
Thu, Jul 23, 2026


Volume 14, Issue 1 (1-2026)
J. Pediatr. Rev 2026, 14(1): 87-92 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mollaeifard F, Mehrabani S, Esmaeili Dooki M, Mahmoodi-Nesheli H, Pornasrolah M, Esmaeilzadeh F. Uncommon Initial Symptoms in Pediatric Burkitt Lymphoma: Pancreatic and Mandibular Involvement. J. Pediatr. Rev 2026; 14 (1) :87-92
URL: http://jpr.mazums.ac.ir/article-1-726-en.html
URL: http://jpr.mazums.ac.ir/article-1-726-en.html
Fatemeh Mollaeifard1 

 , Sanaz Mehrabani *2 , Mohammadreza Esmaeili Dooki3 , Hassan Mahmoodi-Nesheli3 , Mohammad Pornasrolah4 , Firozeh Esmaeilzadeh1
, Sanaz Mehrabani *2 , Mohammadreza Esmaeili Dooki3 , Hassan Mahmoodi-Nesheli3 , Mohammad Pornasrolah4 , Firozeh Esmaeilzadeh1
, Sanaz Mehrabani *2 , Mohammadreza Esmaeili Dooki3 , Hassan Mahmoodi-Nesheli3 , Mohammad Pornasrolah4 , Firozeh Esmaeilzadeh1
1- Student Research Committee, Babol University of Medical Sciences, Babol, Iran.
2- Clinical Research Development Unit of Amirkola Children's Hospital, Babol University of Medical Sciences, Babol, Iran. ,mehrabanisanaz@gmail.com
3- Clinical Research Development Unit of Amirkola Children's Hospital, Babol University of Medical Sciences, Babol, Iran.
4- Non-Communicable Pediatric Diseases Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran.
2- Clinical Research Development Unit of Amirkola Children's Hospital, Babol University of Medical Sciences, Babol, Iran. ,
3- Clinical Research Development Unit of Amirkola Children's Hospital, Babol University of Medical Sciences, Babol, Iran.
4- Non-Communicable Pediatric Diseases Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran.
Full-Text [PDF 2038 kb]
(291 Downloads)
| Abstract (HTML) (697 Views)
Full-Text: (164 Views)
Introduction
Lymphomas are a heterogeneous group of lymphoid malignancies broadly classified into Hodgkin and non-Hodgkin lymphomas (NHL), with NHL being more prevalent worldwide and ranking as the 11th most common cancer [1, 2]. Burkitt lymphoma (BL), a highly aggressive B-cell lymphoma, predominantly affects children and adolescents [3]. The World Health Organization (WHO) recognizes three subtypes: Endemic (linked to malaria and Epstein-Barr virus in equatorial regions), immunodeficiency-associated (often in HIV-positive patients), and sporadic (the most frequent form in Western countries) [4]. Sporadic BL accounts for about 30% of pediatric lymphomas, typically presenting around age 10, and usually involves lymph nodes, abdomen, bone marrow, or facial bones [5].
Pancreatic involvement is rare, especially in immunocompetent children. While pancreatitis is usually attributed to infection, trauma, or medications, its occurrence as an initial manifestation of BL emphasizes the need to consider malignancy in atypical pediatric presentations [6]. In this study, we present the case of an 11-year-old immunocompetent boy whose initial symptoms of BL was associated with acute pancreatitis and jaw pain. This rare presentation is particularly important, as it underscores the need to consider malignancy in atypical pediatric pancreatitis cases.
