
Sun, Jun 14, 2026


Volume 14, Issue 1 (1-2026)
J. Pediatr. Rev 2026, 14(1): 73-80 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ashraf M, Ahmed P, Ahmed Peer S, Suhail Lone M, Nisar Andrabi A, Mushtaq S. Clinico-bacteriological Profile, Antibiotic Resistance Pattern, in Recurrent Urinary Tract Infections In Children. J. Pediatr. Rev 2026; 14 (1) :73-80
URL: http://jpr.mazums.ac.ir/article-1-773-en.html
URL: http://jpr.mazums.ac.ir/article-1-773-en.html
Mohd Ashraf *1 

 , Parvez Ahmed2 , Sameer Ahmed Peer2 , Mohd Suhail Lone3 , Ashiq Nisar Andrabi3 , Samiya Mushtaq2
, Parvez Ahmed2 , Sameer Ahmed Peer2 , Mohd Suhail Lone3 , Ashiq Nisar Andrabi3 , Samiya Mushtaq2
, Parvez Ahmed2 , Sameer Ahmed Peer2 , Mohd Suhail Lone3 , Ashiq Nisar Andrabi3 , Samiya Mushtaq2
1- Department of Pediatric Nephrology, Govt Medical College Srinagar, Kashmir India. , aashraf05@gmail.com
2- Department of Pediatrics, Govt Medical College Srinagar, Kashmir India.
3- Department of Pediatric Microbiology, Govt Medical College Srinagar, Kashmir India.
2- Department of Pediatrics, Govt Medical College Srinagar, Kashmir India.
3- Department of Pediatric Microbiology, Govt Medical College Srinagar, Kashmir India.
Full-Text [PDF 364 kb]
(188 Downloads)
| Abstract (HTML) (437 Views)
Full-Text: (111 Views)
Introduction
Recurrent urinary tract infection (UTI) in children is associated with considerable health risk and financial burden on the affected individuals and their families. Approximately 30% of children will experience at least one recurrence within 6–12 months, and 3–15% of children after the first UTI will show renal scarring [1-4]. Factors associated with recurrent UTI in infants <1 year include high-grade vesicoureteral reflux and delayed contrast clearance on Micturating cystourethrogram (MCU) [5, 6].
Besides these, other risk factors include various forms of obstructive uropathy, abnormal communications between the urinary and gastrointestinal systems, phimosis in male children, vulval synechiae in female children, bladder instability, and a history of antecedent infections [7-9].
Approximately 75% of pediatric UTIs are caused by Escherichia coli, which has demonstrated resistance to relapse [10, 11]. The presence of virulence factors, such as P fimbriae, the K1 capsular antigen, hemolytic factors, and cytotoxic necrotizing factors, helps E. coli colonize and cause UTIs. Other pathogens, such as Klebsiella, Proteus, Pseudomonas aeruginosa, Enterococcus, Staphylococcus, and Streptococcus, exhibit varied mechanisms for causing UTI [12, 13].
The use of antibiotics before the urine culture report is based on clinical findings and a positive urinalysis, to eradicate the microbe before it causes renal damage. However, while treating UTIs primarily with antimicrobials, antimicrobial resistance is emerging as a major challenge for physicians. This disturbing trend constitutes a major international public health threat where primary healthcare accounts for about 80% of all antibiotics prescribed [14, 15].
We aimed to study the clinical profile, common incriminating pathogens, risk factors, and antibiotic resistance in children with recurrent UTIs.
