
Mon, Jul 13, 2026


Volume 14, Issue 2 (April 2026)
J. Pediatr. Rev 2026, 14(2): 97-110 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Alimohammadi M, Sabzyan M, Kelishadi R, Vard B, Maghami-Mehr A. The Effect of Zinc on Appetite and Nutritional Status in Children: A Systematic Review. J. Pediatr. Rev 2026; 14 (2) :97-110
URL: http://jpr.mazums.ac.ir/article-1-769-en.html
URL: http://jpr.mazums.ac.ir/article-1-769-en.html



1- Department of General Practice, Isfahan University of Medical Sciences, Isfahan, Iran. , nima.alimohammadi1999@gmail.com
2- Department of Pediatrics, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran.
3- Child Growth and Development Research Center, Research Institute for Primordial Prevention of Non-Communicable Disease, Isfahan University of Medical Sciences, Isfahan, Iran.
4- Department of Pediatrics, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran. & Child Growth and Development Research Center, Research Institute for Primordial Prevention of Non-Communicable Disease, Isfahan University of Medical Sciences, Isfahan, Iran.
5- Department of Statistics, Faculty of Mathematical Sciences, Yazd University, Yazd, Iran.
2- Department of Pediatrics, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran.
3- Child Growth and Development Research Center, Research Institute for Primordial Prevention of Non-Communicable Disease, Isfahan University of Medical Sciences, Isfahan, Iran.
4- Department of Pediatrics, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran. & Child Growth and Development Research Center, Research Institute for Primordial Prevention of Non-Communicable Disease, Isfahan University of Medical Sciences, Isfahan, Iran.
5- Department of Statistics, Faculty of Mathematical Sciences, Yazd University, Yazd, Iran.
Keywords: Zinc, Pediatrics, Micronutrients, Development, Nutrition, Supplementation, Systematic review
Full-Text [PDF 791 kb]
(231 Downloads)
| Abstract (HTML) (476 Views)
Full-Text: (45 Views)
Introduction
Zinc, an essential trace element, plays a critical role for numerous biological processes in the human body, particularly in supporting cellular growth and differentiation. This role is largely attributed to its involvement in nucleic acid and protein synthesis, as well as its influence on hormonal mediators of growth [1]. Zinc is also integral to the metabolism of proteins, lipids, and nucleic acids and contributes to gene transcription. Its wide range of functions includes roles in supporting reproduction, immune function, and wound repair. At the cellular level, zinc significantly impacts the normal functioning of macrophages, neutrophils, natural killer cells, and the complement system [2]. Furthermore, zinc serves as a structural component or catalyst in zinc metalloenzymes that regulate antioxidant defense, anti-inflammatory responses, immune function, and apoptosis [3].
Zinc deficiency is a major contributor to childhood stunting, particularly during infancy and early childhood, and is associated with several adverse health consequences, including growth retardation [4], delayed wound healing [5], increased susceptibility to infectious diseases [6], and impaired cognitive function [7]. Zinc deficiency is a significant public health issue in nearly all low- and middle-income countries, with an estimated prevalence ranging from 20% to 26% among children [8]. The main causes of zinc deficiency include inadequate consumption of zinc-rich foods, increased requirements or losses, malabsorption, and impaired zinc utilization. In healthy infants, zinc needs are typically met through breast milk during the first 6 months of life. However, beyond this period, complementary foods must provide sufficient zinc to support optimal growth and development, as breast milk alone may no longer be adequate [9]. Zinc is abundant in foods, such as meat, fish, poultry, and oysters; however, its bioavailability is reduced by dietary components, such as phytates—inositol phosphates found in cereals, grains, seeds, and legumes—which form poorly soluble complexes with zinc and inhibit its absorption. Diets high in phytates, common in many low- and middle-income countries, thus increase the risk of zinc deficiency, particularly where access to high-zinc foods is limited [10].
Globally, approximately 17.3% of the population is estimated to be at risk of inadequate zinc intake [11]. This issue is particularly concerning in pediatric populations, where zinc deficiency has been reported in 20–26% of otherwise healthy children, underscoring the need for enhanced monitoring and intervention strategies [12]. Zinc has been shown to influence appetite by enhancing ghrelin secretion, a hormone that stimulates hunger [13, 14]. Additionally, low zinc status may impair taste acuity and increase stress and anxiety in children, potentially reducing appetite and food intake, thereby exacerbating nutritional deficiencies [12, 15].
In addition to its well-known role in appetite regulation and growth, zinc is involved in the modulation of the hypothalamic–pituitary–gonadal axis. Emerging evidence suggests that excessive zinc exposure during sensitive developmental periods may be associated with earlier activation of pubertal pathways. This biological consideration has led to clinical caution regarding routine zinc supplementation before the onset of puberty, particularly in otherwise healthy children [16].
Multiple studies have been conducted to assess the effect of zinc on children’s growth; however, their findings are inconsistent, with variations attributed to differences in study populations, intervention types, and settings. Previous systematic reviews on this topic have highlighted significant variability in participant characteristics, intervention protocols, and outcome measures, making it challenging to provide clear, evidence-based conclusions about the efficacy and safety of zinc supplementation for improving linear growth and appetite in children [14]. Therefore, this systematic review aimed to synthesize the available evidence and address the specific question of how zinc intake, through diet or supplementation, impacts appetite and growth in healthy children aged 6 months to 18 years.
Materials and Methods
Protocol and registration
This systematic review followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines [17] and was registered in the International Prospective Register of Systematic Reviews (PROSPERO CRD42024578984). Ethical approval and patient consent were not required because all analyses were based on previously published studies.
Eligibility criteria
Type of studies: We included observational studies (cross‑sectional, case–control, and cohort studies), prospective and retrospective studies, and randomized controlled trials (RCTs) assessing zinc intake (dietary or supplemental, including medicinal or food fortification) and its relationship with appetite or growth in healthy children. The exclusion criteria were letters, conference proceedings, reviews, duplicated data, animal studies, and studies lacking relevant data. To minimize bias, we attempted to obtain full texts through institutional access, interlibrary loans, or author contact; however, 14 studies were excluded due to inaccessible full texts, potentially introducing selection bias.
Study population: Healthy children and adolescents aged 6 months to 18 years were eligible. Studies on infants younger than six months or children with chronic illnesses were excluded to focus on healthy populations.
Outcome parameters: Studies were included if they reported outcomes related to appetite, weight-for-age Z-score (WAZ), height-for-age Z-scores (HAZ), linear growth, weight-for-length Z-scores (WLZ), or body mass index (BMI)-for-age.
Information sources and search
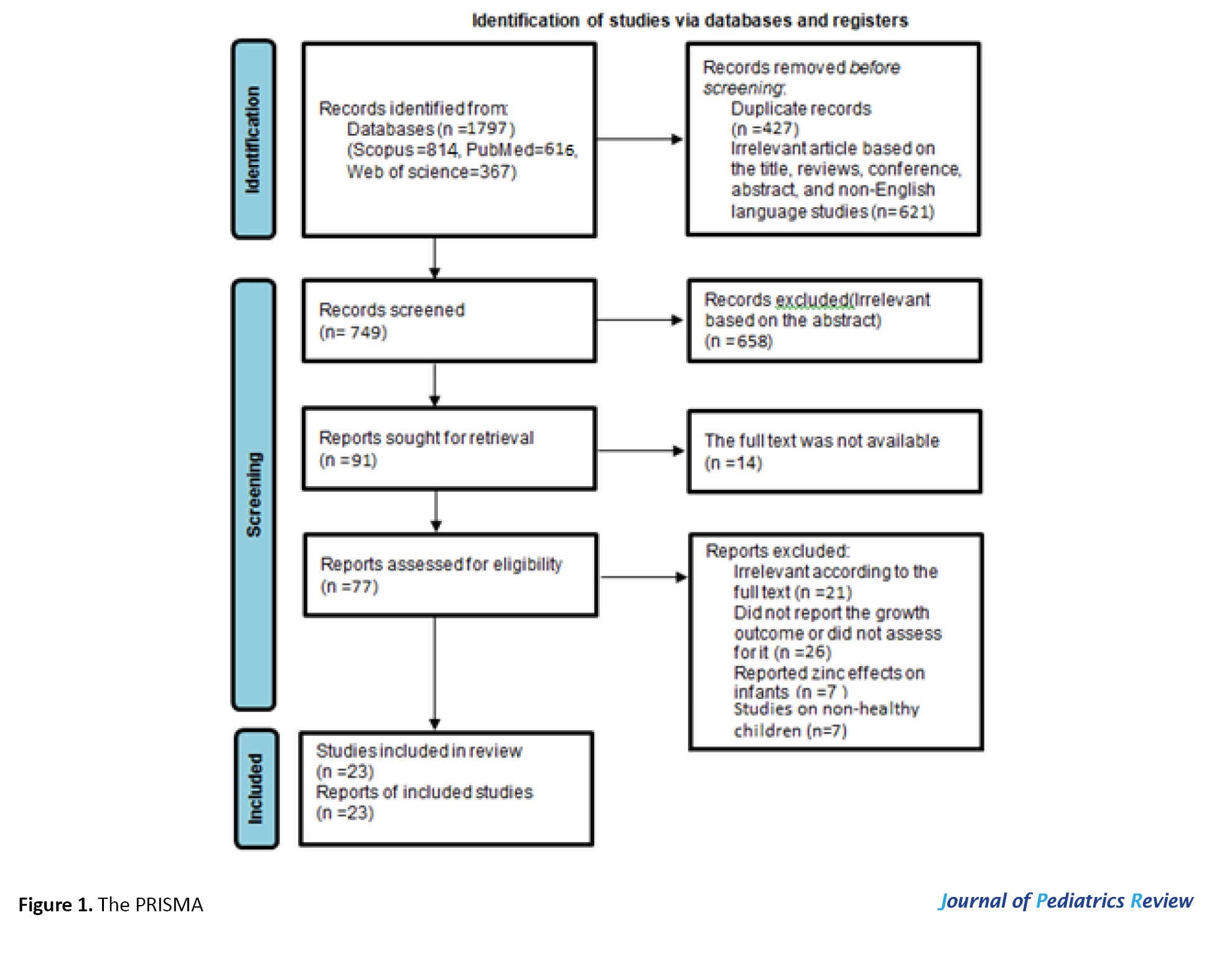
We searched PubMed, Web of Science, and Scopus for studies published from April 2015 to January 2024, using terms such as “zinc”, “dietary zinc”, “zinc intake”, “serum zinc”, “zinc supplementation”, “zinc supplements”, “poor appetite”, “appetite”, “anorexia”, “nutritional status”, “food intake”, “eating”, “food consumption”, “energy intake”, “growth”, “growth development”, “malnutrition”, “body height”, “body weight”, “body mass index”, “child”, “children”, “toddler”, “pediatrics”, “adolescent”, “infant”. Reference lists of all included papers and relevant reviews were screened for additional citations [18]. The search identified 1,797 articles, which were managed using Endnote 20.0 to remove duplicates. Titles and abstracts of the identified studies were scanned in duplicate to exclude irrelevant references. Titles, abstracts, and full texts were screened independently by two authors to ensure eligibility, with disputes resolved through consensus. Twenty‑three studies met the eligibility criteria and were included in the final review (Figure 1).