Case Presentation
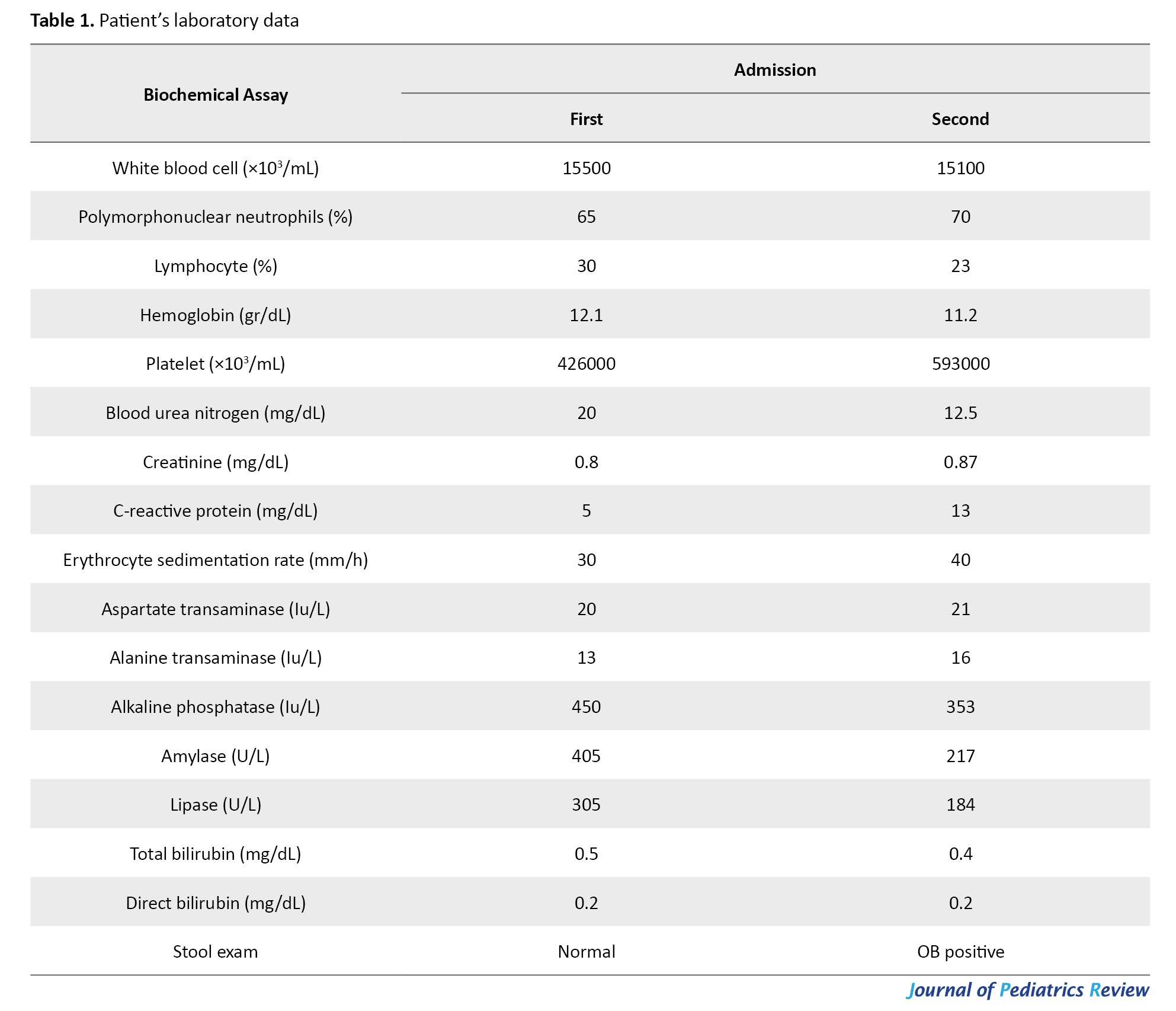
We report a 11-year-old boy with gastrointestinal discomfort. A medical history was obtained from his biological parents, and they provided informed consent for the reporting of his symptoms. He had 10 days of abdominal pain with nausea, vomiting, lethargy, and weakness. Notably, the intensity of the abdominal pain was not affected by food intake or defecation. The patient had no fever, respiratory symptoms, or recent dietary changes. The mother reported occasional constipation, but no other gastrointestinal concerns were noted. The patient had been briefly hospitalized for similar symptoms 2 days before this admission. Additionally, he reported dental pain. His past medical, surgical, and drug histories were unremarkable, and his developmental history was normal. However, his paternal uncle had been diagnosed with BL and had undergone a bone marrow transplant. On examination, his vital signs were within normal limits (Table 1); however, he exhibited signs of irritability and aggressive behavior.
Abdominal examination revealed mild periumbilical tenderness, while findings from other systems were unremarkable.
Given the patient’s presenting symptoms of nausea, vomiting, and abdominal pain, viral gastroenteritis was initially considered, based on which we initiated supportive treatment. Additionally, due to other possible diagnoses, we conducted further tests and evaluations. Diagnostic evaluations included laboratory and radiologic tests. Laboratory studies showed elevated amylase and lipase levels, suggesting acute pancreatitis. Radiological assessments, including a chest and abdominal x-rays, revealed mild fecal loading. Subsequently, an abdominal-pelvic ultrasound was performed, showing circumferential thickening and increased fat echogenicity around the descending colon, suggestive of infectious colitis. For a more detailed evaluation, a contrast-enhanced CT scan was conducted, revealing mild stranding and several lymph nodes in the transverse colon. The pancreas appeared enlarged with smooth borders. It contained at least 5 nodules with relatively well-defined margins and lower enhancement than the surrounding pancreatic tissue. These findings are most consistent with pancreatitis, particularly autoimmune pancreatitis or granulomatous disease such as sarcoidosis. Due to suspicion of autoimmune disease, ACE and IgG4 levels were checked and found within normal limits. Additionally, an ophthalmologic examination was performed to evaluate for possible uveitis.