Materials and Methods
This prospective observational study was conducted over 18 months at the Department of Pediatrics and Pediatric Nephrology at the Government Children’s Hospital, Bemina, Srinagar—a tertiary care facility in Jammu and Kashmir, India. The study population comprised all children aged 1 month to 18 years who visited the pediatric nephrology and general pediatric outpatient departments with symptoms suggesting a UTI and who were subsequently evaluated for recurrent UTI, which was confirmed, and enrolled. All suspected patients between 1 month to 18 years, who met the inclusion criteria, were studied. Patients with HIV, congenital immune deficiencies, sickle cell disease, neurogenic bladder, paralytic syndromes, chronic renal disease, renal calculi, or central nervous system malformations were excluded. Informed consent from all participating patients or their parents/guardians was obtained, and comprehensive data were collected from each patient’s history, physical examination, and investigations, and recorded in a pre-designed proforma. During evaluation, clinical observations, comprehensive urinalysis (including isolation of specific pathogens and their antimicrobial sensitivity/resistance profiles), and ultrasound of the kidneys were performed in all. MCU and dimercaptosuccinic acid (DMSA)/diethylene triamine pentaacetic acid (DTPA)/uroflowmetry were performed as per protocol. Our additional evaluations included inquiries about urinary symptoms such as frequency, hesitancy, intermittent stream, weak stream, incontinence, nocturia, dysuria, holding manoeuvres, and incomplete emptying, which were also documented and analysed. In addition to assessment for urinary retention, post-micturition dribbling, suprapubic pain, bowel and bladder diary, along with psychological evaluation, were also carried out as needed.
