prevalence and distribution of Dengue, Chikungunya and Zika Arboviruses among non-measles febrile rash cases in selected regions of Kenya: 2008-2014. Juja: Jomo Kenyatta University of agriculture and technology; 2022. [Link]
- Uncini A, Shahrizaila N, Kuwabara S. Zika virus infection and Guillain-Barré syndrome: A review focused on clinical and electrophysiological subtypes. J Neurol Neurosurg Psychiatry. 2017; 88(3):266-71. [DOI:10.1136/jnnp-2016-314310] [PMID]
- Freitas DA, Souza-Santos R, Carvalho LMA, Barros WB, Neves LM, Brasil P, et al. Congenital Zika syndrome: A systematic review. PLoS One. 2020; 15(12):e0242367. [DOI:10.1371/journal.pone.0242367] [PMID]
- Martelli CMT, Cortes F, Brandão-Filho SP, Turchi MD, Souza WVd, Araújo TVBd, et al. Clinical spectrum of congenital Zika virus infection in Brazil: Update and issues for research development. Rev Soc Bras Med Trop. 2024; 57:e00301-2024. [DOI:10.1590/0037-8682-0153-2024] [PMID]
- Major CG, Paz-Bailey G, Hills SL, Rodriguez DM, Biggerstaff BJ, Johansson M. Risk estimation of sexual transmission of Zika virus-United States, 2016-2017. J Infect Dis. 2021; 224(10):1756-64. [DOI:10.1093/infdis/jiab173] [PMID]
- Kharwadkar S, Herath N. Clinical manifestations of dengue, Zika and chikungunya in the Pacific Islands: A systematic review and meta-analysis. Rev Med Virol. 2024; 34(2):e2521. [DOI:10.1002/rmv.2521] [PMID]
- Ojianwuna C, Enwemiwe V. Water closets as breeding sites for Aedes mosquitoes in dry seasons. Niger J Parasitol. 2022; 43(1). [DOI:10.4314/njpar.v43i1.19]
- Reiner Jr RC, Stoddard ST, Scott TW. Socially structured human movement shapes dengue transmission despite the diffusive effect of mosquito dispersal. Epidemics. 2014; 6:30-6. [DOI:10.1016/j.epidem.2013.12.003] [PMID]
- Paul KK, Macadam I, Green D, Regan DG, Gray RT. Dengue transmission risk in a changing climate: Bangladesh is likely to experience a longer dengue fever season in the future. Environ Res Lett. 2021; 16(11):114003. [DOI:10.1088/1748-9326/ac2b60]
- Islam MT, Quispe C, Herrera-Bravo J, Sarkar C, Sharma R, Garg N, et al. Production, transmission, pathogenesis, and control of dengue virus: A literature-based undivided perspective. BioMed Res Int. 2021; 2021(1):4224816. [DOI:10.1155/2021/4224816] [PMID]
- Brar R, Sikka P, Suri V, Singh MP, Suri V, Mohindra R, et al. Maternal and fetal outcomes of dengue fever in pregnancy: A large prospective and descriptive observational study. Arch Gynecol Obstet. 2021; 304:91-100. [DOI:10.1007/s00404-020-05930-7] [PMID]
- Chong V, Tan JZL, Arasoo VJT. Dengue in pregnancy: A southeast asian perspective. Trop Med Infect Dis. 2023; 8(2):86. [DOI:10.3390/tropicalmed8020086] [PMID]
- National Notifiable Diseases Surveillance System (NNDSS) Dengue Virus Infections 2015 Case Definition. Canberra: NNDSS; 2021. [Link]
- Vasilakis N, Cardosa J, Hanley KA, Holmes EC, Weaver SC. Fever from the forest: Prospects for the continued emergence of sylvatic dengue virus and its impact on public health. Nat Rev Microbiol. 2011; 9(7):532-41. [DOI:10.1038/nrmicro2595] [PMID]
- Paz-Bailey G, Adams LE, Deen J, Anderson KB, Katzelnick LC. Dengue. Lancet. 2024; 403(10427):667-82. [DOI:10.1016/S0140-6736(23)02576-X] [PMID]