However, the results were normal. After 7 days, he was discharged on antibiotics, pantoprazole, and probiotics. Recommendations included outpatient follow-up, with additional lab tests and a repeat abdominal-pelvic ultrasound to assess for a pancreatic pseudocyst. Outpatient referrals were made for a dental consultation to address persistent dental pain and a psychiatric consultation to evaluate and manage his irritability.
He was readmitted after 4 days due to recurrent symptoms. He presented with recurrent colicky abdominal pain centered in the epigastric and peri-umbilical regions. There was no fever or diarrhea; however, the patient reported reduced appetite, excessive sweating, and pain in the right jaw, along with noted dental decay. On initial examination, the patient’s vital signs were stable with a blood pressure of 110/60 mm Hg, a temperature of 36.7 °C, a pulse rate of 84 beats per minute, and a weight of 40 kg. There were no signs of fever or respiratory distress. Mild periumbilical tenderness was noted on abdominal examination, and the patient exhibited irritability and anxious behavior. No other significant findings were noted in the other systemic examinations. On physical examination, mild periumbilical tenderness and swelling of the right jaw were observed. Laboratory and imaging studies were conducted. Lab results showed elevated amylase and lipase levels (Table 1). Additionally, all other tests, including those for infectious causes (wright, coombs wright, widal, and PPD) were within normal limits. Based on these results, our initial diagnosis was acute pancreatitis. Sonography supported this diagnosis, revealing signs of acute pancreatitis without pseudocysts. An MRCP further confirmed pancreatitis, and an abdominal CT scan with IV contrast demonstrated pancreatic enlargement and decreased enhancement in the tail and body, along with mass-like thickening of the gastric fundus. Following our initial diagnosis of acute pancreatitis, supportive treatment was promptly initiated. Antibiotics were administered to address a suspected dental infection, and risperidone and sertraline were started to manage anxiety-related behaviors.
While our initial suspicion was focused on acute pancreatitis, additional findings warranted further investigation. Due to the jaw swelling, a sonographic evaluation was performed, revealing a hypoechoic structure adjacent to the bone between the ramus and angle. A subsequent head and neck CT scan, with and without contrast, suggested a potentially malignant soft tissue lesion near the mandible, showing destructive changes and erosion in the mandible, as well as similar changes in the zygoma and associated soft tissue lesions in both maxillary sinuses. These findings were indicative of maxillofacial lymphoma. During hospitalization, the patient also experienced episodes of coffee-ground vomiting, which prompted an endoscopy. As shown in Figure 1, this procedure identified a polypoid mass with ulceration in the gastric fundus.