Search strategy
PubMed
Search terms: ((“zinc”[Mesh] OR “dietary zinc” OR “zinc intake” OR “serum zinc” OR “zinc supplementation” OR “zinc supplements”) AND (“poor appetite” OR “appetite”[Mesh] OR “anorexia”[Mesh] OR “nutritional status”[Mesh] OR “food intake” OR “eating”[Mesh] OR “food consumption” OR “energy intake”[Mesh] OR “growth”[Mesh] OR “growth development”[Mesh] OR “malnutrition”[Mesh] OR “body height”[Mesh] OR “body weight”[Mesh] OR “body mass index”[Mesh]) AND (“child”[Mesh] OR “children” OR “toddler” OR “pediatrics”[Mesh] OR “adolescent”[Mesh] OR “infant”[Mesh]))
Search timeframe: January 2015-January 2024, Total articles identified: 616.
Web of Science
Search terms: TS=(“Zinc” OR “dietary zinc” OR “zinc intake” OR “serum zinc” OR “zinc supplementation” OR “zinc supplements”) AND
TS=(“Poor appetite” OR “appetite” OR “anorexia” OR “nutritional status” OR “food intake” OR “eating” OR “food consumption” OR “energy intake” OR “growth” OR “growth development” OR “malnutrition” OR “body height” OR “body weight” OR “body mass index”) AND
TS=(“Child” OR “children” OR “toddler” OR “pediatrics” OR “adolescent” OR “infant”)
Search timeframe: January 2015-January 2024, Total articles identified: 367.
Scopus
Search terms: (TITLE-ABS-KEY(“zinc” OR “dietary zinc” OR “zinc intake” OR “serum zinc” OR “zinc supplementation” OR “zinc supplements”) AND
TITLE-ABS-KEY(“poor appetite” OR “appetite” OR “anorexia” OR “nutritional status” OR “food intake” OR “eating” OR “food consumption” OR “energy intake” OR “growth” OR “growth development” OR “malnutrition” OR “body height” OR “body weight” OR “body mass index”) AND
TITLE-ABS-KEY(“child” OR “children” OR “toddler” OR “pediatrics” OR “adolescent” OR “infant”))
Search timeframe: January 2015-January 2024, Total articles identified: 814.
Selection of studies
Two authors independently screened and assessed the eligibility of the studies, extracted relevant data, and assessed the risk of bias for all included studies. Disagreements were resolved through discussion until consensus was reached.
Data collection process
Data were collected independently by two authors, who reviewed and consolidated the data from the included studies.
Assessment of risk of bias
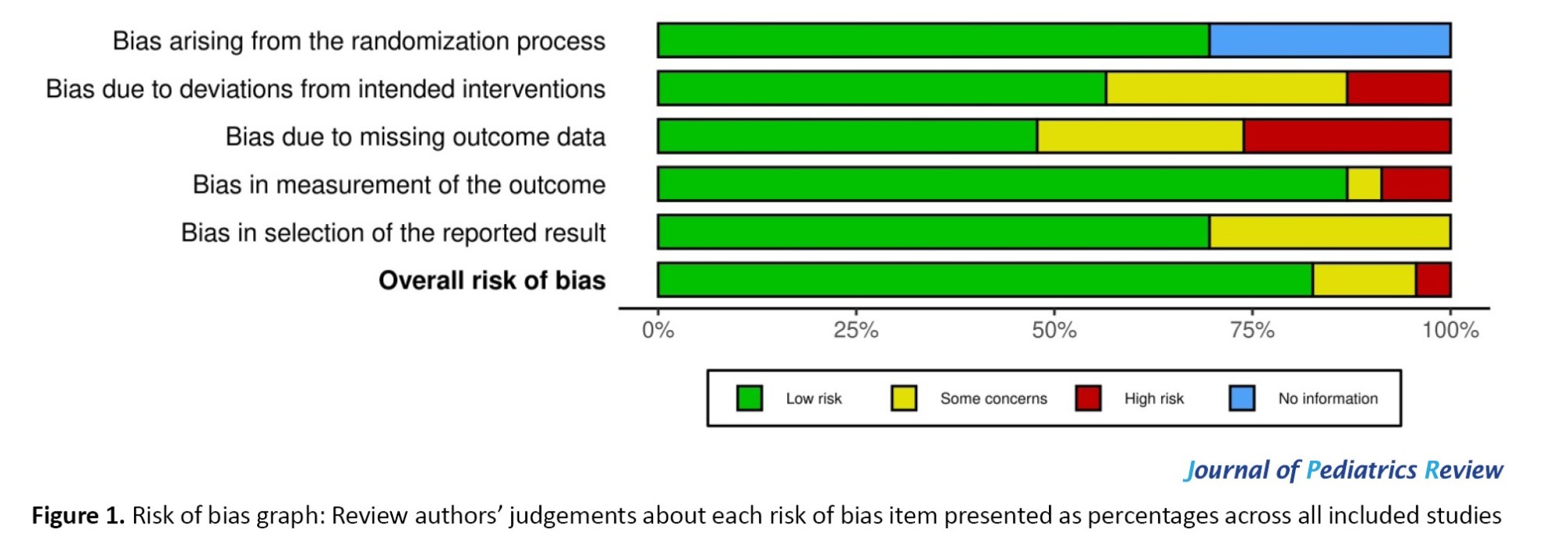
In this review, all studies underwent critical appraisal by one review team member (X) using the Joanna Briggs Institute critical appraisal checklists [19]. This tool was chosen because it can be used to assess descriptive cross-sectional studies as well as randomized controlled trials [20, 21]. A second reviewer (Y) blinded to the first reviewer’s (X) assessments checked a random 15% of the included articles for risk of bias, and any differences between the reviewers were discussed and resolved. Figure 2 shows the reviewers’ judgments about each risk of bias item for each included study.
Synthesis of results
The results were synthesized based on the extracted data, and findings were analyzed to provide insights into the effect of zinc on appetite and growth in children.
Results
Study selection
A total of 1,797 articles were identified (616 from PubMed, 814 from Scopus, and 367 from Web of Science). After removing 427 duplicates, 1,370 abstracts were screened, and 621 articles unrelated to zinc, growth, or appetite in children were excluded, along with 658 additional irrelevant records. Of the remaining 91 articles, the full texts were reviewed, and 68 were excluded: 14 due to unavailable full texts, 21 for irrelevance, 26 for not reporting growth outcomes or focusing on infants under 6 months, and 7 for including non-healthy children. Twenty-three studies [12, 22-43] were included (Figure 1).