- Yousuf R, Salam MW, Akter S, Sinha S, Haque M. Dengue dynamics: A global update. Adv Human Bio. 2024; 14(1):5-10. [DOI: 10.4103/aihb.aihb_135_23]
- Sinha B, Goyal N, Kumar M, Choudhary A, Arya A, Revi A, et al. Incidence of lab-confirmed dengue fever in a pediatric cohort in Delhi, India. PLOS Negl Trop Dis. 2022; 16(4):e0010333. [DOI:10.1371/journal.pntd.0010333] [PMID]
- World Health Organization. Dengue haemorrhagic fever: Diagnosis, treatment, prevention and control. Geneva: World Health Organization; 1997. [Link]
- Karami H, Salehi-Vaziri M. Dengue fever in Iran: An emerging threat requiring urgent public health interventions. New Microbes New Infect. 2024; 62:101535. [DOI:10.1016/j.nmni.2024.101535] [PMID]
- Abbasi M, Yousefi S, Khayatzadeh S, Azarmi S, Normandipour F. Detection of invasive Aedes mosquitoes (Diptera: Culicidae): A crucial alert for public health in Northwest of Iran. Arch Public Health. 2025; 83(1):288. [DOI: 10.1186/s13690-025-01763-5] [PMID]
- Pothapregada S, Kamalakannan B, Thulasingam M. Clinical profile of atypical manifestations of dengue fever. Indian J Pediatr. 2016; 83:493-9. [DOI:10.1007/s12098-015-1942-9]
- World Health Organization. Dengue: Guidelines for diagnosis, treatment, prevention and control. Geneva: World Health Organization; 2009. [Link]
- Tayal A, Kabra SK, Lodha R. Management of dengue: An updated review. Indian J Pediatr. 2023; 90(2):168-77. [DOI:10.1007/s12098-022-04394-8] [PMID]
- Hadinegoro SRS. The revised WHO dengue case classification: Does the system need to be modified? Paediatr Int Child Health. 2012; 32(sup1):33-8. [DOI:10.1179/2046904712Z.00000000052] [PMID]
- Pan American Health Organization. Guidelines for the clinical diagnosis and treatment of dengue, chikungunya, and zika. Washington, D.C: Pan American Health Organization (PAHO); 2022. [Link]
- Fried JR, Gibbons RV, Kalayanarooj S, Thomas SJ, Srikiatkhachorn A, Yoon IK, et al. Serotype-specific differences in the risk of dengue hemorrhagic fever: An analysis of data collected in Bangkok, Thailand from 1994 to 2006. PLoS Negl Trop Dis. 2010; 4(3):e617. [DOI:10.1371/journal.pntd.0000617] [PMID]
- Salgado DM, Eltit JM, Mansfield K, Panqueba C, Castro D, Vega MR, et al. Heart and skeletal muscle are targets of dengue virus infection. Pediatr Infect Dis J. 2010; 29(3):238-42. [DOI:10.1097/INF.0b013e3181bc3c5b] [PMID]
- Puccioni-Sohler M, Rosadas C, Cabral-Castro MJ. Neurological complications in dengue infection: A review for clinical practice. Arq Neuro-Psiquiatr. 2013;71(9B):667-71. [DOI:10.1590/0004-282X20130147] [PMID]
- Gordon A, Kuan G, Mercado JC, Gresh L, Avilés W, Balmaseda A, et al. The Nicaraguan pediatric dengue cohort study: incidence of inapparent and symptomatic dengue virus infections, 2004-2010. PLoS Negl Trop Dis. 2013; 7(9):e2462. [DOI:10.1371/journal.pntd.0002462] [PMID]
- Rudolph KE, Lessler J, Moloney RM, Kmush B, Cummings DA. Incubation periods of mosquito-borne viral infections: a systematic review. Am J Trop Med Hyg. 2014; 90(5):882. [DOI:10.4269/ajtmh.13-0403] [PMID]
- Soman L. Fever with rashes. Indian J Pediatr. 2018; 85(7):528-34. [DOI:10.1007/s12098-017-2459-1] [PMID]