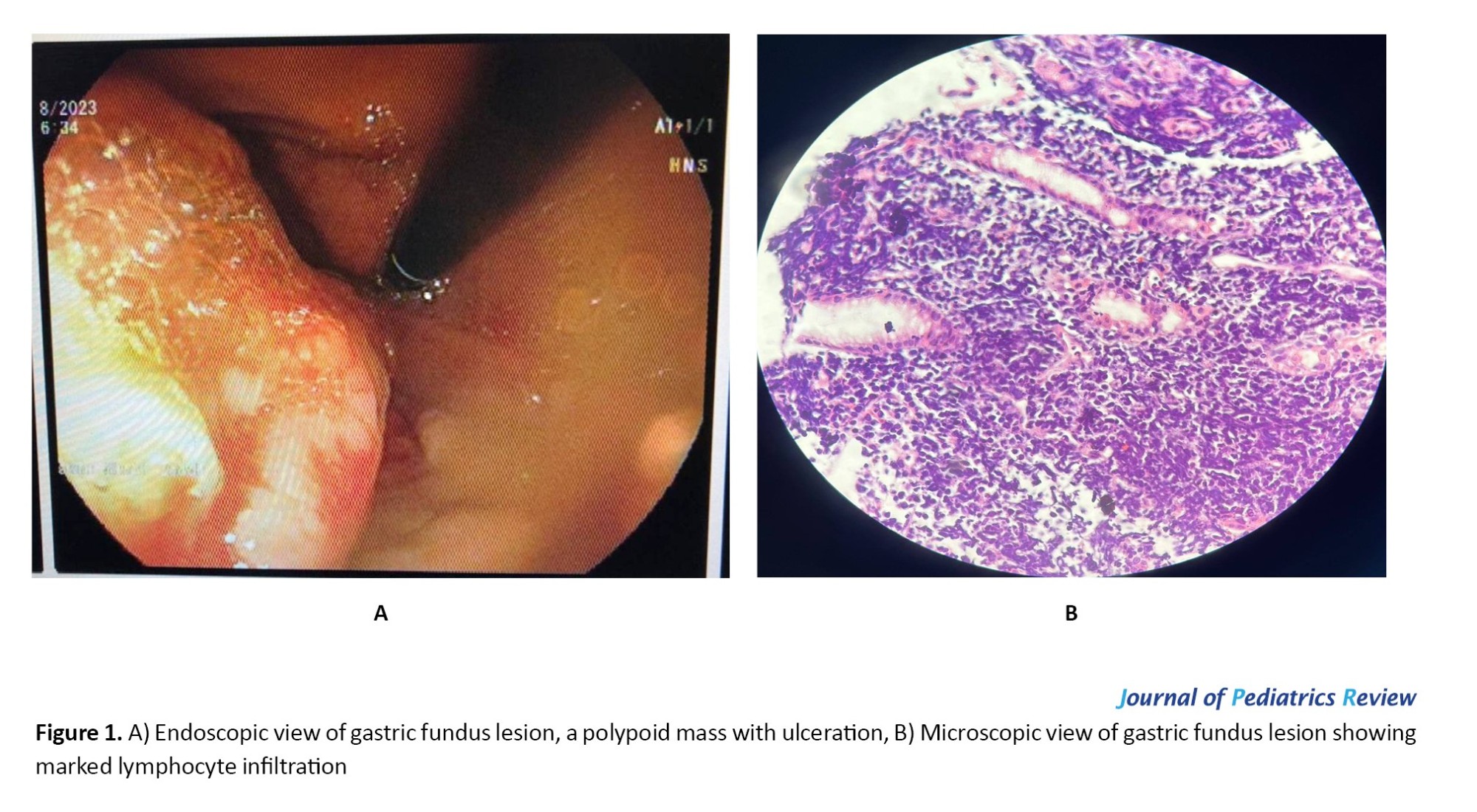 Pathological examination of the biopsy showed marked lymphocyte infiltration within the glands and lamina propria, with relatively monomorphic cells, some with prominent nucleoli, suggesting a small blue round cell tumor, likely lymphoma.
Pathological examination of the biopsy showed marked lymphocyte infiltration within the glands and lamina propria, with relatively monomorphic cells, some with prominent nucleoli, suggesting a small blue round cell tumor, likely lymphoma.
In light of the lymphoma diagnosis, a comprehensive metastasis workup was conducted. Further imaging, including a chest CT scan with oral and IV contrast, returned normal results. The patient was subsequently transferred to the hematology department, where both bone marrow biopsy and immunohistochemistry (IHC) were performed. The IHC report showed positive c-MYC expression, along with atypical lymphocytes expressing B-cell markers such as CD20 and co-expressing germinal center markers CD10 and BCL6. The Ki-67 proliferation index was exceptionally high, nearing 100%. Altogether, these findings led to a definitive diagnosis of BL. Chemotherapy was initiated with a regimen comprising cyclophosphamide, methotrexate (MTX), cytarabine, vincristine, prednisolone, and hydrocortisone. However, the initial chemotherapy regimen failed to control the disease, likely due to the aggressive nature of BL and extensive organ involvement. A bone marrow transplant was necessary to achieve remission and prevent relapse. Fortunately, the transplant was successful. The patient will undergo regular follow-up visits to monitor for signs of recurrence. Long-term management will focus on addressing any potential side effects of the transplant and maintaining remission.
Discussion
BL is an aggressive subtype of B-cell non-Hodgkin lymphoma that primarily affects children and adolescents. It is characterized by the translocation and abnormal activation of the MYC gene on chromosome 8. Despite family history, BL is usually sporadic, with no strong hereditary link [7].
BL often manifests as fast-growing tumors in areas such as the bone marrow, lymph nodes, and abdomen [8]. Abdominal involvement frequently affects the cecum and terminal ileum [9]. Our case demonstrated unusual involvement of the pancreas and gastric fundus. BL diagnosis is difficult when symptoms are atypical or localized. Rare presentations, such as acute pancreatitis or hematemesis, have been documented in a few cases [10-12]. Koca et al. [13] described diffuse pancreatic enlargement resembling autoimmune pancreatitis with associated cholestasis, whereas Dror et al. [14] reported severe pancreatitis with extreme bile duct dilatation and an additional cranial mass. In contrast, our patient’s pancreas showed multiple nodules without extreme bile duct dilatation, making the presentation even more atypical.
