
Mon, May 18, 2026


Volume 14, Issue 1 (1-2026)
J. Pediatr. Rev 2026, 14(1): 3-12 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nourmohammadi J, Lotfi M, Nazari Rad M, Ghaljaei F. Nursing and Family-centered Care and Quality of Life in Children With Diabetic Kidney Disease: A Systematic Review. J. Pediatr. Rev 2026; 14 (1) :3-12
URL: http://jpr.mazums.ac.ir/article-1-750-en.html
URL: http://jpr.mazums.ac.ir/article-1-750-en.html



1- Student Research Committee, School of Nursing and Midwifery, Zahedan University of Medical Sciences, Zahedan, Iran.
2- Faculty of Medicine, Clinical Research Development Unit of Akbar Hospital, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Pediatric Nursing, Community Nursing Research Center, School of Nursing and Midwifery, Zahedan University of Medical Sciences, Zahedan, Iran. ,ghaljaei.f51@gmail.com
2- Faculty of Medicine, Clinical Research Development Unit of Akbar Hospital, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Pediatric Nursing, Community Nursing Research Center, School of Nursing and Midwifery, Zahedan University of Medical Sciences, Zahedan, Iran. ,
Keywords: Children, Diabetic kidney disease, Family-centered care, Nursing interventions, Quality of life (QoL)
Full-Text [PDF 895 kb]
(877 Downloads)
| Abstract (HTML) (568 Views)
Full-Text: (53 Views)
Introduction
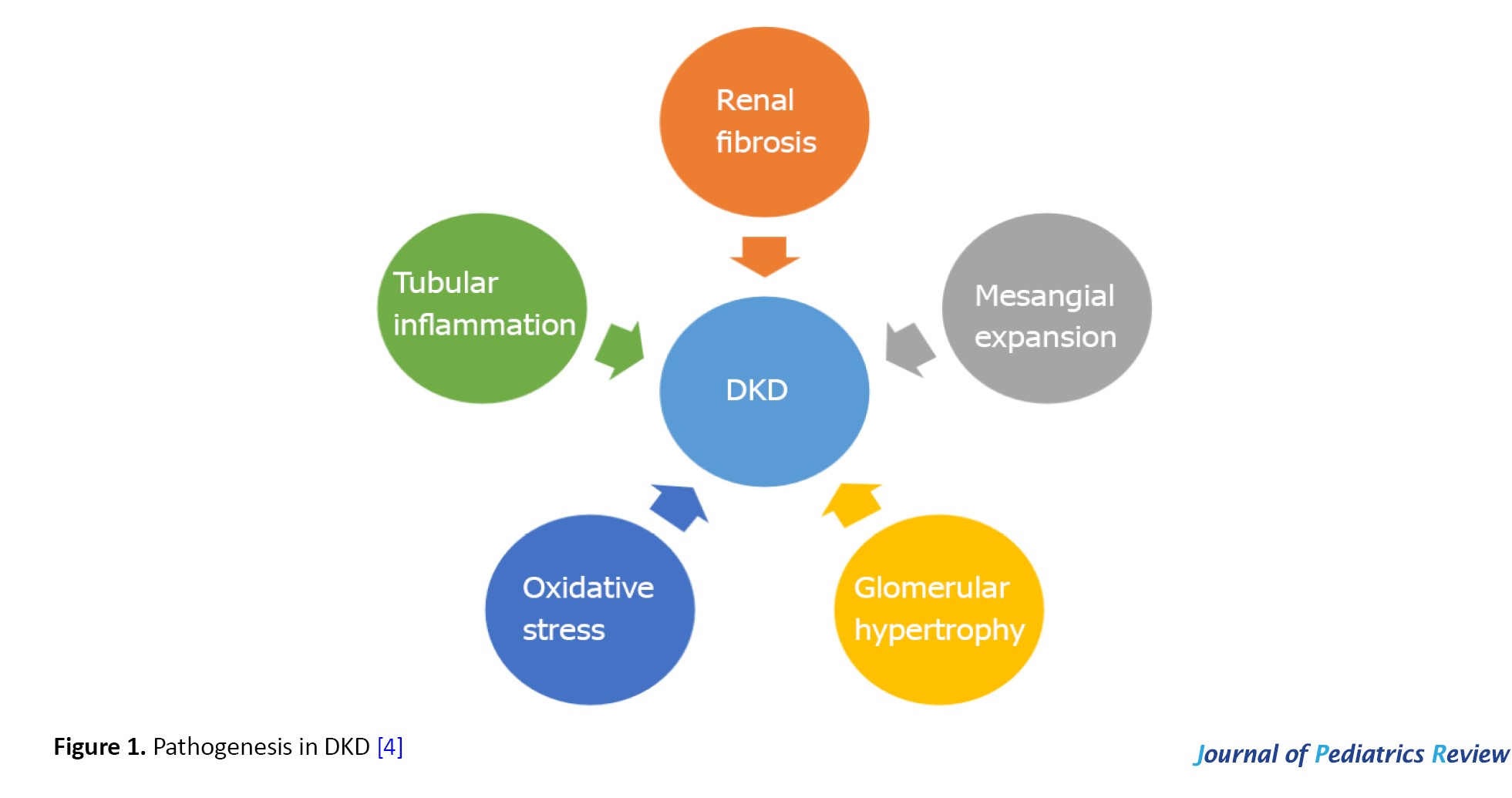
Diabetic kidney disease (DKD) in children is a severe and progressive condition that disrupts the body’s water and electrolyte balance, leading to a gradual decline in kidney function over three months or more as shown in Figure 1 [1].
 This condition typically necessitates long-term clinical care in both hospital and community settings. DKD is associated with various complications that require nursing interventions and family-centered care in inpatient and outpatient environments [2]. Given the progressive nature of the disease and the complexity of treatment protocols, nurses and families need to be actively involved in acute and preventive care strategies and in coordinating these efforts [3].
This condition typically necessitates long-term clinical care in both hospital and community settings. DKD is associated with various complications that require nursing interventions and family-centered care in inpatient and outpatient environments [2]. Given the progressive nature of the disease and the complexity of treatment protocols, nurses and families need to be actively involved in acute and preventive care strategies and in coordinating these efforts [3].