Antibiogram disks for nitrofurantoin, meropenem, imipenem, ertapenem, co-amoxiclav, piperacillin-tazobactam, gentamicin, amikacin, colistin, cefepime, cefixime, cefotaxime, ceftazidime, ceftriaxone, linzolid, vancomycin, levofloxacin, ciprofloxacin, cotrimoxazole, fosfomycin, amoxicillin, ampicillin, amphotericin B, and rifampicin were studied and analysed. Data were collected using the structured pro forma and entered into a Microsoft Excel spreadsheet for subsequent statistical analysis. For continuous variables, Mean±SD was used; for non-normal distributions or those containing outliers, results were reported as percentages.
Results
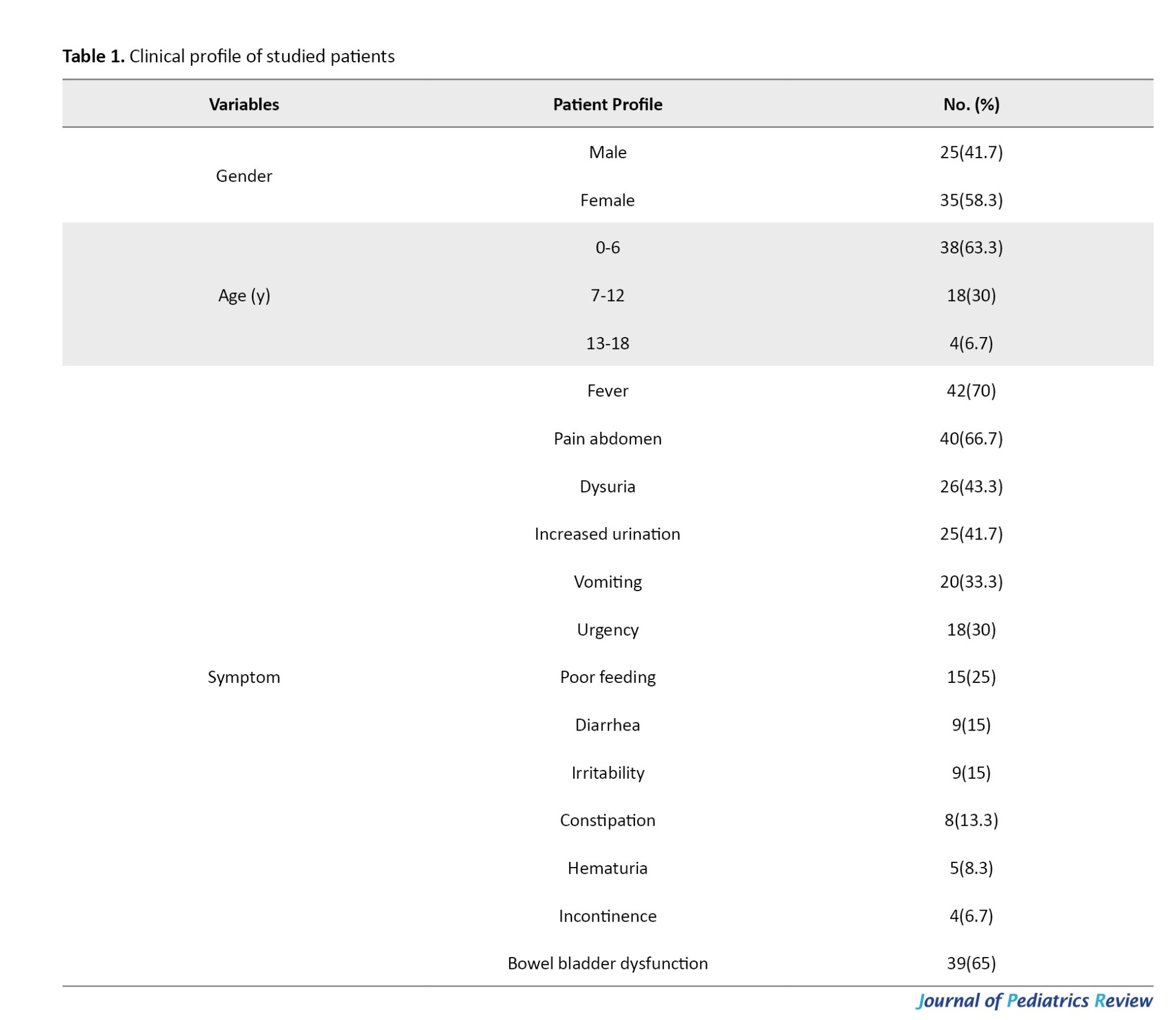
Of 60 children studied, 35(58.3%) were females, and 25(41.7%) were males; 38 patients (63.3%) were in the 1-5 years age group, with a mean age of presentation of 4.88±3.99 years. The most frequently reported clinical symptoms included fever in 42 patients (70%), followed by abdominal pain in 40(66.7%) and dysuria in 25 (41.7%). Other symptoms are shown in Table 1—bowel-bladder dysfunction, affecting 39 patients (65%) is a remarkable finding.
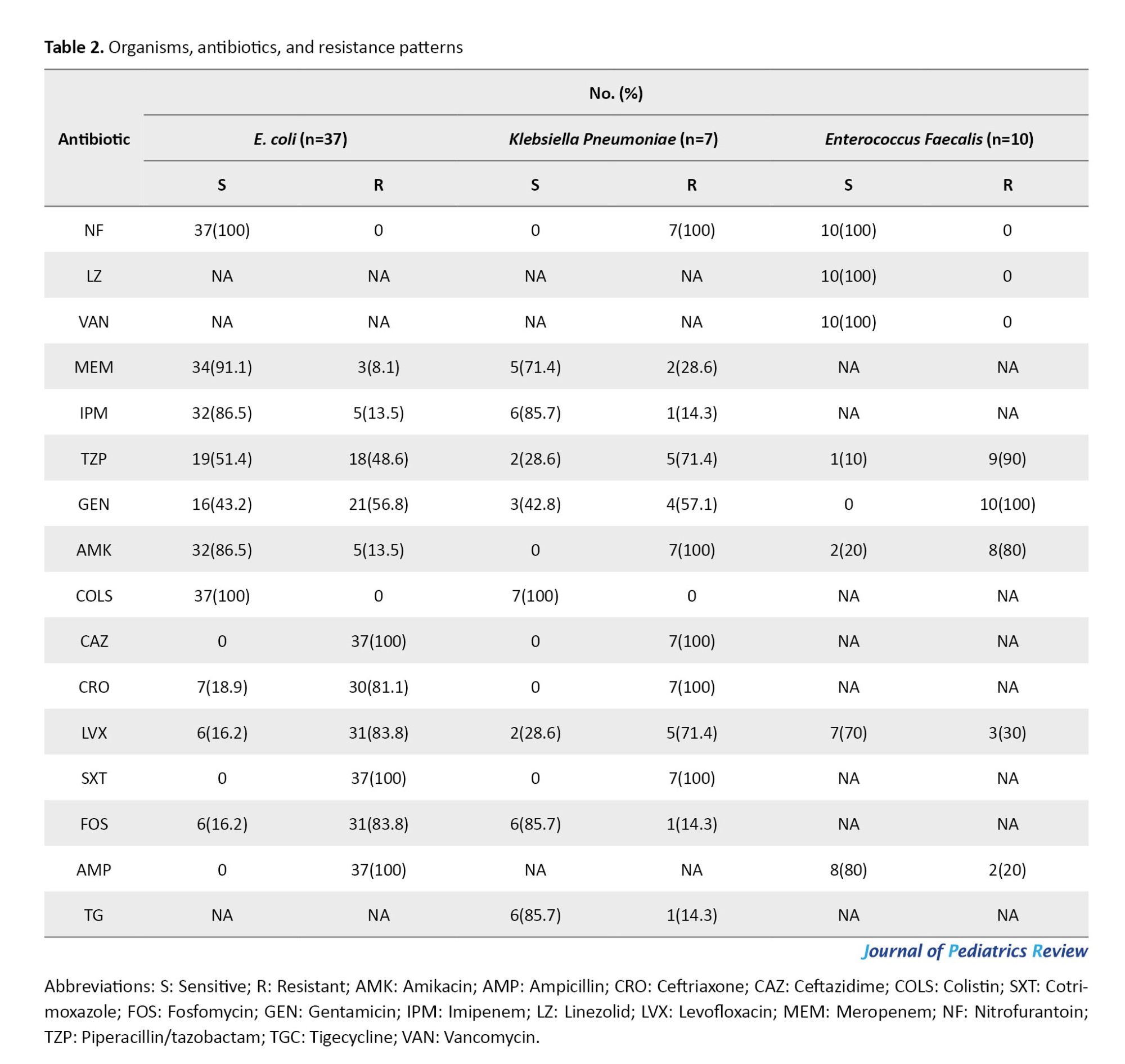
Antibiograms showing sensitivity and resistance are shown in Table 2.
Candida was isolated from one patient and was sensitive to amphotericin B. Mycobacterium tuberculosis was isolated from one patient and was sensitive to rifampicin. MCU was performed in 27 patients (45%), DMSA scans in 21(35%), and DTPA scans in 9(15%) patients. The majority of patients (n=48; 80%) were managed conservatively, while 12(20%) required surgical intervention; among those, ureterostomy was the most common procedure (33.3%), followed by fulguration. Nephrectomy was performed in one patient having chronic pyelonephritis with hypertension.
Discussion