Characteristics of included studies
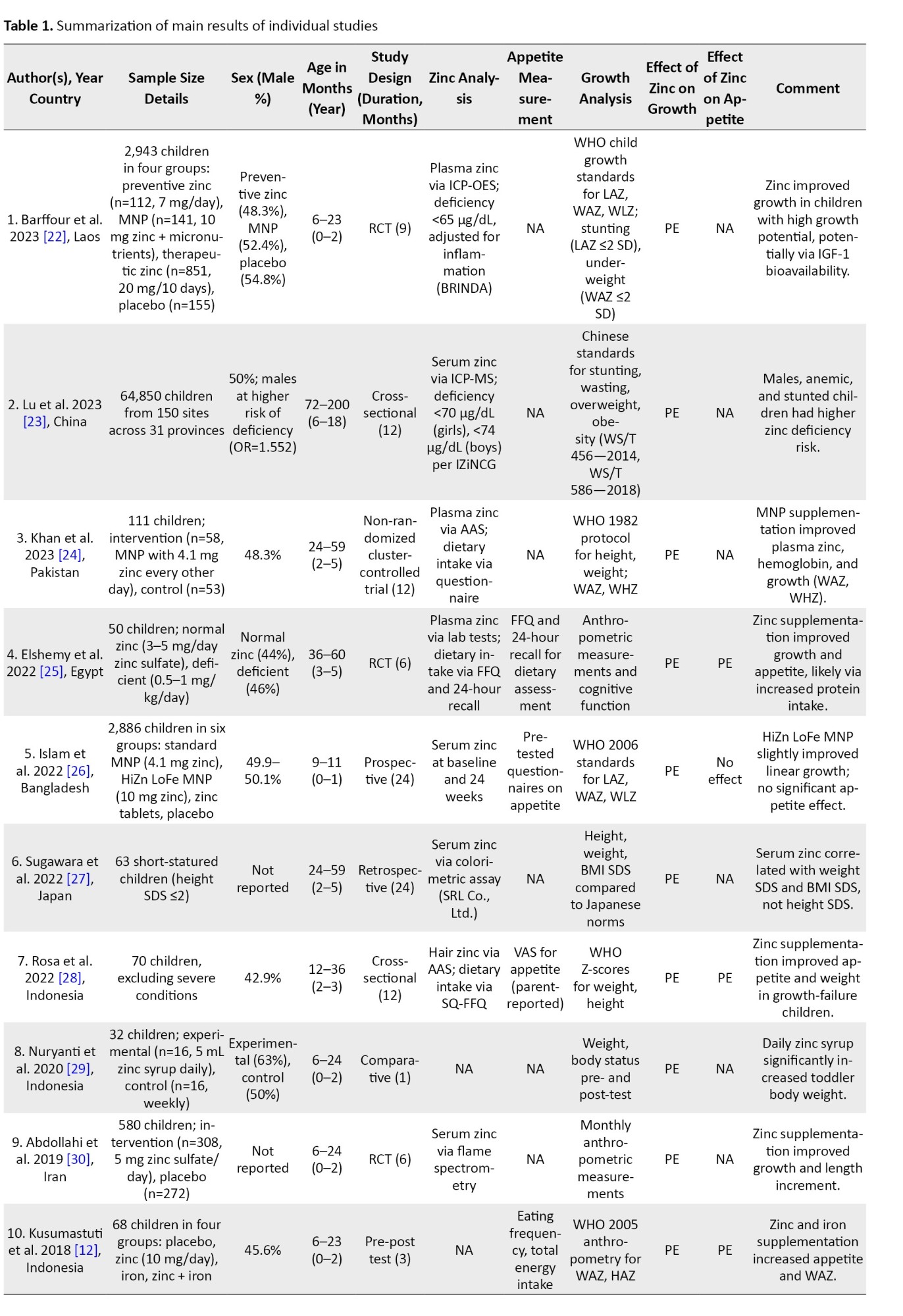
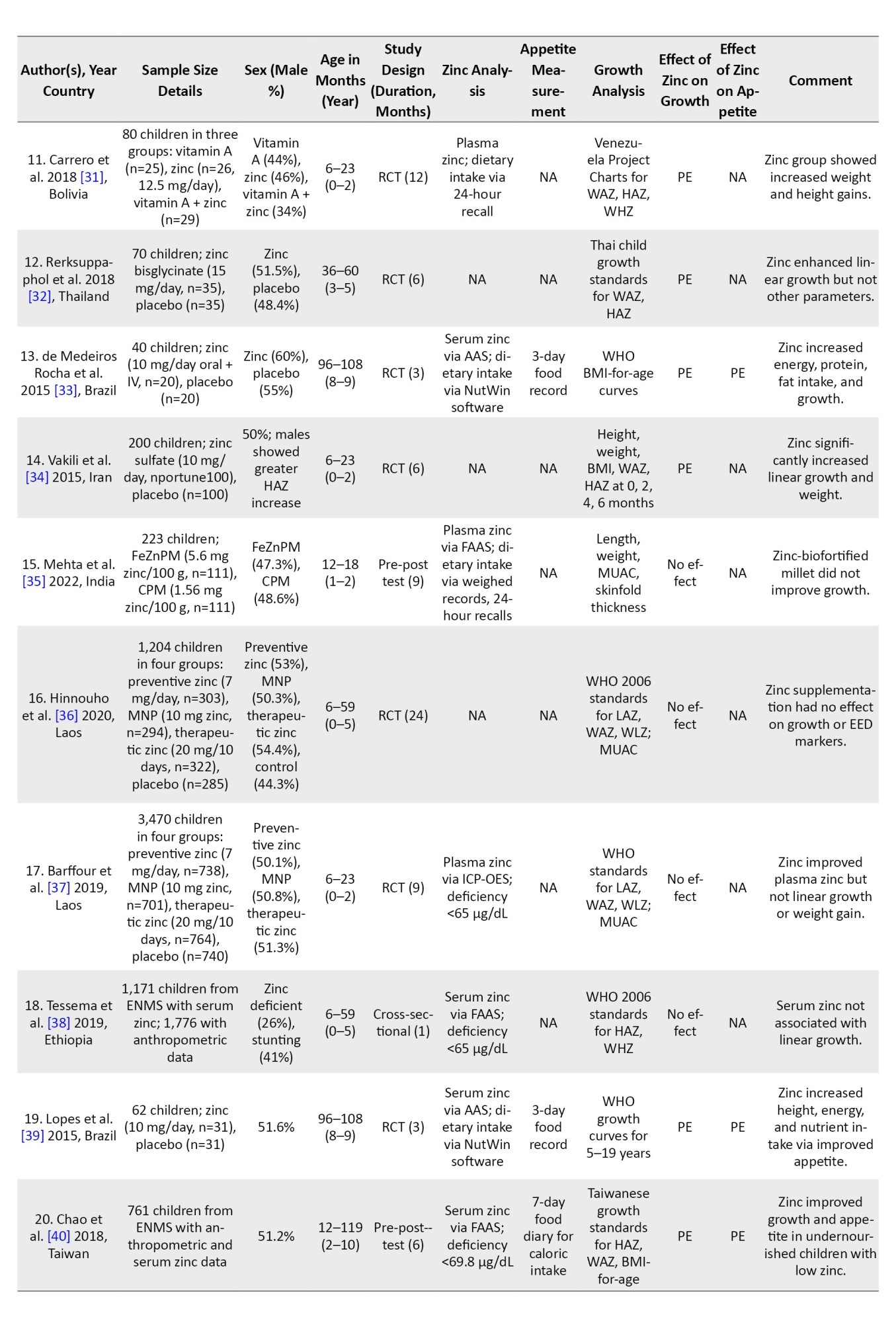
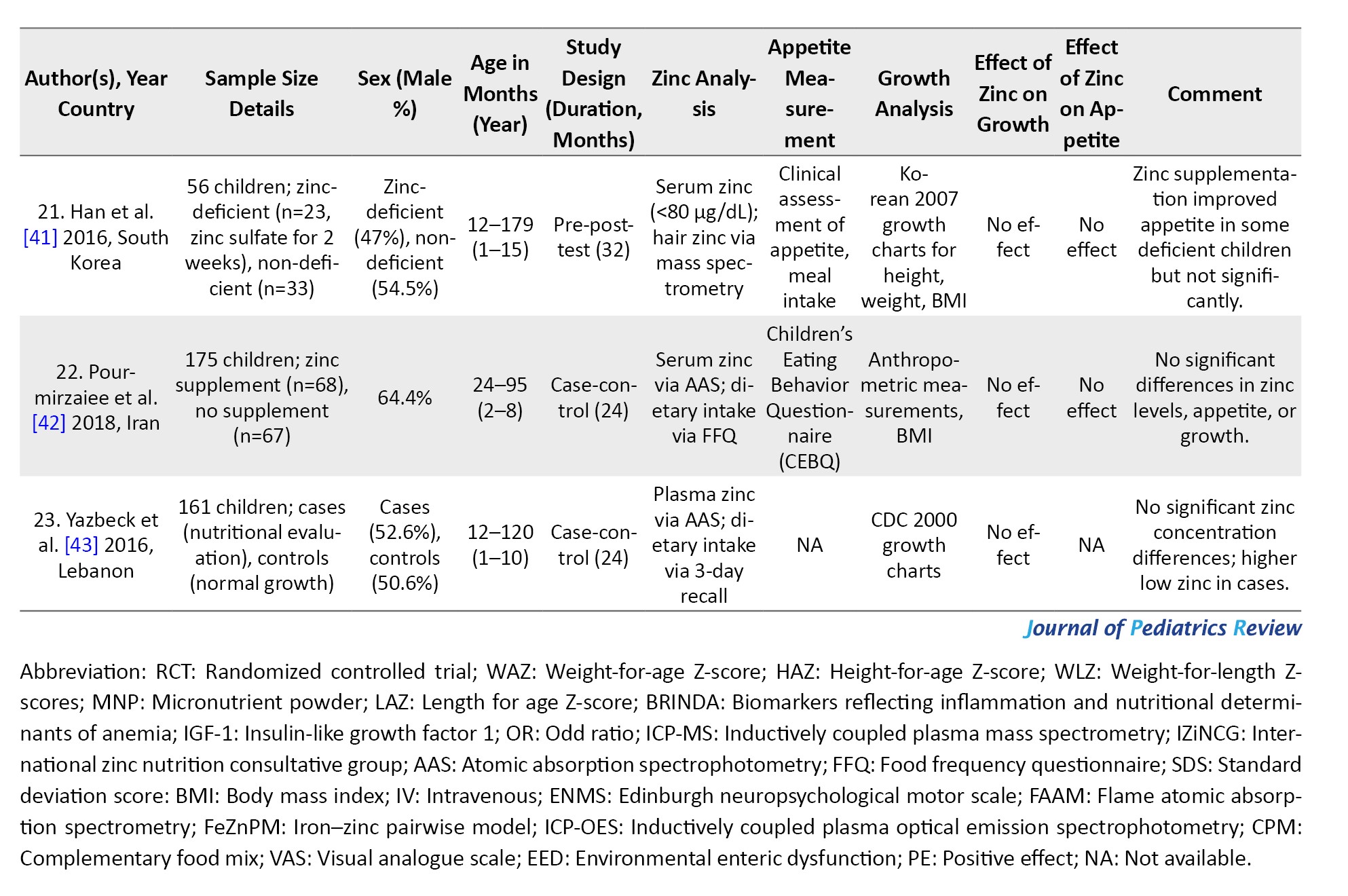
The 23 studies, conducted in Asia [12, 22-24, 26-30, 32, 34-37, 40-43), Africa [25, 38], and South America [31, 33, 39], involved 79,319 participants aged 6 months to 18 years. Study durations ranged from 1 to 24 months, with zinc supplementation doses of 3–20 mg/day administered via micronutrient powders, zinc sulfate tablets, or syrups (Table 1).