Additionally, the need for multiple treatments can be distressing for patients and their families, highlighting the critical role of nurses in educating and involving them in decision-making regarding treatment plans [4, 5]. Research indicates that approximately 26.3 million people worldwide suffer from DKD. Furthermore, data show an increasing prevalence of this disease among children, with current estimates indicating that 18 out of every 1000000 children worldwide are affected [6]. This condition significantly affects the quality of life (QoL) of affected children and their families. Children with diabetes who experience episodes of diabetic ketoacidosis (DKA) or hyperglycemia without ketoacidosis are at risk for acute kidney injury (AKI), which is characterized by volume depletion as reflected in adjusted sodium concentrations [7].
AKI during DKA is worsened by stress and inflammatory responses. Repeated instances of poor blood sugar control and DKA heighten the risk of developing DKD in children [8]. The progression involves significant alterations in the structure of various parts of the kidney, starting with the thickening of the capillary basement membrane and changes in the tubules. Additional glomerular changes may include loss of endothelial cells and matrix proliferation [9]. The longer a child has diabetes, the higher the likelihood of developing DKD. A concerning aspect of pediatric DKA is the high rate of AKI, which is linked to poorer outcomes and may result in permanent kidney damage [10]. Impact of factors involved in the onset and progression of DKD [11].
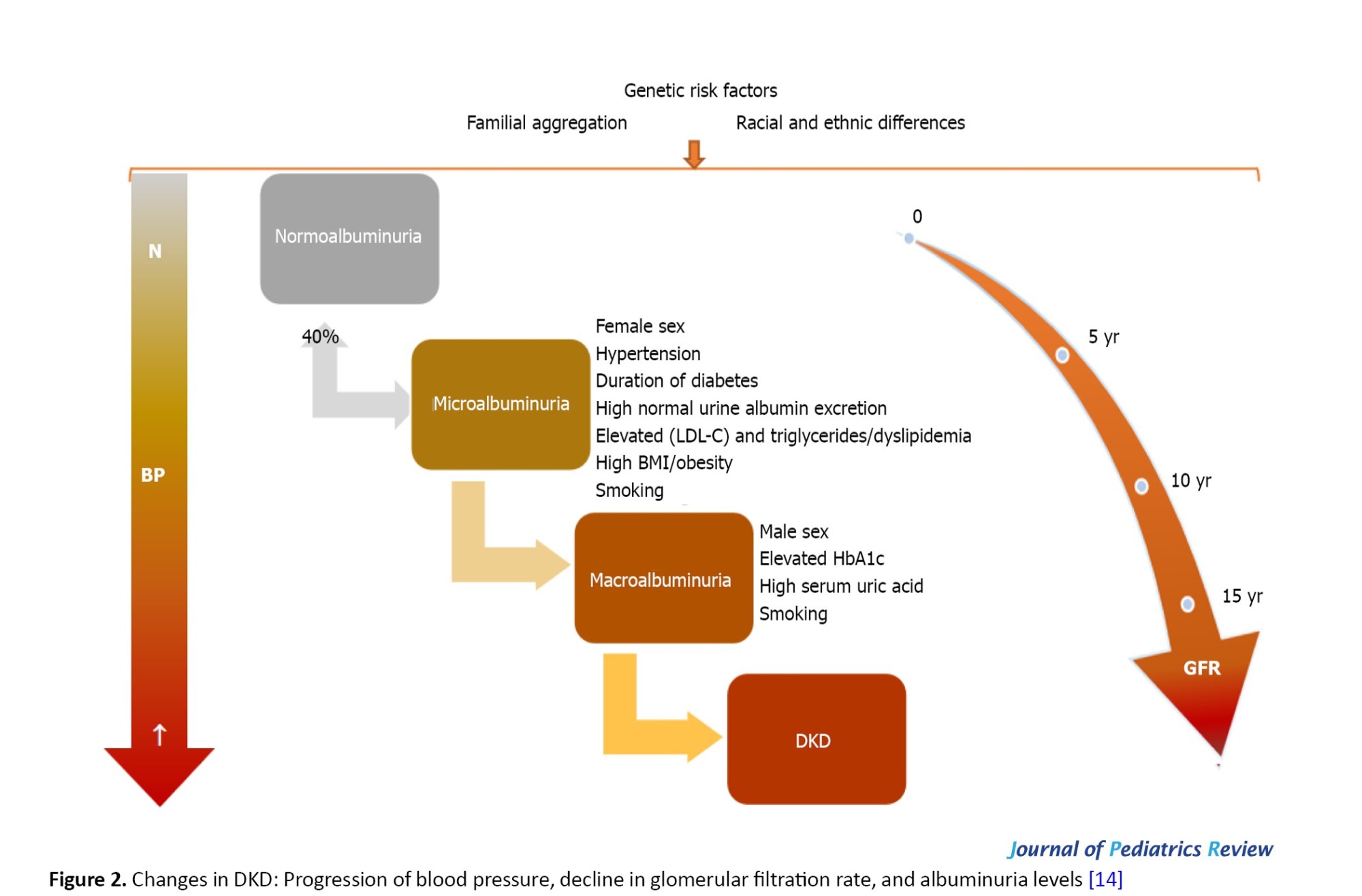
Children may exhibit symptoms such as swelling around the eyes or ankles due to fluid retention, fatigue from anemia or toxin buildup, increased frequency or urgency of nighttime urination, and elevated blood pressure. These symptoms are crucial indicators of deteriorating kidney function and require immediate medical attention [11]. Diagnosis typically involves a combination of urine tests to detect protein and blood tests to evaluate kidney function, using indicators such as serum creatinine levels and estimated glomerular filtration rate [12]. Regular monitoring is vital for early detection and prompt intervention. Managing diabetic kidney failure in children necessitates a comprehensive approach that combines specialized nursing care with family-centered support, addressing the physical, psychological, and social aspects of the disease [13]. Nurses and families play a critical role in recognizing signs and symptoms, managing treatments, and ensuring patient safety. Overall, effective nursing interventions and family-centered care can significantly improve various aspects of the QoL for children with diabetic kidney failure, particularly in psychological and physical areas as shown in Figure 2 [14].