In pediatric cases, these conditions are generally linked to non-cancerous causes [6, 15], which can lead to misdiagnosis or diagnostic delays. However, certain symptoms should raise suspicion; for instance, jaw or dental pain should be carefully evaluated, as they may suggest an underlying malignancy. Additionally, any swelling in these areas warrants further investigation through radiological studies. Burkitt first described cases of BL in children presenting with jaw swelling and lesions, underscoring the importance of this classic symptom in early identification of the disease [8]. While mandibular involvement is well recognized, the coexistence of mandibular destruction with pancreatic and gastric lesions at initial presentation has rarely been documented, highlighting the uniqueness of our case. In addition, hematemesis is a critical sign that necessitates additional diagnostic workup [12], as our endoscopic and pathological findings raised the suspicion of lymphoma in this case. Despite these findings, radiologic evidence of malignancy was observed in the mandible. In contrast, no signs of malignancy were noted in the pancreatic imaging, highlighting the need for a comprehensive diagnostic approach. Pancreatic involvement in BL does not typically present a distinctive radiologic pattern, whether the disease is localized or widely disseminated; however, findings such as nodular or diffuse pancreatic lesions can raise suspicion of pancreatic non-Hodgkin lymphoma [13]. Taken together, compared to previously published cases, our patient’s concurrent presentation of pancreatitis, gastric fundus mass with hematemesis, and mandibular lesion represents an exceptionally uncommon constellation in an immunocompetent child.
Accurately diagnosing BL often requires a collaborative, multidisciplinary approach involving pediatricians, oncologists, radiologists, and pathologists, underscoring the necessity of a team effort for prompt and precise diagnosis. In this case, a combination of CT and MRCP imaging, endoscopy, pathology, and ultimately a bone marrow biopsy confirmed the diagnosis. Because BL grows rapidly, early diagnosis and treatment are essential. Intensive chemotherapy is the standard treatment approach, with survival rates in children significantly improving due to these protocols. Studies show that, with proper treatment, over 90% of pediatric BL patients achieve long-term survival [16]. This fact highlights the critical role of efficient clinical management and early detection in enhancing patient outcomes and preventing disease progression.
Conclusion
Clinicians should maintain a high index of suspicion for rare malignancies, such as BL, in pediatric patients with atypical symptoms. Early diagnosis, coupled with a multidisciplinary approach, is crucial for improving outcomes and ensuring timely, effective treatment.
Ethical Considerations
Compliance with ethical guidelines
In preparing this case report, all ethical guidelines were strictly followed. Informed consent was obtained from the patient’s guardians, ensuring that they fully understood and agreed to the publication of the patient’s case details. Personal identifiers were omitted to maintain patient privacy, anonymity, and confidentiality. This study was approved by the Ethics Committee of Babol University of Medical Sciences, Babol, Iran (Code: IR.MUBABOL.REC.1403.107). Written informed consent was obtained from the patient, permitting the publication of this case report and its associated images.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Data collection and writing: Fatemeh Mollaeifard; Literature review: Sanaz Mehrabani, Mohammadreza Esmaeili Dooki, and Hasan Mahmoodi Nesheli; Endoscopy: Sanaz Mehrabani; Histopathology report: Mohammad Pournasrollah; Radiology report: Firoozeh Esmaeilzadeh.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors thank the Non-Communicable Pediatric Diseases Research Center of Babol University of Medical Sciences for their support in this project.
References
Lymphomas are a heterogeneous group of lymphoid malignancies broadly classified into Hodgkin and non-Hodgkin lymphomas (NHL), with NHL being more prevalent worldwide and ranking as the 11th most common cancer [1, 2]. Burkitt lymphoma (BL), a highly aggressive B-cell lymphoma, predominantly affects children and adolescents [3]. The World Health Organization (WHO) recognizes three subtypes: Endemic (linked to malaria and Epstein-Barr virus in equatorial regions), immunodeficiency-associated (often in HIV-positive patients), and sporadic (the most frequent form in Western countries) [4]. Sporadic BL accounts for about 30% of pediatric lymphomas, typically presenting around age 10, and usually involves lymph nodes, abdomen, bone marrow, or facial bones [5].
Pancreatic involvement is rare, especially in immunocompetent children. While pancreatitis is usually attributed to infection, trauma, or medications, its occurrence as an initial manifestation of BL emphasizes the need to consider malignancy in atypical pediatric presentations [6]. In this study, we present the case of an 11-year-old immunocompetent boy whose initial symptoms of BL was associated with acute pancreatitis and jaw pain. This rare presentation is particularly important, as it underscores the need to consider malignancy in atypical pediatric pancreatitis cases.
Case Presentation
We report a 11-year-old boy with gastrointestinal discomfort. A medical history was obtained from his biological parents, and they provided informed consent for the reporting of his symptoms. He had 10 days of abdominal pain with nausea, vomiting, lethargy, and weakness. Notably, the intensity of the abdominal pain was not affected by food intake or defecation. The patient had no fever, respiratory symptoms, or recent dietary changes. The mother reported occasional constipation, but no other gastrointestinal concerns were noted. The patient had been briefly hospitalized for similar symptoms 2 days before this admission. Additionally, he reported dental pain. His past medical, surgical, and drug histories were unremarkable, and his developmental history was normal. However, his paternal uncle had been diagnosed with BL and had undergone a bone marrow transplant. On examination, his vital signs were within normal limits (Table 1); however, he exhibited signs of irritability and aggressive behavior.