- Ranjit S, Kissoon N. Dengue hemorrhagic fever and shock syndromes. Pediatr Crit Care Med. 2011; 12(1):90-100. [DOI:10.1097/PCC.0b013e3181e911a7] [PMID]
- Tantawichien T. Dengue fever and dengue hemorrhagic fever in adults. Southeast Asian J Trop Med Public Health. 2015; 46 Suppl 1:79-98. [PMID]
- Kalayanarooj S. Clinical manifestations and management of dengue/DHF/DSS. Trop Med Health. 2011; 39(4SUPPLEMENT):S83-S7. [DOI:10.2149/tmh.2011-S10] [PMID]
- World Health Organization. Comprehensive guideline for prevention and control of dengue and dengue haemorrhagic fever. Geneva: World Health Organization; 2011. [Link]
- Rajapakse S, Rodrigo C, Rajapakse A. Treatment of dengue fever. Infect Drug Resist. 2012; 103-12. [DOI:10.2147/IDR.S22613] [PMID]
- Karyanti MR, Uiterwaal CSPM, Hadinegoro SR, Jansen MAC, Heesterbeek JAPH, Hoes AW, et al. Clinical course and management of dengue in children admitted to hospital; a 5 years prospective cohort study in Jakarta, Indonesia. Pediatr Infect Dis J. 2019. [DOI:10.1097/INF.0000000000002277] [PMID]
- Ang LW, Thein TL, Ng Y, Boudville IC, Chia PY, Lee VJM, et al. A 15-year review of dengue hospitalizations in Singapore: Reducing admissions without adverse consequences, 2003 to 2017. PLoS Negl Trop Dis. 2019; 13(5):e0007389. [DOI:10.1371/journal.pntd.0007389] [PMID]
- Umakanth M, Suganthan N. Unusual manifestations of dengue fever: A review on expanded dengue syndrome. Cureus. 2020; 12(9). [DOI:10.7759/cureus.10678]
- Lam PK, Tam DTH, Diet TV, Tam CT, Tien NTH, Kieu NTT, et al. Clinical characteristics of dengue shock syndrome in Vietnamese children: A 10-year prospective study in a single hospital. Clin Infect Dis. 2013; 57(11):1577-86. [DOI:10.1093/cid/cit594] [PMID]
- Halstead SB. Pathogenesis of dengue: Dawn of a new era. F1000Research. 2015; 4:F1000 Faculty Rev-353. [DOI:10.12688/f1000research.7024.1] [PMID]
- Simmons CP, Farrar JJ, van Vinh Chau N, Wills B. Dengue. N Eng J Med. 2012; 366(15):1423-32. [DOI:10.1056/NEJMra1110265] [PMID]
- Srikiatkhachorn A. Plasma leakage in dengue haemorrhagic fever. Thromb Haemost. 2009; 102(12):1042-9. [DOI:10.1160/TH09-03-0208] [PMID]
- Guzman MG, Harris E. Dengue. Lancet. 2015; 385(9966):453-65. [DOI:10.1016/S0140-6736(14)60572-9] [PMID]
- Blacksell SD, Jarman RG, Gibbons RV, Tanganuchitcharnchai A, Mammen Jr MP, Nisalak A, et al. Comparison of seven commercial antigen and antibody enzyme-linked immunosorbent assays for detection of acute dengue infection. Clin Vaccine Immunol. 2012; 19(5):804-10. [DOI:10.1128/CVI.05717-11] [PMID]
- Schaefer TJ, Panda PK, Wolford RW. Dengue fever [Internet]. 2024. [Updated 2026 February 2]. Available from: [Link]
- Paixão ES, Teixeira MG, Rodrigues LC. Zika, chikungunya and dengue: the causes and threats of new and re-emerging arboviral diseases. BMJ Glob Health. 2018 Jan 4;3(Suppl 1):e000530. [DOI:10.1136/bmjgh-2017-000530] [PMID]
- Ioos S, Mallet HP, Goffart IL, Gauthier V, Cardoso T, Herida M. Current Zika virus epidemiology and recent epidemics. Med Mal Infect. 2014; 44(7):302-7. [DOI:10.1016/j.medmal.2014.04.008] [PMID]
- Nikookar SH, Fazeli-Dinan M, Zaim M, Enayati A. Prevention and control policies of dengue vectors (Aedes aegypti and albopictus) in Iran. J Mazandaran Univ Med Sci. 2023; 33(227):381-96. [DOI:10.32598/ijhs.11.3.701.1]