Of the 23 included studies, 16 were interventional studies (12 randomized controlled trials and 4 non-randomized trials), while 7 were observational studies, including 6 cross-sectional studies and 1 case–control study.
Baseline for zinc deficiency
Zinc deficiency was typically defined as serum or plasma zinc concentrations below 65 μg/dL, with some studies adjusting thresholds for age or inflammation according to International Zinc Nutrition Consultative Group guidelines [23, 30, 40].
Zinc level measurement
Zinc levels were measured in 18 studies using plasma or serum analysis, primarily using inductively coupled plasma optical emission spectrophotometry (ICP-OES) or atomic absorption spectrophotometry (AAS). Two studies [24, 28] used hair samples for zinc analysis, and five studies [12, 29, 31, 33, 34] did not measure zinc levels.
Zinc intake assessment
Seven studies assessed both dietary and supplemental zinc intake. For example, Elshemy et al. (2022) measured plasma zinc levels and dietary intake using food frequency questionnaires (FFQs) and 24-hour dietary recalls [25]. Some studies focused solely on supplementation [12, 26, 30, 32, 34, 40], while others relied solely on dietary intake [28].
Zinc’s effect on appetite
Five studies (55.6%, including four RCTs and one observational study) reported significant improvements in appetite, particularly in zinc-deficient children [12, 25, 28, 33, 39], while four (44.4%, including three RCTs and one observational study) found no significant effect [22, 24, 26, 42]. No studies reported any negative effects on appetite.
Zinc’s effect on growth and nutritional status
All 23 studies (12 RCTs and 11 observational studies) evaluated growth outcomes, focusing on HAZ, WAZ, and WHZ. Sixteen studies (69.6%, including nine RCTs and seven observational studies) reported significant improvements in growth, particularly in zinc-deficient or malnourished children [12, 22-33, 34, 39-40]. Seven studies (30.4%, including three RCTs and four observational studies) found no significant effect [35-38, 41- 43].
Zinc supplementation vs placebo
Ten studies (all RCTs) used placebo-controlled designs, with most (e.g. Abdollahi et al. 2019 [30]; Vakili et al. 2015 [34]) showing significant growth improvements in children receiving zinc supplementation compared to those receiving placebo.
Gender-based effects
Males were more likely to exhibit zinc deficiency [23] and showed greater growth responses to supplementation, particularly in HAZ [30, 32, 34]. In another study, boys showed more significant improvements in WAZ and WHZ [24]. Appetite improvements were not consistently gender-specific, but boys with zinc deficiency at baseline were more likely to benefit from supplementation.
Age-based effects
Children under 5 years, especially those aged 6–24 months, showed the most significant growth and appetite improvements [30, 32, 40]. Effects in school-aged children (6–18 years) were less consistent [27]. Appetite improvements were more pronounced in younger children, particularly those with growth faltering [28].
Discussion
This systematic review synthesizes evidence from 23 studies across Asia, Africa, and South America to evaluate the effects of zinc supplementation on appetite and growth in healthy children aged six months to 18 years. The findings reveal a complex relationship between zinc supplementation, appetite stimulation, and growth improvements, with outcomes varying based on baseline zinc status, population characteristics, and study design.
Main findings and implications
Zinc supplementation improved appetite in five of nine studies (all of which were RCTs), particularly in zinc-deficient children. For instance, Rosa et al. (2022) reported significant appetite enhancements in children with growth faltering following zinc supplementation [28]. These effects may stem from zinc’s role in promoting ghrelin secretion, a hormone that stimulates hunger, and in enhancing taste acuity, which increases food intake [44]. Ghrelin, released primarily in response to a negative energy balance, regulates appetite by acting on the hypothalamus and limbic system and counteracting appetite-suppressing peptides through the vagus nerve [45–47]. Additionally, zinc supports the production and release of neuropeptide Y (NPY), a key appetite regulator, and zinc deficiency may impair NPY function, potentially reducing appetite and food intake [48–50]. Elshemy et al. (2022) further confirmed that therapeutic doses of zinc sulfate improved appetite in zinc-deficient children [25]. However, four studies (two RCTs and two observational studies) found no significant appetite changes, with Barffour et al. (2023) reporting no effect despite improved plasma zinc concentrations [22]. These inconsistencies suggest that zinc’s impact on appetite is most evident in children with severe zinc deficiency or significant malnutrition, particularly in high-prevalence regions like Southeast Asia and Africa.
These findings align with prior research indicating that children with low serum zinc levels experience greater appetite improvements with supplementation [15]. However, the lack of effect in some studies highlights the need to identify specific populations and conditions where zinc supplementation is most effective. Factors, such as baseline zinc status, dietary intake, and coexisting micronutrient deficiencies, may influence outcomes.
Zinc’s effect on growth
The evidence for zinc’s effect on growth was mixed, with 16 of 23 studies (nine RCTs and seven observational studies) reporting significant improvements in growth outcomes, such as HAZ and WAZ Z-scores, particularly in zinc-deficient or malnourished children. Khan et al. (2023) observed significant increases in WAZ and WHZ after 12 months of zinc supplementation via micronutrient powders [24], while Abdollahi et al. (2019) reported enhanced height and weight gains in children receiving zinc sulfate for six months [30]. These benefits likely stem from zinc’s role in protein synthesis and its mediation of insulin-like growth factor 1 (IGF-1) bioavailability, a critical growth hormone regulator [51, 52]. Zinc also supports immune function, reducing infection-related growth setbacks, and contributes to bone development, essential for linear growth [53–56].
However, seven studies (three RCTs and four observational studies) found no significant growth effects. For example, Barffour et al. (2023) and Hinnouho et al. (2020) reported no impact on linear growth or weight gain, despite improved zinc status [22, 36]. These discrepancies may reflect variations in baseline zinc deficiency, supplementation dosage, duration, or population-specific factors, such as dietary adequacy or socioeconomic conditions. The mixed results underscore the importance of tailoring interventions to populations with confirmed zinc deficiency.
Subgroup and regional variations
Subgroup analyses indicated that children with baseline zinc deficiency or stunting benefited most from supplementation. Lu et al. (2023) found that stunted children showed greater appetite and growth responses to zinc supplementation, particularly among males, who exhibited higher deficiency rates [23]. Similarly, Khan et al. (2023) reported more significant growth improvements in boys for WAZ and WHZ [24]. These findings highlight the need to target supplementation to high-risk subgroups, such as malnourished or zinc-deficient children.
Geographical variations also influenced outcomes. Studies in Southeast Asia and Africa, where zinc deficiency prevalence is higher (20–26%), generally reported stronger effects on appetite and growth [8]. For instance, studies in Bangladesh and Pakistan reported positive effects on growth outcomes [24, 26]. In contrast, studies in regions with lower deficiency rates, such as parts of South America, often reported less pronounced effects. These regional differences emphasize the importance of context-specific interventions, particularly in areas with limited access to zinc-rich foods, such as meat and fish, where phytate-rich diets can further reduce zinc absorption [10].
Zinc deficiency and measurement methods
Most studies defined zinc deficiency as serum or plasma zinc concentrations below 65 μg/dL, consistent with the International Zinc Nutrition Consultative Group (IZiNCG) guidelines, although some studies adjusted the cut‑off values for age or inflammatory markers [57, 58]. Eighteen studies used reliable techniques, such as ICP-OES or AAS, to measure zinc levels, ensuring robust assessment. Rosa et al. (2022) employed hair analysis as a non-invasive alternative to evaluate long-term zinc status, offering a complementary approach [28]. These standardized measurement methods strengthen the reliability of zinc status assessments across studies.
Placebo-controlled studies
Ten studies utilized placebo-controlled RCT designs, providing high-quality evidence (level I). Abdollahi et al. (2019) and Vakili et al. (2015) demonstrated significant improvements in growth in zinc-supplemented groups compared to placebo, particularly in children aged 6–24 months [30, 34]. These findings reinforce zinc’s potential to address growth faltering and appetite suppression in deficient populations. The use of placebo controls also minimizes bias and enhances the validity of the results.
Conclusion
In conclusion, the evidence synthesized in this systematic review demonstrates that zinc supplementation has a significant and clinically relevant impact on appetite regulation and growth outcomes in children, particularly among those with underlying zinc deficiency, stunting, or malnutrition. The consistent positive effects observed in these high-risk subgroups underscore the role of zinc as a critical micronutrient in childhood growth and nutritional rehabilitation. Importantly, the findings indicate that zinc supplementation is most effective when implemented as a targeted intervention rather than a universal strategy.
For malnourished and zinc-deficient children, zinc supplementation should be considered an essential component of comprehensive nutritional programs designed to improve appetite, linear growth, and overall nutritional status. In contrast, for healthy children with adequate dietary intake, routine supplementation is likely unnecessary, and emphasis should be placed on ensuring sufficient zinc intake through diversified diets rich in animal-source foods.
Despite the demonstrated benefits, substantial heterogeneity across studies—particularly regarding dosage, duration, baseline nutritional status, and co-supplementation with other micronutrients—hinders the formulation of uniform clinical guidelines. This underscores the need for well-designed, standardized RCTs to define optimal supplementation protocols and clarify the mechanisms linking zinc status to appetite and growth regulation. Overall, these findings reinforce the importance of context-specific, evidence-based zinc interventions as a strategic tool to combat childhood malnutrition and support healthy growth and development, especially in regions with a high prevalence of zinc deficiency.