Abdominal examination revealed mild periumbilical tenderness, while findings from other systems were unremarkable.
Given the patient’s presenting symptoms of nausea, vomiting, and abdominal pain, viral gastroenteritis was initially considered, based on which we initiated supportive treatment. Additionally, due to other possible diagnoses, we conducted further tests and evaluations. Diagnostic evaluations included laboratory and radiologic tests. Laboratory studies showed elevated amylase and lipase levels, suggesting acute pancreatitis. Radiological assessments, including a chest and abdominal x-rays, revealed mild fecal loading. Subsequently, an abdominal-pelvic ultrasound was performed, showing circumferential thickening and increased fat echogenicity around the descending colon, suggestive of infectious colitis. For a more detailed evaluation, a contrast-enhanced CT scan was conducted, revealing mild stranding and several lymph nodes in the transverse colon. The pancreas appeared enlarged with smooth borders. It contained at least 5 nodules with relatively well-defined margins and lower enhancement than the surrounding pancreatic tissue. These findings are most consistent with pancreatitis, particularly autoimmune pancreatitis or granulomatous disease such as sarcoidosis. Due to suspicion of autoimmune disease, ACE and IgG4 levels were checked and found within normal limits. Additionally, an ophthalmologic examination was performed to evaluate for possible uveitis.
However, the results were normal. After 7 days, he was discharged on antibiotics, pantoprazole, and probiotics. Recommendations included outpatient follow-up, with additional lab tests and a repeat abdominal-pelvic ultrasound to assess for a pancreatic pseudocyst. Outpatient referrals were made for a dental consultation to address persistent dental pain and a psychiatric consultation to evaluate and manage his irritability.
He was readmitted after 4 days due to recurrent symptoms. He presented with recurrent colicky abdominal pain centered in the epigastric and peri-umbilical regions. There was no fever or diarrhea; however, the patient reported reduced appetite, excessive sweating, and pain in the right jaw, along with noted dental decay. On initial examination, the patient’s vital signs were stable with a blood pressure of 110/60 mm Hg, a temperature of 36.7 °C, a pulse rate of 84 beats per minute, and a weight of 40 kg. There were no signs of fever or respiratory distress. Mild periumbilical tenderness was noted on abdominal examination, and the patient exhibited irritability and anxious behavior. No other significant findings were noted in the other systemic examinations. On physical examination, mild periumbilical tenderness and swelling of the right jaw were observed. Laboratory and imaging studies were conducted. Lab results showed elevated amylase and lipase levels (Table 1). Additionally, all other tests, including those for infectious causes (wright, coombs wright, widal, and PPD) were within normal limits. Based on these results, our initial diagnosis was acute pancreatitis. Sonography supported this diagnosis, revealing signs of acute pancreatitis without pseudocysts. An MRCP further confirmed pancreatitis, and an abdominal CT scan with IV contrast demonstrated pancreatic enlargement and decreased enhancement in the tail and body, along with mass-like thickening of the gastric fundus. Following our initial diagnosis of acute pancreatitis, supportive treatment was promptly initiated. Antibiotics were administered to address a suspected dental infection, and risperidone and sertraline were started to manage anxiety-related behaviors.
While our initial suspicion was focused on acute pancreatitis, additional findings warranted further investigation. Due to the jaw swelling, a sonographic evaluation was performed, revealing a hypoechoic structure adjacent to the bone between the ramus and angle. A subsequent head and neck CT scan, with and without contrast, suggested a potentially malignant soft tissue lesion near the mandible, showing destructive changes and erosion in the mandible, as well as similar changes in the zygoma and associated soft tissue lesions in both maxillary sinuses. These findings were indicative of maxillofacial lymphoma. During hospitalization, the patient also experienced episodes of coffee-ground vomiting, which prompted an endoscopy. As shown in Figure 1, this procedure identified a polypoid mass with ulceration in the gastric fundus.
In light of the lymphoma diagnosis, a comprehensive metastasis workup was conducted. Further imaging, including a chest CT scan with oral and IV contrast, returned normal results. The patient was subsequently transferred to the hematology department, where both bone marrow biopsy and immunohistochemistry (IHC) were performed. The IHC report showed positive c-MYC expression, along with atypical lymphocytes expressing B-cell markers such as CD20 and co-expressing germinal center markers CD10 and BCL6. The Ki-67 proliferation index was exceptionally high, nearing 100%. Altogether, these findings led to a definitive diagnosis of BL. Chemotherapy was initiated with a regimen comprising cyclophosphamide, methotrexate (MTX), cytarabine, vincristine, prednisolone, and hydrocortisone. However, the initial chemotherapy regimen failed to control the disease, likely due to the aggressive nature of BL and extensive organ involvement. A bone marrow transplant was necessary to achieve remission and prevent relapse. Fortunately, the transplant was successful. The patient will undergo regular follow-up visits to monitor for signs of recurrence. Long-term management will focus on addressing any potential side effects of the transplant and maintaining remission.