Materials and Methods
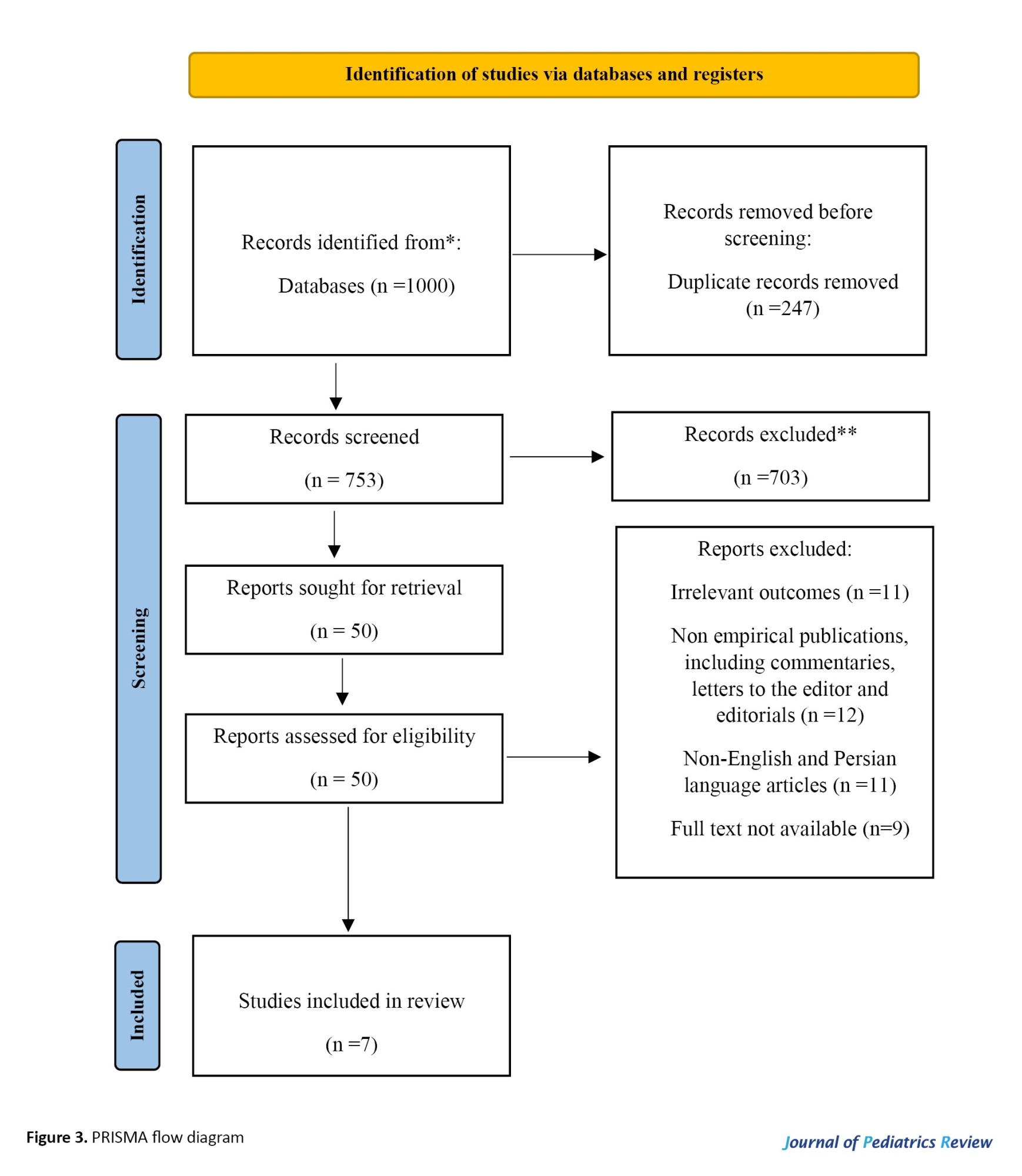
An extensive search of several academic databases initially retrieved 1000 records. After duplicates were removed and titles and abstracts were thoroughly screened, 50 articles were retained for full-text assessment. Of these, 7 studies met the predefined inclusion criteria and were published between January 2010 and March 2025.
Data sources
The literature search was conducted systematically across 5 major databases: PubMed, Scopus, Web of Science, Google Scholar, and Scientific Information Database (SID). These sources were chosen for their comprehensive coverage and reliability in the fields of medicine, health sciences, and social sciences.
Search strategy
The search employed a combination of predefined terms: (“Child”[MeSH] OR “adolescent”[MeSH] OR “pediatrics”[MeSH]) AND (“diabetic nephropathies”[MeSH] OR “kidney diseases”[MeSH] OR “renal insufficiency”[MeSH]) AND (“nursing care”[MeSH] OR “family-centered care”[MeSH] OR “patient care team”[MeSH] OR “health education”[MeSH] OR “self care”[MeSH]) AND (“quality of life”[MeSH] OR “health-related quality of life”[MeSH] OR “patient satisfaction”[MeSH]).
Eligibility criteria
Studies were eligible if they examined the effects of nursing and family-centered care interventions on the QoL of children with DKD. Broader studies addressing related outcomes were also included if they offered insights relevant to the pediatric population.
Study design
Both qualitative and quantitative research designs were considered. Acceptable study types included randomized and non-randomized trials, observational studies, systematic reviews, and case reports.
Time frame and language
Only studies published in English or Persian between January 2010 and March 2025 were included.
Exclusion criteria
Publications without original data or lacking a clearly defined methodological framework, such as commentaries, editorials, or letters, were excluded unless they provided empirically verifiable evidence. Studies in languages other than English or Persian, or those with insufficient reporting of outcomes, were also omitted.
Data extraction and management
Two reviewers independently extracted study data using a structured form. Information collected included authorship, publication year, study design, sample size, study setting, and detailed descriptions of nursing and family-centered care interventions, including frequency and duration. Data were initially recorded in Google Sheets and later imported into EndNote for duplicate removal and reference management.
Quality appraisal
To account for the variety of study designs, validated tools suitable for each methodology were applied. Randomized controlled trials were assessed using the Cochrane risk-of-bias 2 tool; observational studies were assessed using the Newcastle–Ottawa scale; and qualitative studies were assessed using the critical appraisal skills programme (CASP) checklist. Discrepancies between reviewers were resolved through discussion. No study was excluded solely on the basis of risk of bias; however, quality assessments informed the narrative synthesis, and findings from studies rated as moderate or high risk were interpreted with caution. Further details are presented in Table 1.

Data analysis
A thematic synthesis approach was used to integrate findings across studies. Following Braun and Clarke’s 6-step framework (familiarization, coding, theme identification, review, definition, and reporting), two reviewers independently conducted inductive coding. Any disagreements were resolved through discussion or consultation with a third reviewer, allowing recurring patterns to be organized into coherent thematic categories.
Limitations
Several limitations were identified: 1) high heterogeneity in study designs, sample sizes, and outcome measures prevented meta-analytic synthesis; 2) methodological quality varied, with some studies showing moderate to high risk of bias; 3) geographical and resource limitations affected the generalizability of certain interventions; and 4) few studies addressed parental psychosocial challenges, highlighting the need for further targeted research in this area.