Limitations and future directions
Several limitations should be acknowledged. Variability in study design, zinc dosages (3–20 mg/day), and population characteristics complicates direct comparisons. While 16 studies reported positive growth effects, seven found no impact. This discrepancy may reflect the influence of confounding factors, such as dietary intake, caloric adequacy, or baseline health status, which were not fully addressed in many studies. The exclusion of some studies due to lack of access to full texts may introduce potential selection bias, although efforts were made to mitigate this limitation through interlibrary loans and author contact.
Also, the findings of the present review should be interpreted in light of the potential influence of zinc on pubertal timing. One possible explanation for the inconsistency observed across studies is variation in participants’ baseline pubertal status. Studies, including prepubertal children, may yield heterogeneous results due to ethical and physiological limits on zinc supplementation during this developmental period. This factor may partially account for the divergent outcomes reported in the literature and underscores the need for future trials to stratify analyses by pubertal stage.
Future research should prioritize long-term RCTs with standardized protocols to clarify optimal zinc supplementation strategies, including dosage, duration, and delivery methods (e.g. tablets vs micronutrient powders). Studies should also explore the synergistic effects of zinc with other micronutrients, such as iron or vitamin A, to enhance nutritional interventions [31]. Additionally, assessing dietary zinc bioavailability in phytate-rich diets, and its impact on supplementation efficacy could inform strategies in low- and middle-income countries [10]. Targeting interventions to high-risk subgroups, such as children younger than five years or those with confirmed deficiency, will maximize benefits.
Ethical Considerations
Compliance with ethical guidelines
This article is a systematic review with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflicts of interest
The authors declared no conflict of interest.
References
Zinc, an essential trace element, plays a critical role for numerous biological processes in the human body, particularly in supporting cellular growth and differentiation. This role is largely attributed to its involvement in nucleic acid and protein synthesis, as well as its influence on hormonal mediators of growth [1]. Zinc is also integral to the metabolism of proteins, lipids, and nucleic acids and contributes to gene transcription. Its wide range of functions includes roles in supporting reproduction, immune function, and wound repair. At the cellular level, zinc significantly impacts the normal functioning of macrophages, neutrophils, natural killer cells, and the complement system [2]. Furthermore, zinc serves as a structural component or catalyst in zinc metalloenzymes that regulate antioxidant defense, anti-inflammatory responses, immune function, and apoptosis [3].
Zinc deficiency is a major contributor to childhood stunting, particularly during infancy and early childhood, and is associated with several adverse health consequences, including growth retardation [4], delayed wound healing [5], increased susceptibility to infectious diseases [6], and impaired cognitive function [7]. Zinc deficiency is a significant public health issue in nearly all low- and middle-income countries, with an estimated prevalence ranging from 20% to 26% among children [8]. The main causes of zinc deficiency include inadequate consumption of zinc-rich foods, increased requirements or losses, malabsorption, and impaired zinc utilization. In healthy infants, zinc needs are typically met through breast milk during the first 6 months of life. However, beyond this period, complementary foods must provide sufficient zinc to support optimal growth and development, as breast milk alone may no longer be adequate [9]. Zinc is abundant in foods, such as meat, fish, poultry, and oysters; however, its bioavailability is reduced by dietary components, such as phytates—inositol phosphates found in cereals, grains, seeds, and legumes—which form poorly soluble complexes with zinc and inhibit its absorption. Diets high in phytates, common in many low- and middle-income countries, thus increase the risk of zinc deficiency, particularly where access to high-zinc foods is limited [10].
Globally, approximately 17.3% of the population is estimated to be at risk of inadequate zinc intake [11]. This issue is particularly concerning in pediatric populations, where zinc deficiency has been reported in 20–26% of otherwise healthy children, underscoring the need for enhanced monitoring and intervention strategies [12]. Zinc has been shown to influence appetite by enhancing ghrelin secretion, a hormone that stimulates hunger [13, 14]. Additionally, low zinc status may impair taste acuity and increase stress and anxiety in children, potentially reducing appetite and food intake, thereby exacerbating nutritional deficiencies [12, 15].
In addition to its well-known role in appetite regulation and growth, zinc is involved in the modulation of the hypothalamic–pituitary–gonadal axis. Emerging evidence suggests that excessive zinc exposure during sensitive developmental periods may be associated with earlier activation of pubertal pathways. This biological consideration has led to clinical caution regarding routine zinc supplementation before the onset of puberty, particularly in otherwise healthy children [16].
Multiple studies have been conducted to assess the effect of zinc on children’s growth; however, their findings are inconsistent, with variations attributed to differences in study populations, intervention types, and settings. Previous systematic reviews on this topic have highlighted significant variability in participant characteristics, intervention protocols, and outcome measures, making it challenging to provide clear, evidence-based conclusions about the efficacy and safety of zinc supplementation for improving linear growth and appetite in children [14]. Therefore, this systematic review aimed to synthesize the available evidence and address the specific question of how zinc intake, through diet or supplementation, impacts appetite and growth in healthy children aged 6 months to 18 years.
Materials and Methods
Protocol and registration
This systematic review followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines [17] and was registered in the International Prospective Register of Systematic Reviews (PROSPERO CRD42024578984). Ethical approval and patient consent were not required because all analyses were based on previously published studies.
Eligibility criteria
Type of studies: We included observational studies (cross‑sectional, case–control, and cohort studies), prospective and retrospective studies, and randomized controlled trials (RCTs) assessing zinc intake (dietary or supplemental, including medicinal or food fortification) and its relationship with appetite or growth in healthy children. The exclusion criteria were letters, conference proceedings, reviews, duplicated data, animal studies, and studies lacking relevant data. To minimize bias, we attempted to obtain full texts through institutional access, interlibrary loans, or author contact; however, 14 studies were excluded due to inaccessible full texts, potentially introducing selection bias.
Study population: Healthy children and adolescents aged 6 months to 18 years were eligible. Studies on infants younger than six months or children with chronic illnesses were excluded to focus on healthy populations.
Outcome parameters: Studies were included if they reported outcomes related to appetite, weight-for-age Z-score (WAZ), height-for-age Z-scores (HAZ), linear growth, weight-for-length Z-scores (WLZ), or body mass index (BMI)-for-age.
Information sources and search
We searched PubMed, Web of Science, and Scopus for studies published from April 2015 to January 2024, using terms such as “zinc”, “dietary zinc”, “zinc intake”, “serum zinc”, “zinc supplementation”, “zinc supplements”, “poor appetite”, “appetite”, “anorexia”, “nutritional status”, “food intake”, “eating”, “food consumption”, “energy intake”, “growth”, “growth development”, “malnutrition”, “body height”, “body weight”, “body mass index”, “child”, “children”, “toddler”, “pediatrics”, “adolescent”, “infant”. Reference lists of all included papers and relevant reviews were screened for additional citations [18]. The search identified 1,797 articles, which were managed using Endnote 20.0 to remove duplicates. Titles and abstracts of the identified studies were scanned in duplicate to exclude irrelevant references. Titles, abstracts, and full texts were screened independently by two authors to ensure eligibility, with disputes resolved through consensus. Twenty‑three studies met the eligibility criteria and were included in the final review (Figure 1).
Search strategy
PubMed
Search terms: ((“zinc”[Mesh] OR “dietary zinc” OR “zinc intake” OR “serum zinc” OR “zinc supplementation” OR “zinc supplements”) AND (“poor appetite” OR “appetite”[Mesh] OR “anorexia”[Mesh] OR “nutritional status”[Mesh] OR “food intake” OR “eating”[Mesh] OR “food consumption” OR “energy intake”[Mesh] OR “growth”[Mesh] OR “growth development”[Mesh] OR “malnutrition”[Mesh] OR “body height”[Mesh] OR “body weight”[Mesh] OR “body mass index”[Mesh]) AND (“child”[Mesh] OR “children” OR “toddler” OR “pediatrics”[Mesh] OR “adolescent”[Mesh] OR “infant”[Mesh]))
Search timeframe: January 2015-January 2024, Total articles identified: 616.
Web of Science
Search terms: TS=(“Zinc” OR “dietary zinc” OR “zinc intake” OR “serum zinc” OR “zinc supplementation” OR “zinc supplements”) AND
TS=(“Poor appetite” OR “appetite” OR “anorexia” OR “nutritional status” OR “food intake” OR “eating” OR “food consumption” OR “energy intake” OR “growth” OR “growth development” OR “malnutrition” OR “body height” OR “body weight” OR “body mass index”) AND
TS=(“Child” OR “children” OR “toddler” OR “pediatrics” OR “adolescent” OR “infant”)
Search timeframe: January 2015-January 2024, Total articles identified: 367.
Scopus
Search terms: (TITLE-ABS-KEY(“zinc” OR “dietary zinc” OR “zinc intake” OR “serum zinc” OR “zinc supplementation” OR “zinc supplements”) AND
TITLE-ABS-KEY(“poor appetite” OR “appetite” OR “anorexia” OR “nutritional status” OR “food intake” OR “eating” OR “food consumption” OR “energy intake” OR “growth” OR “growth development” OR “malnutrition” OR “body height” OR “body weight” OR “body mass index”) AND
TITLE-ABS-KEY(“child” OR “children” OR “toddler” OR “pediatrics” OR “adolescent” OR “infant”))
Search timeframe: January 2015-January 2024, Total articles identified: 814.
Selection of studies
Two authors independently screened and assessed the eligibility of the studies, extracted relevant data, and assessed the risk of bias for all included studies. Disagreements were resolved through discussion until consensus was reached.
Data collection process
Data were collected independently by two authors, who reviewed and consolidated the data from the included studies.