Our study demonstrated that the most common age group was 1 month to 5 years (mean 4.88±3.99), which is consistent with the findings of Shaikh et al. [16]. A similar finding was observed by Kiros et al. [17] and Malla et al. [18], who noted that children under 10 years are more susceptible to recurrent UTIs. Regarding gender susceptibility, our finding of higher female prevalence (1.4:1) in recurrent UTIs is consistent with Malla et al. [18] and Gebremariam et al. [19], attributing this to females having a shorter and wider urethra, its proximity to the anus, and a warm, moist environment conducive to bacterial growth. However, some studies, such as those by Elale et al. [20], Kiros et al. [17], and Winberg et al. [21], reported a male predominance, potentially due to a larger proportion of uncircumcised males in their cohorts.
The most common presenting symptoms were fever (70%), followed by abdominal pain (66.7%), dysuria (43.3%), and increased urine frequency (41.7%). These clinical presentations are consistent with those reported by Schlager et al. [22].
Ultrasonography revealed various abnormalities in 43 patients (71.6%) which included hydronephrosis in 25(58%), unilateral multicystic dysplastic kidneys in 8(18.6%), prominent ureters 4(9.3%), pyelonephritis in 3(6,95), and horse shoe kidney, single kidney, unilateral double moiety in one each (2.3%), which is in line with the observations was made by Sinha et al. [23].
The present study showed vesicoureteral reflux (VUR) in 27 patients (45%), the commonest form of congenital anomalies of the kidney and urinary tract, similar to the observations of Sinha et al. [23] and Wils Gliam [24]. Among the 21 DMSA scans, 17 patients (81%) showed decreased uptake/renal scarring, while among the 9 DTPA scans, 4(44.4%) showed decreased estimated GFR unilaterally.