Results
Seven studies met the inclusion criteria and were included in this review following a thorough and systematic screening process. The initial search retrieved a large number of records evaluating the effects of nursing and family-centered care interventions on the QoL of children with DKD. The selection process is illustrated in Figure 1, which presents a PRISMA-compliant flowchart in Figure 3, showing the number of records identified, screened, assessed for eligibility, and ultimately included, along with the reasons for exclusion at each stage.
 This table summarizes the key features of the seven included studies and presents the thematic categories identified during the synthesis.
This table summarizes the key features of the seven included studies and presents the thematic categories identified during the synthesis.
Family-centered care interventions for improving the QoL of children with DKD
Parental involvement is crucial in managing a child with DKD. The concept of family-centered care, which emphasizes the family’s integral role in managing children’s chronic illnesses, is gaining traction. This model treats the family as an essential collaborator in the child’s treatment plan. Fundamental to this approach are principles such as mutual respect, open communication, collaborative decision-making, and the empowerment of parents [21].
The significance of family-centered care becomes particularly apparent in conditions like DKD, where the management is intricate, prolonged, and expensive, especially when it progresses to kidney failure in children. In such contexts, family-centered care enhances the following aspects (Figure 4) [22, 23].
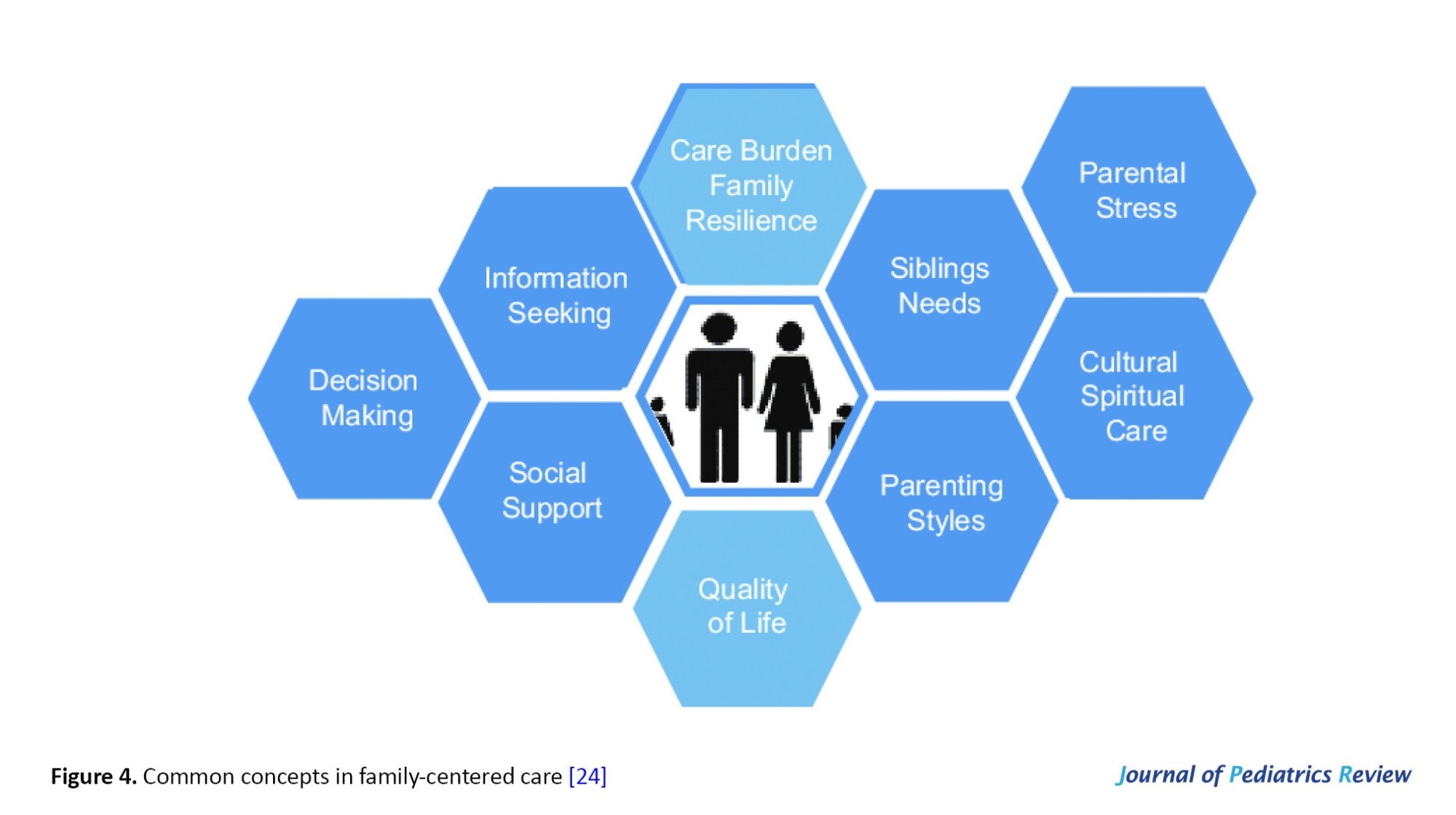 1) It boosts the family’s knowledge and ability to manage the illness; 2) It strengthens the engagement between parents and healthcare providers; 3) It amplifies family involvement in making treatment decisions. It elevates the overall wellbeing of both the child and the family.
1) It boosts the family’s knowledge and ability to manage the illness; 2) It strengthens the engagement between parents and healthcare providers; 3) It amplifies family involvement in making treatment decisions. It elevates the overall wellbeing of both the child and the family.
Discussion
AKI frequently occurs in children with DKA, although it is usually transient. The severity of this condition is associated with prolonged intensive care unit stays and extended periods required to correct the acidosis [24]. Certain factors, such as male sex and reduced serum bicarbonate levels, have been associated with an elevated risk of AKI [25]. Among children with type 1 diabetes, DKA accounts for approximately 64% of AKI cases, and it is linked to adverse outcomes, including increased hospitalization rates, higher mortality, and progression to chronic kidney disease [26].
Bergmann et al. (2024) reported a notably high frequency of AKI in children and adolescents hospitalized for DKA [27]. Although Garcia et al. did not conduct longitudinal follow-up, their findings indicated that 42% of AKI episodes persisted at follow-up [28]. In contrast, Hegab et al. observed that while most AKI cases were mild, they generally did not result in prolonged hospital stays or sustained renal dysfunction. Nonetheless, two patients progressed to end-stage renal disease after 14 years, at ages 22 and 23 [29].