- Fazeli-Dinan M, Nikookar SH, Azarnoosh M, Jafari A, Daneshpour E, Enayati A, et al. An overview of different control methods of invasive Aedes aegypti and Aedes albopictus. J Mazandaran Uni Med Sci. 2024;34(232):260-86. [Link]
- Zaim M, Enayati A, Sedaghat M, Gouya M. [Guidelines for prevention and control of Aedes aegypti and Aedes albopictus in Iran (Persian)]. Tehran: Iran Ministry of Health and Medical Education. 2020. [Link]
- Alkuriji MA, Al-Fageeh MB, Shaher FM, Almutairi BF. Dengue vector control: A review for Wolbachia-based strategies. Biosci Biotechnol Res Asia. 2020; 17(3):507-15. [DOI:10.13005/bbra/2854]
- Eisen L, Beaty BJ, Morrison AC, Scott TW. Proactive vector control strategies and improved monitoring and evaluation practices for dengue prevention. J Med Entomol. 2009; 46(6):1245-55. [DOI:10.1603/033.046.0601] [PMID]
- Getahun A, Batikawai A, Nand D, Khan S, Sahukhan A, Faktaufon D. Dengue in Fiji: Epidemiology of the 2014 DENV-3 outbreak. Western Pac surveill Response J. 2019; 10(2):31. [DOI:10.5365/wpsar.2018.9.3.001] [PMID]
- Hadinegoro SR, Arredondo-García JL, Capeding MR, Deseda C, Chotpitayasunondh T, Dietze R, et al. Efficacy and long-term safety of a dengue vaccine in regions of endemic disease. New Eng J Med. 2015; 373(13):1195-206. [DOI:10.1056/NEJMoa1506223] [PMID]
- Durbin AP, Whitehead SS. Next-generation dengue vaccines: Novel strategies currently under development. Viruses. 2011; 3(10):1800-14. [DOI:10.3390/v3101800] [PMID]
- Deen JL, Harris E, Wills B, Balmaseda A, Hammond SN, Rocha C, et al. The WHO dengue classification and case definitions: time for a reassessment. Lancet. 2006; 368(9530):170-3. [DOI:10.1016/S0140-6736(06)69006-5] [PMID]
- Zhang F, He J, Peng J, Tang X, Qin C, Lu H, et al. Guidelines for the diagnosis and treatment of dengue in China. Infect Dis Immun. 2021; 1(03):144-52. [DOI:10.1097/ID9.0000000000000026]
- Diana B, Yenny C, Carolina M, Esteban T, Emiro B. Fluid Management in Den-gue Critical Phase: Which, When, How Much. Int Arch Med Microbiol. 2022; 4:015. [DOI:10.23937/2643-4008/1710015]
- Pothapregada S, Kamalakannan B, Thulasingam M. Role of platelet transfusion in children with bleeding in dengue fever. J Vector Borne Dis. 2015; 52(4):304-8. [DOI:10.4103/0972-9062.172809] [PMID]
- Pajor MJ, Long B, Liang SY. Dengue: A focused review for the emergency clinician. Am J Emerg Med. 2024; 82:82-7. [DOI:10.1016/j.ajem.2024.05.022] [PMID]
- Schaber KL, Morrison AC, Elson WH, Astete-Vega H, Córdova-López JJ, Ríos López EJ, et al. The impact of dengue illness on social distancing and caregiving behavior. PLoS Negl Trop Dis. 2021; 15(7):e0009614. [DOI:10.1371/journal.pntd.0009614] [PMID]
- Heyrani A, Pourjalil F, Hosseini Z, Shahabi N, Asadipour E. A comprehensive scoping review of global educational strategies and outcomes in aedes-borne disease control. Arch Public Health. 2024; 82(1):1-28. [DOI:10.1186/s13690-024-01412-3] [PMID]
Type of Study: Review Article |
Subject:
Pediatric Infectious Diseases
Received: 2025/06/13 | Accepted: 2025/08/2 | Published: 2026/01/1
Received: 2025/06/13 | Accepted: 2025/08/2 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