Our higher incidence of hydronephrosis compared to a previous study from the same centre by Ashraf et al. [25] might be attributed to our exclusive enrolment of recurrent UTI patients.
Besides VUR, the second most common association in recurrent UTI was bladder bowel dysfunction (BBD), observed in 39 patients (65%), which is higher than an earlier published study [26] but far lower than the study by Shaikh et al. [27].
Among gram-negative organisms, E. coli was the most common, accounting for 61.7% (37/60), followed by Enterococci at 16.7% (10/60) and Klebsiella at 11.7% (7/60). It is noteworthy that E. coli is consistently detected in recurrent UTIs, possibly due to its ability to evade host defences through evolving mechanisms. These findings are consistent with earlier studies [17-20, 28, 29], which reported E. coli as the predominant uropathogen in children.
E. coli isolates exhibited 100% sensitivity to nitrofurantoin and colistin. High sensitivity was also observed with meropenem (91.1%), imipenem (86.5%), amikacin (86.5%), and piperacillin-tazobactam (51.4%). However, E. coli showed 100% resistance to cefotaxime, ceftazidime, ampicillin, and cotrimoxazole. Increased resistance was also noted for ceftriaxone (81.1%), fosfomycin (83.8%), and levofloxacin (83.8%), as shown in Table 2, findings similar to those of the study conducted by Younis et al. [30]. For Klebsiella species, 100% sensitivity was observed with colistin, and 85.7% sensitivity with fosfomycin, tigecycline, and imipenem. Conversely, Klebsiella exhibited 100% resistance to nitrofurantoin, ceftriaxone, ceftazidime, and cotrimoxazole. Other notable resistances included tazobactam (71.4%) and levofloxacin (71.4%). These findings generally align with those of Maraki et al. [31].
Among gram-positive pathogens, Enterococcus demonstrated 100% sensitivity to linezolid, nitrofurantoin, and vancomycin. They showed 80% sensitivity to ampicillin and 70% to levofloxacin. However, Enterococcus exhibited 100% resistance to gentamicin, 90% resistance to piperacillin-tazobactam, and 80% resistance to amikacin, a pattern consistent with results from Elale et al. [20], who also reported high resistance to tetracycline and erythromycin but no resistance to nitrofurantoin in Enterococcus species.
Conclusion
Recurrent UTIs in children are not uncommon and are often linked to underlying congenital anomalies, such as vesicoureteral reflux, pelvi-ureteric junction obstruction, and posterior urethral valve, as well as clinical conditions like bowel-bladder dysfunction. Among the causative organisms, E. coli and Enterococcus were identified as the most frequent pathogens. These isolates demonstrated high susceptibility to certain antibacterial agents, while showing resistance to many others, underscoring the challenge of effective treatment. These findings emphasize the importance of early identification and management of congenital anomalies of the kidney and urinary tract., addressing bowel–bladder dysfunction as a contributing factor; while implementing targeted antibiotic stewardship to minimize resistance and prevent recurrence.
Study limitations
The main limitations of this study are the small sample size (60 children) and its conduct at a single tertiary care center. These factors restrict the generalizability of the antibiotic resistance findings to other healthcare settings (such as primary care centers) and different geographical regions. The observational, non-comparative nature of the study prevents us from accurately determining cause-and-effect relationships and quantifying the independent effects of each risk factor. As we excluded patients with immunodeficiencies, neurogenic bladder, and chronic kidney disease to homogenize the study group, the results do not apply to the entire spectrum of children with recurrent UTI (who often have these comorbidities). The highest frequency of patients was in the age group of 1 month to 5 years, while risk factors such as BBD are more common in children older than 4-5 years, and remained unresolved, being this a descriptive study.
Study recommendations
Given the above limitations, there is a clear need for larger multicenter studies to enhance the generalizability of findings across diverse populations and healthcare settings. In addition molecular analysis of bacterial strains to better understand resistance mechanisms and epidemiological patterns along with interventional studies on bowel–bladder dysfunction (BBD) management, as this remains an under-resolved risk factor in recurrent pediatric UTIs.