Diabetes mellitus exerts a profound effect on renal and urinary function, with diabetic nephropathy recognized as the leading cause of end-stage kidney disease in children. Patients experiencing stage 2 or 3 AKI exhibited slower resolution of metabolic acidosis due to impaired renal filtration; however, roughly 80% recovered from acidosis within the first day of treatment. Clinical indicators of fluid loss were strongly correlated with AKI severity [30]. Nursing professionals need to recognize that AKI is a common complication of DKA in pediatric populations and carries a risk of permanent kidney damage. Evidence suggests that both nursing interventions and family-centered care strategies can play a crucial role in improving the QoL for children living with DKD [31].
The findings from the reviewed studies indicate that nursing and family-centered care approaches effectively address the multifaceted challenges faced by children with DKD, enhancing their physical, psychological, and social wellbeing [32]. Nursing interventions focus on maintaining fluid and electrolyte balance, supporting adequate nutrition and growth, preventing complications, and offering both educational and emotional guidance to children and their families [33]. Key nursing interventions for managing DKD involve dietary planning, insulin administration, and lifestyle modification. Pharmacological approaches, including angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, are commonly employed to protect kidney function by controlling blood pressure and minimizing proteinuria. For patients who progress to end-stage renal disease, renal replacement therapies such as dialysis or kidney transplantation may be required [34].
Proactive nursing care, when integrated with a family-centered approach, is essential for the management of pediatric DKD. Guidelines promoting healthy lifestyle behaviors, including balanced nutrition and regular exercise, play a key role in minimizing disease-related complications [35]. Although the condition presents substantial challenges for affected children and their families, early detection, coupled with comprehensive nursing interventions, has been shown to improve clinical outcomes significantly [36]. By fostering a collaborative environment among multidisciplinary healthcare providers and encouraging active family engagement, these strategies help mitigate disease risks and enhance the overall QoL for children living with diabetes [37].
Conclusion
Research shows that family-centered nursing and caregiving interventions significantly enhance the QoL for children with DKD. These approaches not only support improvements in physical health but also promote emotional wellbeing and overall QoL for children living with chronic conditions. In addition, these approaches profoundly affect children's emotional, educational, social, and lifestyle aspects. A supportive family environment plays a critical role in building resilience among these children, facilitating effective management of their condition, and improving their overall QoL. Conversely, dysfunctional family dynamics can create barriers that exacerbate the challenges these children face.
Study limitations
This review was limited to studies published in English and Persian, potentially excluding relevant and high-quality research.
Ethical Considerations
Compliance with ethical guidelines
The review was conducted following PRISMA guidelines, and its protocol was registered with PROSPERO (Code: CRD420251022114) and the Research Registry (UIN: reviewregistry1971). The authors adhered to ethical standards, including avoiding plagiarism, data fabrication, and duplicate publication.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, investigation, and writing: All authors; Methodology and formal analysis: Jalal Nourmohammadi and Mojtaba Lotfi; Data curation: Jalal Nourmohammadi, Mojtaba Lotfi and Mehrnaz Nazari Rad; Project administration: Jalal Nourmohammadi; Resources and visualization: Jalal Nourmohammadi and Mehrnaz Nazari Rad; Software: Jalal Nourmohammadi and Mojtaba Lotfi; Validation: Jalal Nourmohammadi and Mojtaba Lotfi; Supervision: Jalal Nourmohammadi and Fereshteh Ghaljaei.
Conflicts of interest
The authors declared no conflict of interest.
References
Diabetic kidney disease (DKD) in children is a severe and progressive condition that disrupts the body’s water and electrolyte balance, leading to a gradual decline in kidney function over three months or more as shown in Figure 1 [1].
Additionally, the need for multiple treatments can be distressing for patients and their families, highlighting the critical role of nurses in educating and involving them in decision-making regarding treatment plans [4, 5]. Research indicates that approximately 26.3 million people worldwide suffer from DKD. Furthermore, data show an increasing prevalence of this disease among children, with current estimates indicating that 18 out of every 1000000 children worldwide are affected [6]. This condition significantly affects the quality of life (QoL) of affected children and their families. Children with diabetes who experience episodes of diabetic ketoacidosis (DKA) or hyperglycemia without ketoacidosis are at risk for acute kidney injury (AKI), which is characterized by volume depletion as reflected in adjusted sodium concentrations [7].
AKI during DKA is worsened by stress and inflammatory responses. Repeated instances of poor blood sugar control and DKA heighten the risk of developing DKD in children [8]. The progression involves significant alterations in the structure of various parts of the kidney, starting with the thickening of the capillary basement membrane and changes in the tubules. Additional glomerular changes may include loss of endothelial cells and matrix proliferation [9]. The longer a child has diabetes, the higher the likelihood of developing DKD. A concerning aspect of pediatric DKA is the high rate of AKI, which is linked to poorer outcomes and may result in permanent kidney damage [10]. Impact of factors involved in the onset and progression of DKD [11].
Children may exhibit symptoms such as swelling around the eyes or ankles due to fluid retention, fatigue from anemia or toxin buildup, increased frequency or urgency of nighttime urination, and elevated blood pressure. These symptoms are crucial indicators of deteriorating kidney function and require immediate medical attention [11]. Diagnosis typically involves a combination of urine tests to detect protein and blood tests to evaluate kidney function, using indicators such as serum creatinine levels and estimated glomerular filtration rate [12]. Regular monitoring is vital for early detection and prompt intervention. Managing diabetic kidney failure in children necessitates a comprehensive approach that combines specialized nursing care with family-centered support, addressing the physical, psychological, and social aspects of the disease [13]. Nurses and families play a critical role in recognizing signs and symptoms, managing treatments, and ensuring patient safety. Overall, effective nursing interventions and family-centered care can significantly improve various aspects of the QoL for children with diabetic kidney failure, particularly in psychological and physical areas as shown in Figure 2 [14].
Materials and Methods
An extensive search of several academic databases initially retrieved 1000 records. After duplicates were removed and titles and abstracts were thoroughly screened, 50 articles were retained for full-text assessment. Of these, 7 studies met the predefined inclusion criteria and were published between January 2010 and March 2025.
Data sources
The literature search was conducted systematically across 5 major databases: PubMed, Scopus, Web of Science, Google Scholar, and Scientific Information Database (SID). These sources were chosen for their comprehensive coverage and reliability in the fields of medicine, health sciences, and social sciences.