Assessment of risk of bias
In this review, all studies underwent critical appraisal by one review team member (X) using the Joanna Briggs Institute critical appraisal checklists [19]. This tool was chosen because it can be used to assess descriptive cross-sectional studies as well as randomized controlled trials [20, 21]. A second reviewer (Y) blinded to the first reviewer’s (X) assessments checked a random 15% of the included articles for risk of bias, and any differences between the reviewers were discussed and resolved. Figure 2 shows the reviewers’ judgments about each risk of bias item for each included study.
Synthesis of results
The results were synthesized based on the extracted data, and findings were analyzed to provide insights into the effect of zinc on appetite and growth in children.
Results
Study selection
A total of 1,797 articles were identified (616 from PubMed, 814 from Scopus, and 367 from Web of Science). After removing 427 duplicates, 1,370 abstracts were screened, and 621 articles unrelated to zinc, growth, or appetite in children were excluded, along with 658 additional irrelevant records. Of the remaining 91 articles, the full texts were reviewed, and 68 were excluded: 14 due to unavailable full texts, 21 for irrelevance, 26 for not reporting growth outcomes or focusing on infants under 6 months, and 7 for including non-healthy children. Twenty-three studies [12, 22-43] were included (Figure 1).
Characteristics of included studies
The 23 studies, conducted in Asia [12, 22-24, 26-30, 32, 34-37, 40-43), Africa [25, 38], and South America [31, 33, 39], involved 79,319 participants aged 6 months to 18 years. Study durations ranged from 1 to 24 months, with zinc supplementation doses of 3–20 mg/day administered via micronutrient powders, zinc sulfate tablets, or syrups (Table 1).
Of the 23 included studies, 16 were interventional studies (12 randomized controlled trials and 4 non-randomized trials), while 7 were observational studies, including 6 cross-sectional studies and 1 case–control study.
Baseline for zinc deficiency
Zinc deficiency was typically defined as serum or plasma zinc concentrations below 65 μg/dL, with some studies adjusting thresholds for age or inflammation according to International Zinc Nutrition Consultative Group guidelines [23, 30, 40].
Zinc level measurement
Zinc levels were measured in 18 studies using plasma or serum analysis, primarily using inductively coupled plasma optical emission spectrophotometry (ICP-OES) or atomic absorption spectrophotometry (AAS). Two studies [24, 28] used hair samples for zinc analysis, and five studies [12, 29, 31, 33, 34] did not measure zinc levels.
Zinc intake assessment
Seven studies assessed both dietary and supplemental zinc intake. For example, Elshemy et al. (2022) measured plasma zinc levels and dietary intake using food frequency questionnaires (FFQs) and 24-hour dietary recalls [25]. Some studies focused solely on supplementation [12, 26, 30, 32, 34, 40], while others relied solely on dietary intake [28].
Zinc’s effect on appetite
Five studies (55.6%, including four RCTs and one observational study) reported significant improvements in appetite, particularly in zinc-deficient children [12, 25, 28, 33, 39], while four (44.4%, including three RCTs and one observational study) found no significant effect [22, 24, 26, 42]. No studies reported any negative effects on appetite.
Zinc’s effect on growth and nutritional status
All 23 studies (12 RCTs and 11 observational studies) evaluated growth outcomes, focusing on HAZ, WAZ, and WHZ. Sixteen studies (69.6%, including nine RCTs and seven observational studies) reported significant improvements in growth, particularly in zinc-deficient or malnourished children [12, 22-33, 34, 39-40]. Seven studies (30.4%, including three RCTs and four observational studies) found no significant effect [35-38, 41- 43].
Zinc supplementation vs placebo
Ten studies (all RCTs) used placebo-controlled designs, with most (e.g. Abdollahi et al. 2019 [30]; Vakili et al. 2015 [34]) showing significant growth improvements in children receiving zinc supplementation compared to those receiving placebo.
Gender-based effects
Males were more likely to exhibit zinc deficiency [23] and showed greater growth responses to supplementation, particularly in HAZ [30, 32, 34]. In another study, boys showed more significant improvements in WAZ and WHZ [24]. Appetite improvements were not consistently gender-specific, but boys with zinc deficiency at baseline were more likely to benefit from supplementation.
Age-based effects
Children under 5 years, especially those aged 6–24 months, showed the most significant growth and appetite improvements [30, 32, 40]. Effects in school-aged children (6–18 years) were less consistent [27]. Appetite improvements were more pronounced in younger children, particularly those with growth faltering [28].
Discussion
This systematic review synthesizes evidence from 23 studies across Asia, Africa, and South America to evaluate the effects of zinc supplementation on appetite and growth in healthy children aged six months to 18 years. The findings reveal a complex relationship between zinc supplementation, appetite stimulation, and growth improvements, with outcomes varying based on baseline zinc status, population characteristics, and study design.
Main findings and implications
Zinc supplementation improved appetite in five of nine studies (all of which were RCTs), particularly in zinc-deficient children. For instance, Rosa et al. (2022) reported significant appetite enhancements in children with growth faltering following zinc supplementation [28]. These effects may stem from zinc’s role in promoting ghrelin secretion, a hormone that stimulates hunger, and in enhancing taste acuity, which increases food intake [44]. Ghrelin, released primarily in response to a negative energy balance, regulates appetite by acting on the hypothalamus and limbic system and counteracting appetite-suppressing peptides through the vagus nerve [45–47]. Additionally, zinc supports the production and release of neuropeptide Y (NPY), a key appetite regulator, and zinc deficiency may impair NPY function, potentially reducing appetite and food intake [48–50]. Elshemy et al. (2022) further confirmed that therapeutic doses of zinc sulfate improved appetite in zinc-deficient children [25]. However, four studies (two RCTs and two observational studies) found no significant appetite changes, with Barffour et al. (2023) reporting no effect despite improved plasma zinc concentrations [22]. These inconsistencies suggest that zinc’s impact on appetite is most evident in children with severe zinc deficiency or significant malnutrition, particularly in high-prevalence regions like Southeast Asia and Africa.
These findings align with prior research indicating that children with low serum zinc levels experience greater appetite improvements with supplementation [15]. However, the lack of effect in some studies highlights the need to identify specific populations and conditions where zinc supplementation is most effective. Factors, such as baseline zinc status, dietary intake, and coexisting micronutrient deficiencies, may influence outcomes.
Zinc’s effect on growth
The evidence for zinc’s effect on growth was mixed, with 16 of 23 studies (nine RCTs and seven observational studies) reporting significant improvements in growth outcomes, such as HAZ and WAZ Z-scores, particularly in zinc-deficient or malnourished children. Khan et al. (2023) observed significant increases in WAZ and WHZ after 12 months of zinc supplementation via micronutrient powders [24], while Abdollahi et al. (2019) reported enhanced height and weight gains in children receiving zinc sulfate for six months [30]. These benefits likely stem from zinc’s role in protein synthesis and its mediation of insulin-like growth factor 1 (IGF-1) bioavailability, a critical growth hormone regulator [51, 52]. Zinc also supports immune function, reducing infection-related growth setbacks, and contributes to bone development, essential for linear growth [53–56].
However, seven studies (three RCTs and four observational studies) found no significant growth effects. For example, Barffour et al. (2023) and Hinnouho et al. (2020) reported no impact on linear growth or weight gain, despite improved zinc status [22, 36]. These discrepancies may reflect variations in baseline zinc deficiency, supplementation dosage, duration, or population-specific factors, such as dietary adequacy or socioeconomic conditions. The mixed results underscore the importance of tailoring interventions to populations with confirmed zinc deficiency.
Subgroup and regional variations
Subgroup analyses indicated that children with baseline zinc deficiency or stunting benefited most from supplementation. Lu et al. (2023) found that stunted children showed greater appetite and growth responses to zinc supplementation, particularly among males, who exhibited higher deficiency rates [23]. Similarly, Khan et al. (2023) reported more significant growth improvements in boys for WAZ and WHZ [24]. These findings highlight the need to target supplementation to high-risk subgroups, such as malnourished or zinc-deficient children.
Geographical variations also influenced outcomes. Studies in Southeast Asia and Africa, where zinc deficiency prevalence is higher (20–26%), generally reported stronger effects on appetite and growth [8]. For instance, studies in Bangladesh and Pakistan reported positive effects on growth outcomes [24, 26]. In contrast, studies in regions with lower deficiency rates, such as parts of South America, often reported less pronounced effects. These regional differences emphasize the importance of context-specific interventions, particularly in areas with limited access to zinc-rich foods, such as meat and fish, where phytate-rich diets can further reduce zinc absorption [10].
Zinc deficiency and measurement methods
Most studies defined zinc deficiency as serum or plasma zinc concentrations below 65 μg/dL, consistent with the International Zinc Nutrition Consultative Group (IZiNCG) guidelines, although some studies adjusted the cut‑off values for age or inflammatory markers [57, 58]. Eighteen studies used reliable techniques, such as ICP-OES or AAS, to measure zinc levels, ensuring robust assessment. Rosa et al. (2022) employed hair analysis as a non-invasive alternative to evaluate long-term zinc status, offering a complementary approach [28]. These standardized measurement methods strengthen the reliability of zinc status assessments across studies.
Placebo-controlled studies
Ten studies utilized placebo-controlled RCT designs, providing high-quality evidence (level I). Abdollahi et al. (2019) and Vakili et al. (2015) demonstrated significant improvements in growth in zinc-supplemented groups compared to placebo, particularly in children aged 6–24 months [30, 34]. These findings reinforce zinc’s potential to address growth faltering and appetite suppression in deficient populations. The use of placebo controls also minimizes bias and enhances the validity of the results.
Conclusion
In conclusion, the evidence synthesized in this systematic review demonstrates that zinc supplementation has a significant and clinically relevant impact on appetite regulation and growth outcomes in children, particularly among those with underlying zinc deficiency, stunting, or malnutrition. The consistent positive effects observed in these high-risk subgroups underscore the role of zinc as a critical micronutrient in childhood growth and nutritional rehabilitation. Importantly, the findings indicate that zinc supplementation is most effective when implemented as a targeted intervention rather than a universal strategy.