Ethical Considerations
Compliance with ethical guidelines
Study was conducted after obtained ethical clearance from the Institution Ethical Committee, Government Medical College Srinagar, Kashmir India. Due informed consents were taken from parents/legal guardians/assent from children whichever was applicable.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization and study design: Parvez Ahmed and Mohd Ashraf; Methodology and data analysis: Mohd Ashraf, Mohd Suhail Lone, Sameer Ahmed Peer; Writing: Mohd Ashraf, Ashiq Nisar Andrabi, and Samiya Mushtaq.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors acknowledge the kind help of Vaseem Yousuf, Plant Pathology SKUAST-Kashmir while preparing this draft.
References
Recurrent urinary tract infection (UTI) in children is associated with considerable health risk and financial burden on the affected individuals and their families. Approximately 30% of children will experience at least one recurrence within 6–12 months, and 3–15% of children after the first UTI will show renal scarring [1-4]. Factors associated with recurrent UTI in infants <1 year include high-grade vesicoureteral reflux and delayed contrast clearance on Micturating cystourethrogram (MCU) [5, 6].
Besides these, other risk factors include various forms of obstructive uropathy, abnormal communications between the urinary and gastrointestinal systems, phimosis in male children, vulval synechiae in female children, bladder instability, and a history of antecedent infections [7-9].
Approximately 75% of pediatric UTIs are caused by Escherichia coli, which has demonstrated resistance to relapse [10, 11]. The presence of virulence factors, such as P fimbriae, the K1 capsular antigen, hemolytic factors, and cytotoxic necrotizing factors, helps E. coli colonize and cause UTIs. Other pathogens, such as Klebsiella, Proteus, Pseudomonas aeruginosa, Enterococcus, Staphylococcus, and Streptococcus, exhibit varied mechanisms for causing UTI [12, 13].
The use of antibiotics before the urine culture report is based on clinical findings and a positive urinalysis, to eradicate the microbe before it causes renal damage. However, while treating UTIs primarily with antimicrobials, antimicrobial resistance is emerging as a major challenge for physicians. This disturbing trend constitutes a major international public health threat where primary healthcare accounts for about 80% of all antibiotics prescribed [14, 15].
We aimed to study the clinical profile, common incriminating pathogens, risk factors, and antibiotic resistance in children with recurrent UTIs.
Materials and Methods
This prospective observational study was conducted over 18 months at the Department of Pediatrics and Pediatric Nephrology at the Government Children’s Hospital, Bemina, Srinagar—a tertiary care facility in Jammu and Kashmir, India. The study population comprised all children aged 1 month to 18 years who visited the pediatric nephrology and general pediatric outpatient departments with symptoms suggesting a UTI and who were subsequently evaluated for recurrent UTI, which was confirmed, and enrolled. All suspected patients between 1 month to 18 years, who met the inclusion criteria, were studied. Patients with HIV, congenital immune deficiencies, sickle cell disease, neurogenic bladder, paralytic syndromes, chronic renal disease, renal calculi, or central nervous system malformations were excluded. Informed consent from all participating patients or their parents/guardians was obtained, and comprehensive data were collected from each patient’s history, physical examination, and investigations, and recorded in a pre-designed proforma. During evaluation, clinical observations, comprehensive urinalysis (including isolation of specific pathogens and their antimicrobial sensitivity/resistance profiles), and ultrasound of the kidneys were performed in all. MCU and dimercaptosuccinic acid (DMSA)/diethylene triamine pentaacetic acid (DTPA)/uroflowmetry were performed as per protocol. Our additional evaluations included inquiries about urinary symptoms such as frequency, hesitancy, intermittent stream, weak stream, incontinence, nocturia, dysuria, holding manoeuvres, and incomplete emptying, which were also documented and analysed. In addition to assessment for urinary retention, post-micturition dribbling, suprapubic pain, bowel and bladder diary, along with psychological evaluation, were also carried out as needed.