Search strategy
The search employed a combination of predefined terms: (“Child”[MeSH] OR “adolescent”[MeSH] OR “pediatrics”[MeSH]) AND (“diabetic nephropathies”[MeSH] OR “kidney diseases”[MeSH] OR “renal insufficiency”[MeSH]) AND (“nursing care”[MeSH] OR “family-centered care”[MeSH] OR “patient care team”[MeSH] OR “health education”[MeSH] OR “self care”[MeSH]) AND (“quality of life”[MeSH] OR “health-related quality of life”[MeSH] OR “patient satisfaction”[MeSH]).
Eligibility criteria
Studies were eligible if they examined the effects of nursing and family-centered care interventions on the QoL of children with DKD. Broader studies addressing related outcomes were also included if they offered insights relevant to the pediatric population.
Study design
Both qualitative and quantitative research designs were considered. Acceptable study types included randomized and non-randomized trials, observational studies, systematic reviews, and case reports.
Time frame and language
Only studies published in English or Persian between January 2010 and March 2025 were included.
Exclusion criteria
Publications without original data or lacking a clearly defined methodological framework, such as commentaries, editorials, or letters, were excluded unless they provided empirically verifiable evidence. Studies in languages other than English or Persian, or those with insufficient reporting of outcomes, were also omitted.
Data extraction and management
Two reviewers independently extracted study data using a structured form. Information collected included authorship, publication year, study design, sample size, study setting, and detailed descriptions of nursing and family-centered care interventions, including frequency and duration. Data were initially recorded in Google Sheets and later imported into EndNote for duplicate removal and reference management.
Quality appraisal
To account for the variety of study designs, validated tools suitable for each methodology were applied. Randomized controlled trials were assessed using the Cochrane risk-of-bias 2 tool; observational studies were assessed using the Newcastle–Ottawa scale; and qualitative studies were assessed using the critical appraisal skills programme (CASP) checklist. Discrepancies between reviewers were resolved through discussion. No study was excluded solely on the basis of risk of bias; however, quality assessments informed the narrative synthesis, and findings from studies rated as moderate or high risk were interpreted with caution. Further details are presented in Table 1.
Data analysis
A thematic synthesis approach was used to integrate findings across studies. Following Braun and Clarke’s 6-step framework (familiarization, coding, theme identification, review, definition, and reporting), two reviewers independently conducted inductive coding. Any disagreements were resolved through discussion or consultation with a third reviewer, allowing recurring patterns to be organized into coherent thematic categories.
Limitations
Several limitations were identified: 1) high heterogeneity in study designs, sample sizes, and outcome measures prevented meta-analytic synthesis; 2) methodological quality varied, with some studies showing moderate to high risk of bias; 3) geographical and resource limitations affected the generalizability of certain interventions; and 4) few studies addressed parental psychosocial challenges, highlighting the need for further targeted research in this area.
Results
Seven studies met the inclusion criteria and were included in this review following a thorough and systematic screening process. The initial search retrieved a large number of records evaluating the effects of nursing and family-centered care interventions on the QoL of children with DKD. The selection process is illustrated in Figure 1, which presents a PRISMA-compliant flowchart in Figure 3, showing the number of records identified, screened, assessed for eligibility, and ultimately included, along with the reasons for exclusion at each stage.
Family-centered care interventions for improving the QoL of children with DKD
Parental involvement is crucial in managing a child with DKD. The concept of family-centered care, which emphasizes the family’s integral role in managing children’s chronic illnesses, is gaining traction. This model treats the family as an essential collaborator in the child’s treatment plan. Fundamental to this approach are principles such as mutual respect, open communication, collaborative decision-making, and the empowerment of parents [21].
The significance of family-centered care becomes particularly apparent in conditions like DKD, where the management is intricate, prolonged, and expensive, especially when it progresses to kidney failure in children. In such contexts, family-centered care enhances the following aspects (Figure 4) [22, 23].
Discussion
AKI frequently occurs in children with DKA, although it is usually transient. The severity of this condition is associated with prolonged intensive care unit stays and extended periods required to correct the acidosis [24]. Certain factors, such as male sex and reduced serum bicarbonate levels, have been associated with an elevated risk of AKI [25]. Among children with type 1 diabetes, DKA accounts for approximately 64% of AKI cases, and it is linked to adverse outcomes, including increased hospitalization rates, higher mortality, and progression to chronic kidney disease [26].
Bergmann et al. (2024) reported a notably high frequency of AKI in children and adolescents hospitalized for DKA [27]. Although Garcia et al. did not conduct longitudinal follow-up, their findings indicated that 42% of AKI episodes persisted at follow-up [28]. In contrast, Hegab et al. observed that while most AKI cases were mild, they generally did not result in prolonged hospital stays or sustained renal dysfunction. Nonetheless, two patients progressed to end-stage renal disease after 14 years, at ages 22 and 23 [29].
Diabetes mellitus exerts a profound effect on renal and urinary function, with diabetic nephropathy recognized as the leading cause of end-stage kidney disease in children. Patients experiencing stage 2 or 3 AKI exhibited slower resolution of metabolic acidosis due to impaired renal filtration; however, roughly 80% recovered from acidosis within the first day of treatment. Clinical indicators of fluid loss were strongly correlated with AKI severity [30]. Nursing professionals need to recognize that AKI is a common complication of DKA in pediatric populations and carries a risk of permanent kidney damage. Evidence suggests that both nursing interventions and family-centered care strategies can play a crucial role in improving the QoL for children living with DKD [31].
The findings from the reviewed studies indicate that nursing and family-centered care approaches effectively address the multifaceted challenges faced by children with DKD, enhancing their physical, psychological, and social wellbeing [32]. Nursing interventions focus on maintaining fluid and electrolyte balance, supporting adequate nutrition and growth, preventing complications, and offering both educational and emotional guidance to children and their families [33]. Key nursing interventions for managing DKD involve dietary planning, insulin administration, and lifestyle modification. Pharmacological approaches, including angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, are commonly employed to protect kidney function by controlling blood pressure and minimizing proteinuria. For patients who progress to end-stage renal disease, renal replacement therapies such as dialysis or kidney transplantation may be required [34].