For malnourished and zinc-deficient children, zinc supplementation should be considered an essential component of comprehensive nutritional programs designed to improve appetite, linear growth, and overall nutritional status. In contrast, for healthy children with adequate dietary intake, routine supplementation is likely unnecessary, and emphasis should be placed on ensuring sufficient zinc intake through diversified diets rich in animal-source foods.
Despite the demonstrated benefits, substantial heterogeneity across studies—particularly regarding dosage, duration, baseline nutritional status, and co-supplementation with other micronutrients—hinders the formulation of uniform clinical guidelines. This underscores the need for well-designed, standardized RCTs to define optimal supplementation protocols and clarify the mechanisms linking zinc status to appetite and growth regulation. Overall, these findings reinforce the importance of context-specific, evidence-based zinc interventions as a strategic tool to combat childhood malnutrition and support healthy growth and development, especially in regions with a high prevalence of zinc deficiency.
Limitations and future directions
Several limitations should be acknowledged. Variability in study design, zinc dosages (3–20 mg/day), and population characteristics complicates direct comparisons. While 16 studies reported positive growth effects, seven found no impact. This discrepancy may reflect the influence of confounding factors, such as dietary intake, caloric adequacy, or baseline health status, which were not fully addressed in many studies. The exclusion of some studies due to lack of access to full texts may introduce potential selection bias, although efforts were made to mitigate this limitation through interlibrary loans and author contact.
Also, the findings of the present review should be interpreted in light of the potential influence of zinc on pubertal timing. One possible explanation for the inconsistency observed across studies is variation in participants’ baseline pubertal status. Studies, including prepubertal children, may yield heterogeneous results due to ethical and physiological limits on zinc supplementation during this developmental period. This factor may partially account for the divergent outcomes reported in the literature and underscores the need for future trials to stratify analyses by pubertal stage.
Future research should prioritize long-term RCTs with standardized protocols to clarify optimal zinc supplementation strategies, including dosage, duration, and delivery methods (e.g. tablets vs micronutrient powders). Studies should also explore the synergistic effects of zinc with other micronutrients, such as iron or vitamin A, to enhance nutritional interventions [31]. Additionally, assessing dietary zinc bioavailability in phytate-rich diets, and its impact on supplementation efficacy could inform strategies in low- and middle-income countries [10]. Targeting interventions to high-risk subgroups, such as children younger than five years or those with confirmed deficiency, will maximize benefits.
Ethical Considerations
Compliance with ethical guidelines
This article is a systematic review with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflicts of interest
The authors declared no conflict of interest.
References
- Ceballos-Rasgado M, Lowe NM, Moran VH, Clegg A, Mallard S, Harris C, et al. Toward revising dietary zinc recommendations for children aged 0 to 3 years: A systematic review and meta-analysis of zinc absorption, excretion, and requirements for growth. Nutr Rev. 2023; 81(8):967-87. [DOI:10.1093/nutrit/nuac098] [PMID]
- Maxfield L, Shukla S, Crane JS. Zinc Deficiency. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [Updated 2024 Sep 13]. Available from: [Link]
- Liu E, Pimpin L, Shulkin M. Effect of zinc supplementation on growth outcomes in children under 5 years of age. Nutrients. 2018; 10(377). [DOI:10.3390/nu10030377] [PMID]
- Imdad A, Bhutta ZA. Effect of preventive zinc supplementation on linear growth in children under 5 years of age in developing countries: A meta-analysis of studies for input to the lives saved tool. BMC Public Health. 2011; 11(Suppl 3):S22. [DOI:10.1186/1471-2458-11-S3-S22] [PMID]
- Kogan S, Sood A, Garnick MS. Zinc and wound healing: a review of zinc physiology and clinical applications. Wounds. 2017; 29:102-6. [PMID]
- Yakoob MY, Theodoratou E, Jabeen A. Preventive zinc supplementation in developing countries: Impact on mortality and morbidity due to diarrhea, pneumonia and malaria. BMC Public Health. 2011; 11(suppl 3). [DOI:10.1186/1471-2458-11-S3-S23] [PMID]
- Warthon-Medina M, Moran VH, Stammers AL. Zinc intake, status and indices of cognitive function in adults and children: a systematic review and metaanalysis. Eur J Clin Nutr. 2015; 69:649-61. [DOI:10.1038/ejcn.2015.60] [PMID]
- Ackland ML, Michalczyk AA. Zinc and infant nutrition. Arch Biochem Biophys. 2016; 611:51-7. [DOI:10.1016/j.abb.2016.06.011] [PMID]
- Gera T, Shah D, Sachdev HS. Zinc Supplementation for Promoting Growth in Children Under 5 years of age in Low- and Middle-income Countries: A Systematic Review. Indian Pediatr. 2019; 56(5):391-406. [DOI:10.1007/s13312-019-1537-z] [PMID]
- Kennedy C, Chukwuebuka N, Uchenna E. Serum zinc levels in apparently healthy children in Nigeria: Are they acceptable. Niger Med J. 2020; 61(6). [DOI:10.4103/nmj.NMJ_20_20] [PMID]
- Wessells KR, Brown KH. Estimating the global prevalence of zinc deficiency: Results based on zinc availability in national food supplies and the prevalence of stunting. PLoS ONE. 2012; 7(11):e50568. [DOI:10.1371/journal.pone.0050568] [PMID]
- Kusumastuti AC, Ardiaria M, Hendrianingtyas M. Effect of zinc and iron supplementation on appetite, nutritional status and intelligence quotient in young children. Indones Biomed J. 2018; 10(2):133-9. [DOI:10.18585/inabj.v10i2.365]
- Yin J, Li X, Li D, Yue T, Fang Q, Ni J, et al. Dietary supplementation with zinc oxide stimulates ghrelin secretion from the stomach of young pigs. J Nutr Biochem. 2009; 20(10):783-90. [DOI:10.1016/j.jnutbio.2008.07.007] [PMID]
- Mayo-Wilson E, Junior JA, Imdad A, Dean S, Chan XHS, Chan ES, et al. Zinc supplementation for preventing mortality, morbidity, and growth failure in children aged 6 months to 12 years of age. Cochrane Database Syst Rev. 2014; (5):CD009384. [DOI:10.1002/14651858.CD009384.pub2]
- Khademian M, Farhangpajouh N, Shahsanaee A, Bahreynian M, Kelishadi MM, R. Effects of zinc supplementation on subscales of anorexia in children: A randomized controlled trial. Pak J Med Sci. 2014; 30:1213-7. [PMID]
- Karaca Z, Tanriverdi F, Kurtoglu S, Tokalioglu S, Unluhizarci K, Kelestimur F. Pubertal arrest due to Zn deficiency. The effect of zinc supplementation. Hormones (Athens). 2007;6(1):71. [PMID]
- Editorial PDV. Review articles, systematic reviews, meta-analysis, and the updated preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 Guidelines. Med Sci Monit. 2021; 27:e934475. [DOI:10.12659/MSM.934475]
- Moher D, Liberati A, Tetzlaff J, Altman DG, Group PRISMA. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann Intern Med. 2009; 18;151(4):264-9. [DOI:10.7326/0003-4819-151-4-200908180-00135] [PMID]
- Institute JB. Critical appraisal tools (Checklist for analytical cross sectional studies, checklist for case control studies, checklist for case reports, checklist for case series, checklist for cohort studies, checklist for prevalence studies, checklist for quasi-experimental studies, checklist for randomized controlled trials [Internet]. 2020 [Updated 24 May 2026]. Available from: [Link]
- Ma LL, Wang YY, Yang ZH. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil Med Res. 2020; 7(7). [DOI:10.1186/s40779-020-00238-8] [PMID]
- McGuinness LA, Higgins JPT. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res Syn Meth. 2020; 1-7. [DOI:10.1002/jrsm.1411] [PMID]
- Barffour MA, Bernstein RM, Hinnouho GM, Wessells KR, Arnold CD, Kounnavong S, et al. Insulin-like Growth Factor 1 (IGF1), IGF Binding Protein-3 (IGFBP3) and Growth Response to Daily Zinc Supplementation: A Randomized Trial in Rural Laotian Children. Nutrients. 2023; 15(11). [DOI:10.3390/nu15112590] [PMID]
- Lu J, Zhang H, Cao W, Jiang S, Fang H, Yu D, et al. Study on the zinc nutritional status and risk factors of chinese 6-18-year-old children. Nutrients. 2023; 15(7). [DOI:10.3390/nu15071685] [PMID]
- Khan A, Ul-Haq Z, Fatima S, Ahmed J, Alobaid HM, Fazid S, et al. Long-term impact of multiple micronutrient supplementation on micronutrient status, hemoglobin level, and growth in children 24 to 59 months of age: a non-randomized community-based trial from Pakistan. Nutrients. 2023; 15(7). [DOI:10.3390/nu15071690] [PMID]