Antibiogram disks for nitrofurantoin, meropenem, imipenem, ertapenem, co-amoxiclav, piperacillin-tazobactam, gentamicin, amikacin, colistin, cefepime, cefixime, cefotaxime, ceftazidime, ceftriaxone, linzolid, vancomycin, levofloxacin, ciprofloxacin, cotrimoxazole, fosfomycin, amoxicillin, ampicillin, amphotericin B, and rifampicin were studied and analysed. Data were collected using the structured pro forma and entered into a Microsoft Excel spreadsheet for subsequent statistical analysis. For continuous variables, Mean±SD was used; for non-normal distributions or those containing outliers, results were reported as percentages.
Results
Of 60 children studied, 35(58.3%) were females, and 25(41.7%) were males; 38 patients (63.3%) were in the 1-5 years age group, with a mean age of presentation of 4.88±3.99 years. The most frequently reported clinical symptoms included fever in 42 patients (70%), followed by abdominal pain in 40(66.7%) and dysuria in 25 (41.7%). Other symptoms are shown in Table 1—bowel-bladder dysfunction, affecting 39 patients (65%) is a remarkable finding.
Antibiograms showing sensitivity and resistance are shown in Table 2.
Candida was isolated from one patient and was sensitive to amphotericin B. Mycobacterium tuberculosis was isolated from one patient and was sensitive to rifampicin. MCU was performed in 27 patients (45%), DMSA scans in 21(35%), and DTPA scans in 9(15%) patients. The majority of patients (n=48; 80%) were managed conservatively, while 12(20%) required surgical intervention; among those, ureterostomy was the most common procedure (33.3%), followed by fulguration. Nephrectomy was performed in one patient having chronic pyelonephritis with hypertension.
Discussion
Our study demonstrated that the most common age group was 1 month to 5 years (mean 4.88±3.99), which is consistent with the findings of Shaikh et al. [16]. A similar finding was observed by Kiros et al. [17] and Malla et al. [18], who noted that children under 10 years are more susceptible to recurrent UTIs. Regarding gender susceptibility, our finding of higher female prevalence (1.4:1) in recurrent UTIs is consistent with Malla et al. [18] and Gebremariam et al. [19], attributing this to females having a shorter and wider urethra, its proximity to the anus, and a warm, moist environment conducive to bacterial growth. However, some studies, such as those by Elale et al. [20], Kiros et al. [17], and Winberg et al. [21], reported a male predominance, potentially due to a larger proportion of uncircumcised males in their cohorts.
The most common presenting symptoms were fever (70%), followed by abdominal pain (66.7%), dysuria (43.3%), and increased urine frequency (41.7%). These clinical presentations are consistent with those reported by Schlager et al. [22].
Ultrasonography revealed various abnormalities in 43 patients (71.6%) which included hydronephrosis in 25(58%), unilateral multicystic dysplastic kidneys in 8(18.6%), prominent ureters 4(9.3%), pyelonephritis in 3(6,95), and horse shoe kidney, single kidney, unilateral double moiety in one each (2.3%), which is in line with the observations was made by Sinha et al. [23].
The present study showed vesicoureteral reflux (VUR) in 27 patients (45%), the commonest form of congenital anomalies of the kidney and urinary tract, similar to the observations of Sinha et al. [23] and Wils Gliam [24]. Among the 21 DMSA scans, 17 patients (81%) showed decreased uptake/renal scarring, while among the 9 DTPA scans, 4(44.4%) showed decreased estimated GFR unilaterally.
Our higher incidence of hydronephrosis compared to a previous study from the same centre by Ashraf et al. [25] might be attributed to our exclusive enrolment of recurrent UTI patients.
Besides VUR, the second most common association in recurrent UTI was bladder bowel dysfunction (BBD), observed in 39 patients (65%), which is higher than an earlier published study [26] but far lower than the study by Shaikh et al. [27].
Among gram-negative organisms, E. coli was the most common, accounting for 61.7% (37/60), followed by Enterococci at 16.7% (10/60) and Klebsiella at 11.7% (7/60). It is noteworthy that E. coli is consistently detected in recurrent UTIs, possibly due to its ability to evade host defences through evolving mechanisms. These findings are consistent with earlier studies [17-20, 28, 29], which reported E. coli as the predominant uropathogen in children.