Proactive nursing care, when integrated with a family-centered approach, is essential for the management of pediatric DKD. Guidelines promoting healthy lifestyle behaviors, including balanced nutrition and regular exercise, play a key role in minimizing disease-related complications [35]. Although the condition presents substantial challenges for affected children and their families, early detection, coupled with comprehensive nursing interventions, has been shown to improve clinical outcomes significantly [36]. By fostering a collaborative environment among multidisciplinary healthcare providers and encouraging active family engagement, these strategies help mitigate disease risks and enhance the overall QoL for children living with diabetes [37].
Conclusion
Research shows that family-centered nursing and caregiving interventions significantly enhance the QoL for children with DKD. These approaches not only support improvements in physical health but also promote emotional wellbeing and overall QoL for children living with chronic conditions. In addition, these approaches profoundly affect children's emotional, educational, social, and lifestyle aspects. A supportive family environment plays a critical role in building resilience among these children, facilitating effective management of their condition, and improving their overall QoL. Conversely, dysfunctional family dynamics can create barriers that exacerbate the challenges these children face.
Study limitations
This review was limited to studies published in English and Persian, potentially excluding relevant and high-quality research.
Ethical Considerations
Compliance with ethical guidelines
The review was conducted following PRISMA guidelines, and its protocol was registered with PROSPERO (Code: CRD420251022114) and the Research Registry (UIN: reviewregistry1971). The authors adhered to ethical standards, including avoiding plagiarism, data fabrication, and duplicate publication.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, investigation, and writing: All authors; Methodology and formal analysis: Jalal Nourmohammadi and Mojtaba Lotfi; Data curation: Jalal Nourmohammadi, Mojtaba Lotfi and Mehrnaz Nazari Rad; Project administration: Jalal Nourmohammadi; Resources and visualization: Jalal Nourmohammadi and Mehrnaz Nazari Rad; Software: Jalal Nourmohammadi and Mojtaba Lotfi; Validation: Jalal Nourmohammadi and Mojtaba Lotfi; Supervision: Jalal Nourmohammadi and Fereshteh Ghaljaei.
Conflicts of interest
The authors declared no conflict of interest.
References
- Das S, Gnanasambandan R. Intestinal microbiome diversity of diabetic and non-diabetic kidney disease: Current status and future perspective. Life Sci. 2023; 316:121414.[DOI:10.1016/j.lfs.2023.121414] [PMID]
- Muntean C, Starcea IM, Banescu C. Diabetic kidney disease in pediatric patients: A current review. World J Diabetes. 2022; 13(8):587-99. [DOI:10.4239/wjd.v13.i8.587] [PMID]
- Piani F, Reinicke T, Borghi C, Tommerdahl KL, Cara-Fuentes G, Johnson RJ, et al. Acute Kidney Injury in Pediatric Diabetic Kidney Disease. Front Pediatr. 2021; 9:668033.[DOI:10.3389/fped.2021.668033] [PMID]
- Bjornstad P, Cherney DZ, Maahs DM. Update on Estimation of Kidney Function in Diabetic Kidney Disease. Curr Diab Rep. 2015; 15(9):57. [DOI:10.1007/s11892-015-0633-2] [PMID]
- Mamilly L, Mastrandrea LD, Mosquera Vasquez C, Klamer B, Kallash M, Aldughiem A. Evidence of early diabetic nephropathy in pediatric type 1 diabetes. Front Endocrinol (Lausanne). 2021; 12:669954. [DOI:10.3389/fendo.2021.669954] [PMID]
- Evin F, Kırkgöz T, Atik T, Ak G, Köse T, Kabasakal C, et al. “Predicting diabetic kidney disease in youth with type 1 diabetes: Insights from genetic risk assessment”. J Diabetes Complications. 2024; 38(11):108833. [DOI:10.1016/j.jdiacomp.2024.108833] [PMID]
- Ryan P, Delbert E, Del Vecchio M, Costello C, Hamilton J, Wicklow B, et al. Diabetic kidney disease screening practices amongst canadian pediatric endocrinologists. Can J Diabetes. 2024; 48(7):S18. [DOI:10.1016/j.jcjd.2024.09.057]
- Sethi SK, Bunchman T, Chakraborty R, Raina R. Pediatric acute kidney injury: New advances in the last decade. Kidney Res Clin Pract. 2021; 40(1):40-51. [DOI:10.23876/j.krcp.20.074] [PMID]
- Marzuillo P, Iafusco D, Zanfardino A, Guarino S, Piscopo A, Casaburo F, et al. Acute kidney injury and renal tubular damage in children with type 1 diabetes mellitus onset. J Clin Endocrinol Metab. 2021; 106(7):e2720-37. [DOI:10.1210/clinem/dgab090] [PMID]
- Devarajan P, Jefferies JL. Progression of chronic kidney disease after acute kidney injury. Prog Pediatr Cardiol. 2016; 41:33-40. [DOI:10.1016/j.ppedcard.2015.12.006] [PMID]
- Laskin BL, Goebel J. Acute kidney injury in children admitted with diabetic ketoacidosis: Finding the sweet spot of fluid management. JAMA Pediatr. 2017; 171(5):e170009. [DOI:10.1001/jamapediatrics.2017.0009] [PMID]
- Roy JP, Devarajan P. Acute kidney injury: Diagnosis and management. Indian J Pediatr. 2020; 87(8):600-7. [DOI:10.1007/s12098-019-03096-y] [PMID]
- Cummins TD, Korte EA, Bhayana S, Merchant ML, Barati MT, Smoyer WE, et al. Advances in proteomic profiling of pediatric kidney diseases. Pediatr Nephrol. 2022; 37(10):2255-65. [DOI:10.1007/s00467-022-05497-2] [PMID]
- Lanzaro F, Barlabà A, De Nigris A, Di Domenico F, Verde V, Miraglia del Giudice E, et al. Pediatric diabetic nephropathy: Novel insights from microRNAs. J Clin Med. 2023; 12(4):1447. [DOI:10.3390/jcm12041447] [PMID]