Discussion
BL is an aggressive subtype of B-cell non-Hodgkin lymphoma that primarily affects children and adolescents. It is characterized by the translocation and abnormal activation of the MYC gene on chromosome 8. Despite family history, BL is usually sporadic, with no strong hereditary link [7].
BL often manifests as fast-growing tumors in areas such as the bone marrow, lymph nodes, and abdomen [8]. Abdominal involvement frequently affects the cecum and terminal ileum [9]. Our case demonstrated unusual involvement of the pancreas and gastric fundus. BL diagnosis is difficult when symptoms are atypical or localized. Rare presentations, such as acute pancreatitis or hematemesis, have been documented in a few cases [10-12]. Koca et al. [13] described diffuse pancreatic enlargement resembling autoimmune pancreatitis with associated cholestasis, whereas Dror et al. [14] reported severe pancreatitis with extreme bile duct dilatation and an additional cranial mass. In contrast, our patient’s pancreas showed multiple nodules without extreme bile duct dilatation, making the presentation even more atypical.
In pediatric cases, these conditions are generally linked to non-cancerous causes [6, 15], which can lead to misdiagnosis or diagnostic delays. However, certain symptoms should raise suspicion; for instance, jaw or dental pain should be carefully evaluated, as they may suggest an underlying malignancy. Additionally, any swelling in these areas warrants further investigation through radiological studies. Burkitt first described cases of BL in children presenting with jaw swelling and lesions, underscoring the importance of this classic symptom in early identification of the disease [8]. While mandibular involvement is well recognized, the coexistence of mandibular destruction with pancreatic and gastric lesions at initial presentation has rarely been documented, highlighting the uniqueness of our case. In addition, hematemesis is a critical sign that necessitates additional diagnostic workup [12], as our endoscopic and pathological findings raised the suspicion of lymphoma in this case. Despite these findings, radiologic evidence of malignancy was observed in the mandible. In contrast, no signs of malignancy were noted in the pancreatic imaging, highlighting the need for a comprehensive diagnostic approach. Pancreatic involvement in BL does not typically present a distinctive radiologic pattern, whether the disease is localized or widely disseminated; however, findings such as nodular or diffuse pancreatic lesions can raise suspicion of pancreatic non-Hodgkin lymphoma [13]. Taken together, compared to previously published cases, our patient’s concurrent presentation of pancreatitis, gastric fundus mass with hematemesis, and mandibular lesion represents an exceptionally uncommon constellation in an immunocompetent child.
Accurately diagnosing BL often requires a collaborative, multidisciplinary approach involving pediatricians, oncologists, radiologists, and pathologists, underscoring the necessity of a team effort for prompt and precise diagnosis. In this case, a combination of CT and MRCP imaging, endoscopy, pathology, and ultimately a bone marrow biopsy confirmed the diagnosis. Because BL grows rapidly, early diagnosis and treatment are essential. Intensive chemotherapy is the standard treatment approach, with survival rates in children significantly improving due to these protocols. Studies show that, with proper treatment, over 90% of pediatric BL patients achieve long-term survival [16]. This fact highlights the critical role of efficient clinical management and early detection in enhancing patient outcomes and preventing disease progression.
Conclusion
Clinicians should maintain a high index of suspicion for rare malignancies, such as BL, in pediatric patients with atypical symptoms. Early diagnosis, coupled with a multidisciplinary approach, is crucial for improving outcomes and ensuring timely, effective treatment.
Ethical Considerations
Compliance with ethical guidelines
In preparing this case report, all ethical guidelines were strictly followed. Informed consent was obtained from the patient’s guardians, ensuring that they fully understood and agreed to the publication of the patient’s case details. Personal identifiers were omitted to maintain patient privacy, anonymity, and confidentiality. This study was approved by the Ethics Committee of Babol University of Medical Sciences, Babol, Iran (Code: IR.MUBABOL.REC.1403.107). Written informed consent was obtained from the patient, permitting the publication of this case report and its associated images.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Data collection and writing: Fatemeh Mollaeifard; Literature review: Sanaz Mehrabani, Mohammadreza Esmaeili Dooki, and Hasan Mahmoodi Nesheli; Endoscopy: Sanaz Mehrabani; Histopathology report: Mohammad Pournasrollah; Radiology report: Firoozeh Esmaeilzadeh.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors thank the Non-Communicable Pediatric Diseases Research Center of Babol University of Medical Sciences for their support in this project.