- Elshemy AN, Aboulghar HM, Mowafy MA, Ahmed ME, Mohamed MS. The effect of zinc supplementation on improving cognitive and nutrition status among preschool children coming to family medicine center clinic in Nikla Village at Giza. Indian J Forensic Med Toxicol. 2020; 30;14(3):1769-76. [DOI: 10.37506/ijfmt.v14i3.10672]
- Islam MM, Black RE, Krebs NF, Westcott J, Long J, Islam KM, et al. Different doses, forms, and frequencies of zinc supplementation for the prevention of diarrhea and promotion of linear growth among young bangladeshi children: A six-arm, randomized, community-based efficacy trial. J Nutr. 2022; 152(5):1306-15. [DOI:10.1093/jn/nxab439] [PMID]
- Zheng Y, Yang L, Wu Z, Zhu H, Xiao B, Li Z, et al. Assessment of dietary nutrient intake and its relationship to the nutritional status of children with congenital heart disease in Guangdong province of China. Asia Pac J Clin Nutr. 2022; 31(3):520-5. [DOI:10.6133/apjcn.202209_31(3).0019] [PMID]
- Rosa AI, Sunardi D, Hardiany NS. Correlation of zinc intake with hair zinc levels and appetite in children aged 2-3 years in Jakarta. World Nutr J. 2022; 5(2):23-31. [DOI:10.25220/WNJ.V05.i2.0005]
- Nuryanti E, Titah Normawati A. The influence of zinc supplement in feeding patterns on the incidence of stunted in the toddler. Syst Rev Pharm. 2020; 11(5):680-2. [DOI: 10.31838/srp.2020.5.96]
- Abdollahi M, Ajami M, Abdollahi Z, Kalantari N, Houshiarrad A, Fozouni F, et al. Zinc supplementation is an effective and feasible strategy to prevent growth retardation in 6 to 24 month children: A pragmatic double blind, randomized trial. Heliyon. 2019; 5(11). [DOI:10.1016/j.heliyon.2019.e02581] [PMID]
- Carrero C, Leal J, Ortega P, Parody A, Montilla M, Sierra L, et al. Effect of Vitamin A, Zinc and multivitamin supplementation on the nutritional status and retinol serum values in school-age children. In Springer Verlag. 2018; 748-58. [DOI:10.1007/978-3-319-93803-5_70]
- Rerksuppaphol S, Rerksuppaphol L. Zinc supplementation enhances linear growth in school-aged children: A randomized controlled trial. Pediatr Rep. 2017; 9(4). [DOI:10.4081/pr.2017.7294] [PMID]
- Rocha A, Iñiguez G, Godoy C, Gaete X, López P, Loreti N, et al. Testicular function during adolescence in boys with type 1 diabetes mellitus (T1D): Absence of hypogonadism and differences in endocrine profile at the beginning and end of puberty. Pediatr Diabetes. 2014; 15(3):198-205. [DOI:10.1111/pedi.12078] [PMID]
- Vakili R, Yazdan Bakhsh M, Vahedian M, Mahmoudi M, Saeidi M, Vakili S. The effect of zinc supplementation on linear growth and growth factors in primary schoolchildren in the suburbs Mashhad, Iran. J Ped Pers. 2015; 3(2.1): 1-7. [DOI:10.22038/ijp.2015.3931]
- Mehta S, Huey SL, Ghugre PS, Potdar RD, Venkatramanan S, Krisher JT, et al. A randomized trial of iron- and zinc-biofortified pearl millet-based complementary feeding in children aged 12 to 18 months living in urban slums. Clin Nutr. 2022; 41(4):937-47. [DOI:10.1093/cdn/nzac060.035]
- Hinnouho GM, Ryan Wessells K, Barffour MA, Sayasone S, Arnold CD, Kounnavong S, et al. Impact of different strategies for delivering supplemental zinc on selected fecal markers of environmental enteric dysfunction among young laotian children: A randomized controlled trial. Am J Trop Med Hyg. 2020; 103(4):1416-26. [DOI:10.4269/ajtmh.20-0106] [PMID]
- Barffour MA, Hinnouho GM, Kounnavong S, Wessells R, Ratsavong K, Bounheuang B, et al. Effects of daily zinc, daily multiple micronutrient powder, or therapeutic zinc supplementation for diarrhea prevention on physical growth, anemia, and micronutrient status in rural laotian children: A randomized controlled trial. J Pediatr. 2018; 207:80-89.e2. [DOI:10.1016/j.jpeds.2018.11.022] [PMID]
- Tessema M, De Groote H, Brouwer ID, Feskens EJM, Belachew T, Zerfu D, et al. Soil zinc is associated with serum zinc but not with linear growth of children in Ethiopia. Nutrients. 2019; 11(2). [DOI:10.3390/nu11020221] [PMID]
- Lopes M, De Brito N, De Medeiros Rocha É, França MC, Das Graças De Almeida M, et al. Nutritional assessment methods for zinc supplementation in prepubertal non-zinc-deficient children. Food Nutr Res. 2015; 59. [DOI:10.3402/fnr.v59.29733] [PMID]
- Chao HC, Chang YJ, Huang WL. Cut-off serum zinc concentration affecting the appetite, growth, and nutrition status of undernourished children supplemented with zinc. Nutr Clin Pract Off Publ Am Soc Parenter Enter Nutr. 2018; 33(5):701-10. [DOI:10.1002/ncp.10079] [PMID]
- Han TH, Lee J, Kim YJ. Hair zinc level analysis and correlative micronutrients in children presenting with malnutrition and poor growth. Pediatr Gastroenterol Hepatol Nutr. 2016; 19(4):259-68. [DOI:10.5223/pghn.2016.19.4.259] [PMID]
- Pourmirzaiee MA, Chehrazi S, Heidari-Beni M, Kelishadi R. Serum zinc level and eating behaviors in children receiving zinc supplements without physician prescription. Adv Biomed Res. 2018; 7:120. [DOI:10.4103/abr.abr_77_18] [PMID]
- Yazbeck N, Hanna-Wakim R, El Rafei R, Barhoumi A, Farra C, Daher RT, et al. Dietary zinc intake and plasma zinc concentrations in children with short stature and failure to thrive. Ann Nutr Metab. 2016; 69(1):9-14. [DOI:10.1159/000447648] [PMID]
- Suzuki H, Asakawa A, Li JB, Tsai M, Amitani H, Ohinata K, et al. Zinc as an appetite stimulator - the possible role of zinc in the progression of diseases such as cachexia and sarcopenia. Recent Pat Food Nutr Agric. 2011; 3(3):226-31. [DOI:10.2174/2212798411103030226] [PMID]
- Ueno H, Nakazato M. Mechanistic relationship between the vagal afferent pathway, central nervous system and peripheral organs in appetite regulation. J Diabetes Investig. 2016; 7(6):812-8. [DOI:10.1111/jdi.12492] [PMID]
- Norman K, Haß U, Pirlich M. Malnutrition in older adults-recent advances and remaining challenges. Nutrients. 2021; 13(8):2764. [DOI:10.3390/nu13082764] [PMID]
- Kirsz K, Zieba DA. Ghrelin-mediated appetite regulation in the central nervous system. Peptides. 2011; 32(11):2256-64. [DOI:10.1016/j.peptides.2011.04.010] [PMID]
- Peng D, Yang L, Liang XF, Chai F. Dietary zinc levels affect growth, appetite, and lipid metabolism of Chinese perch (Siniperca chuatsi). Fish Physiol Biochem. 2023; 49(5):1017-30. [DOI:10.1007/s10695-023-01238-w] [PMID]
- Hu X, Sheikhahmadi A, Li X, Wang Y, Jiao H, Lin H, et al. Effect of zinc on appetite regulatory peptides in the hypothalamus of salmonella-challenged broiler chickens. Biol Trace Elem Res. 2016; 172(1):228-33. [DOI:10.1007/s12011-015-0582-2] [PMID]
- Baltaci AK, Mogulkoc R. Leptin, N. Melatonin and zinc levels in experimental hypothyroidism and hyperthyroidism: the relation to zinc. Biochem Genet. 2017; 55(3):223-33. [DOI:10.1007/s10528-017-9791-z] [PMID]
- Daragó A, Sapota A, Matych J, Nasiadek M, Skrzypińska-Gawrysiak M, Kilanowicz A. The correlation between zinc and insulin-like growth factor 1 (IGF-1), its binding protein (IGFBP-3) and prostate-specific antigen (PSA) in prostate cancer. Clin Chem Lab Med. 2011; 49(10):1699-705. [DOI:10.1515/CCLM.2011.651] [PMID]
- Maggio M, De Vita F, Lauretani F, Buttò V, Bondi G, Cattabiani C, et al. IGF-1, the cross road of the nutritional, inflammatory and hormonal pathways to frailty. Nutrients. 2013; 5(10):4184-205. [DOI:10.3390/nu5104184] [PMID]
- Sanna A, Firinu D, Zavattari P, Valera P. Zinc status and autoimmunity: a systematic review and meta-analysis. Nutrients. 2018; 10(1):68. [DOI:10.3390/nu10010068] [PMID]
- Lin PH, Sermersheim M, Li H, Lee P, Steinberg SM, Ma J. Zinc in wound healing modulation. Nutrients. 2017; 10(1):16. [DOI:10.3390/nu10010016] [PMID]
- Park SG, Choi HN, Yang HR, Yim JE. Effects of zinc supplementation on catch-up growth in children with failure to thrive. Nutr Res Pr. 2017; 11(6):487-91. [DOI:10.4162/nrp.2017.11.6.487] [PMID]
- Monfared V, Salehian A, Nikniaz Z, Ebrahimpour-Koujan S, Faghfoori Z. The effect of zinc supplementation on anthropometric measurements in healthy children over two years: A systematic review and meta-analysis. BMC Pediatr. 2023; 23(1):414. [DOI:10.1186/s12887-023-04249-x] [PMID]
- Sugawara D, Makita E, Matsuura M, Ichihashi K. The association between serum zinc levels and anthropometric measurements and nutritional indicators in children with idiopathic short stature. Cureus. 2022. [DOI:10.7759/cureus.24906]
- International Zinc Nutrition Consultative Group (IZiNCG), Brown KH, Rivera JA, Bhutta Z, Gibson RS, et al. International zinc nutrition consultative group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr Bull. 2004; 25(1 Suppl 2):S99-203. [DOI:10.1177/156482650402500220]
Type of Study: Systematic Review |
Subject:
Pediatric Nephrology
Received: 2025/07/2 | Accepted: 2026/04/12 | Published: 2026/04/12
Received: 2025/07/2 | Accepted: 2026/04/12 | Published: 2026/04/12
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