- Soltysiak J, Krzysko-Pieczka I, Gertig-Kolasa A, Mularz E, Skowrońska B, Ostalska-Nowicka D, et al. Acute kidney injury and diabetic kidney disease in children with acute complications of diabetes. Pediatr Nephrol. 2023; 38(5):1643-52. [DOI:10.1007/s00467-022-05735-7] [PMID]
- Lopez LN, Wang W, Loomba L, Afkarian M, Butani L. Diabetic kidney disease in children and adolescents: An update. Pediatr Nephrol. 2022; 37(11):2583-97. [DOI:10.1007/s00467-021-05347-7] [PMID]
- Hursh BE, Ronsley R, Islam N, Mammen C, Panagiotopoulos C. Acute kidney injury in children with type 1 diabetes hospitalized for diabetic ketoacidosis. JAMA Pediatr. 2017; 171(5):e170020. [DOI:10.1001/jamapediatrics.2017.0020] [PMID]
- Huang SK, Huang CY, Lin CH, Cheng BW, Chiang YT, Lee YC, et al. Acute kidney injury is a common complication in children and adolescents hospitalized for diabetic ketoacidosis. Plos One. 2020; 15(10):e0239160. [DOI:10.1371/journal.pone.0239160] [PMID]
- Bjornstad P, Nehus E, El Ghormli L, Bacha F, Libman IM, McKay S, et al. Insulin sensitivity and diabetic kidney disease in children and adolescents with type 2 diabetes: An observational analysis of data from the TODAY clinical trial. Am J Kidney Dis. 2018; 71(1):65-74. [DOI:10.1053/j.ajkd.2017.07.015] [PMID]
- Myers SR, Glaser NS, Trainor JL, Nigrovic LE, Garro A, Tzimenatos L, et al. Frequency and risk factors of acute kidney injury during diabetic ketoacidosis in children and association with neurocognitive outcomes. JAMA Netw Open. 2020; 3(12):e2025481. [DOI:10.1001/jamanetworkopen.2020.25481] [PMID]
- LeBron J, Ronis S. Factors associated with patient- and family-centered care in the Hispanic pediatric population: A secondary analysis. Acad Pediatr. 2025; 25(6):102828.[DOI:10.1016/j.acap.2025.102828] [PMID]
- Lyon ME, Fraser JL, Thompkins JD, Clark H, Brodie N, Detwiler K, Torres C, et al. Advance care planning for children with rare diseases: A pilot RCT. Pediatrics. 2024; 153(6):e2023064557. [PMID]
- Darwish MM, Hassan SH, Taha SF, Abd El-Megeed HS, Ismail TAM. Family impact and economic burden among caregivers of children with chronic kidney disease in Assiut, Egypt. J Egypt Public Health Assoc. 2020; 95(1):27. [DOI:10.1186/s42506-020-00058-7] [PMID]
- Meena J, Yadav J, Kumar J, Dawman L, Tiewosh K, Mittal A, et al. Incidence, predictors, and short-term outcomes of acute kidney injury in children with diabetic ketoacidosis: A systematic review. Pediatr Nephrol. 2023; 38(7):2023-31. [DOI:10.1007/s00467-023-05878-1] [PMID]
- Al Khalifah R, Al-Eyadhy A, Musibeeh N, Alshalawi A, Alanazi N, Alhboob A, et al. Risk factors, outcomes, and predictors of resolution of acute kidney injury in children with diabetic ketoacidosis. Pediatr Nephrol. 2023; 38(2):573-82.[DOI:10.1007/s00467-022-05578-2] [PMID]
- Baalaaji M, Jayashree M, Nallasamy K, Singhi S, Bansal A. Predictors and outcome of acute kidney injury in children with diabetic ketoacidosis. Indian Pediatr. 2018; 55(4):311-4. [DOI:10.1007/s13312-018-1274-8] [PMID]
- Bergmann KR, Bjornstad P, Abuzzahab MJ, Zhong L, Collins-Dippel E, Nickel A, et al. Multicentre, retrospective cohort study protocol to identify racial and ethnic differences in acute kidney injuries in children and adolescents with diabetic ketoacidosis. BMJ Open. 2024; 14(6):e086261. [Link]
- Sánchez García C, Briones Castellanos M, Velasco Morales A. Acute kidney injury and diabetic ketoacidosis in pediatric patients: Risk factors. Arch Argent Pediatr. 2020; 118(2):135-8. [DOI:10.5546/aap.2020.eng.135] [PMID]
- Hegab AM, Khalil FF, Abosedera MM. Incidence and factors associated with acute kidney injury among children with type 1 diabetes hospitalized with diabetic ketoacidosis: A prospective study. Pediatr Diabetes. 2022; 23(6):783-91.[DOI:10.1111/pedi.13370] [PMID]
- Yuan XW, Wang X, Tang N, Xie H, Gu W. [A clinical study of acute kidney injury in children with type 1 diabetes and diabetic ketoacidosis (Chinese)]. Zhongguo Dang Dai Er Ke Za Zhi. 2022; 24(8):858-62. [PMID]
- Mishra OP, Prasad R. Acute Kidney Injury in Children with Diabetic Ketoacidosis: Risk factors and outcome. Indian J Pediatr. 2021; 88(6):5423. [DOI:10.1007/s12098-021-03762-0] [PMID]
- Ghaljaei F, Lotfi M, Rad MN, Ghaljeh M, Nourmohammadi J. [Nursing Interventions for Pediatrics with Type 1 Diabetes and Their Families: A systematic review (Persian)]. Iran J Diabetes Metab. 2025; 25(5):395-404. [Link]
- Parajuli B, Angurana SK, Baalaaji M, Williams V. Acute kidney injury in children with diabetic ketoacidosis: A real concern. Pediatr Crit Care Med. 2019; 20(6):590-1.[DOI:10.1097/PCC.0000000000001928] [PMID]
- Cirillo L, De Chiara L, Innocenti S, Errichiello C, Romagnani P, Becherucci F. Chronic kidney disease in children: An update. Clin Kidney J. 2023; 16(10):1600-11. [DOI:10.1093/ckj/sfad097] [PMID]
- Greenberg JH, Kakajiwala A, Parikh CR, Furth S. Emerging biomarkers of chronic kidney disease in children. Pediatr Nephrol. 2018; 33(6):925-33. [DOI:10.1007/s00467-017-3701-9] [PMID]
- Rossing P, Groop PH, Singh R, Lawatscheck R, Tuttle KR. Prevalence of chronic kidney disease in type 1 diabetes among adults in the US. Diabetes Care. 2024; 47(8):1395-9. [DOI:10.2337/dc24-0335] [PMID]
- Amatruda M, Gembillo G, Giuffrida AE, Santoro D, Conti G. The aggressive diabetic kidney disease in youth-onset type 2 diabetes: Pathogenetic mechanisms and potential therapies. Medicina. 2021; 57(9):868. [DOI:10.3390/medicina57090868] [PMID]
Type of Study: Review Article |
Subject:
Pediatric Nephrology
Received: 2025/01/15 | Accepted: 2025/07/15 | Published: 2026/01/1
Received: 2025/01/15 | Accepted: 2025/07/15 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