References
- Cazzola M. Introduction to a review series: The 2016 revision of the WHO classification of tumors of hematopoietic and lymphoid tissues. Blood. 2016; 127(20):2361-4. [DOI:10.1182/blood-2016-03-657379] [PMID]
- Cai W, Zeng Q, Zhang X, Ruan W. Trends analysis of non-hodgkin lymphoma at the national, regional, and global level, 1990-2019: Results from the global burden of disease Study 2019. Front Med (Lausanne). 2021; 8:738693. [DOI:10.3389/fmed.2021.738693] [PMID]
- Miles RR, Arnold S, Cairo MS. Risk factors and treatment of childhood and adolescent Burkitt lymphoma/leukaemia. Br J Haematol. 2012; 156(6):730-43. [DOI:10.1111/j.1365-2141.2011.09024.x] [PMID]
- Alaggio R, Amador C, Anagnostopoulos I, Attygalle AD, Araujo IB de O, Berti E, et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia. 2022; 36(7):1720-48. [Link]
- Kalisz K, Alessandrino F, Beck R, Smith D, Kikano E, Ramaiya NH, et al. An update on Burkitt lymphoma: A review of pathogenesis and multimodality imaging assessment of disease presentation, treatment response, and recurrence. Insights Imaging. 2019; 10(1):56. [DOI:10.1186/s13244-019-0733-7] [PMID]
- Suzuki M, Sai JK, Shimizu T. Acute pancreatitis in children and adolescents. World J Gastrointest Pathophysiol. 2014; 5(4):416-26. [DOI:10.4291/wjgp.v5.i4.416] [PMID]
- Love C, Sun Z, Jima D, Li G, Zhang J, Miles R, et al. The genetic landscape of mutations in Burkitt lymphoma. Nat Genet. 2012; 44(12):1321-5. [DOI:10.1038/ng.2468] [PMID]
- Ferry JA. BBurkitt’s lymphoma: Clinicopathologic features and differential diagnosis. Oncologist. 2006; 11(4):375-83.[DOI:10.1634/theoncologist.11-4-375] [PMID]
- Angotti R, Marini M, Giannotti G, Burgio A, Meucci D, Pavone M, et al. Gastric BBurkitt’s lymphoma in a child: A rare case. Oncol Lett. 2012; 4(4):802-4. [DOI:10.3892/ol.2012.789] [PMID]
- Amodio J, Brodsky JE. Pediatric burkitt lymphoma presenting as acute pancreatitis: MRI characteristics. Pediatr Radiol. 2010; 40(5):770-2. [DOI:10.1007/s00247-009-1475-3] [PMID]
- Mehrabani S, Nesheli HM. B-cell lymphoma presenting as acute pancreatitis symptoms in a child. Iran J Pediatr Hematol Oncol. 2021; 11(1):64-8. [DOI:10.18502/ijpho.v11i1.5008]
- Kim MS, Sung H, Han SB, Lee JW, Chung NG, Cho B, et al. Gastric Burkitt Lymphoma in a Six Year-old Boy Presenting with Upper Gastrointestinal Bleeding. Clin Pediatr Hematol Oncol. 2013; 20(2):116-20. [Link]
- Koca T, Aslan N, Dereci S, Akcam M. Burkitt lymphoma with unusual presentation: Acute pancreatitis. Pediatr Int. 2015; 57(4):775-7. [DOI:10.1111/ped.12640] [PMID]
- Dror T, Donovan V, Strubel N, Bhaumik S. Sporadic Burkitt Lymphoma Presenting with Middle Cranial Fossa Masses with Sphenoid Bony Invasion and Acute Pancreatitis in a Child. Case Rep Oncol Med. 2021; 2021:6610666.[DOI:10.1155/2021/6610666] [PMID]
- Boyle JT. Gastrointestinal bleeding in infants and children. Pediatr Rev. 2008; 29(2):39-52. [DOI:10.1542/pir.29.2.39] [PMID]
- Kim H, Park ES, Lee SH, Koo HH, Kim HS, Lyu CJ, et al. Clinical outcome of relapsed or refractory burkitt lymphoma and mature B-Cell lymphoblastic leukemia in children and adolescents. Cancer Res Treat. 2014; 46(4):358-65.[DOI:10.4143/crt.2013.047] [PMID]
Type of Study: Case Report and Review of Literature |
Subject:
Pediatrics
Received: 2025/03/3 | Accepted: 2025/05/23 | Published: 2026/01/1
Received: 2025/03/3 | Accepted: 2025/05/23 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