E. coli isolates exhibited 100% sensitivity to nitrofurantoin and colistin. High sensitivity was also observed with meropenem (91.1%), imipenem (86.5%), amikacin (86.5%), and piperacillin-tazobactam (51.4%). However, E. coli showed 100% resistance to cefotaxime, ceftazidime, ampicillin, and cotrimoxazole. Increased resistance was also noted for ceftriaxone (81.1%), fosfomycin (83.8%), and levofloxacin (83.8%), as shown in Table 2, findings similar to those of the study conducted by Younis et al. [30]. For Klebsiella species, 100% sensitivity was observed with colistin, and 85.7% sensitivity with fosfomycin, tigecycline, and imipenem. Conversely, Klebsiella exhibited 100% resistance to nitrofurantoin, ceftriaxone, ceftazidime, and cotrimoxazole. Other notable resistances included tazobactam (71.4%) and levofloxacin (71.4%). These findings generally align with those of Maraki et al. [31].
Among gram-positive pathogens, Enterococcus demonstrated 100% sensitivity to linezolid, nitrofurantoin, and vancomycin. They showed 80% sensitivity to ampicillin and 70% to levofloxacin. However, Enterococcus exhibited 100% resistance to gentamicin, 90% resistance to piperacillin-tazobactam, and 80% resistance to amikacin, a pattern consistent with results from Elale et al. [20], who also reported high resistance to tetracycline and erythromycin but no resistance to nitrofurantoin in Enterococcus species.
Conclusion
Recurrent UTIs in children are not uncommon and are often linked to underlying congenital anomalies, such as vesicoureteral reflux, pelvi-ureteric junction obstruction, and posterior urethral valve, as well as clinical conditions like bowel-bladder dysfunction. Among the causative organisms, E. coli and Enterococcus were identified as the most frequent pathogens. These isolates demonstrated high susceptibility to certain antibacterial agents, while showing resistance to many others, underscoring the challenge of effective treatment. These findings emphasize the importance of early identification and management of congenital anomalies of the kidney and urinary tract., addressing bowel–bladder dysfunction as a contributing factor; while implementing targeted antibiotic stewardship to minimize resistance and prevent recurrence.
Study limitations
The main limitations of this study are the small sample size (60 children) and its conduct at a single tertiary care center. These factors restrict the generalizability of the antibiotic resistance findings to other healthcare settings (such as primary care centers) and different geographical regions. The observational, non-comparative nature of the study prevents us from accurately determining cause-and-effect relationships and quantifying the independent effects of each risk factor. As we excluded patients with immunodeficiencies, neurogenic bladder, and chronic kidney disease to homogenize the study group, the results do not apply to the entire spectrum of children with recurrent UTI (who often have these comorbidities). The highest frequency of patients was in the age group of 1 month to 5 years, while risk factors such as BBD are more common in children older than 4-5 years, and remained unresolved, being this a descriptive study.
Study recommendations
Given the above limitations, there is a clear need for larger multicenter studies to enhance the generalizability of findings across diverse populations and healthcare settings. In addition molecular analysis of bacterial strains to better understand resistance mechanisms and epidemiological patterns along with interventional studies on bowel–bladder dysfunction (BBD) management, as this remains an under-resolved risk factor in recurrent pediatric UTIs.
Ethical Considerations
Compliance with ethical guidelines
Study was conducted after obtained ethical clearance from the Institution Ethical Committee, Government Medical College Srinagar, Kashmir India. Due informed consents were taken from parents/legal guardians/assent from children whichever was applicable.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization and study design: Parvez Ahmed and Mohd Ashraf; Methodology and data analysis: Mohd Ashraf, Mohd Suhail Lone, Sameer Ahmed Peer; Writing: Mohd Ashraf, Ashiq Nisar Andrabi, and Samiya Mushtaq.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors acknowledge the kind help of Vaseem Yousuf, Plant Pathology SKUAST-Kashmir while preparing this draft.
References
- Williams G, Craig JC. Long-term antibiotics for preventing recurrent urinary tract infection in children. Cochrane Database Syst Rev. 2019; 4:CD001534. [DOI:10.1002/14651858.CD001534.pub4]
- Stein R, Dogan HS, Hoebeke P, Kočvara R, Nijman RJ, Radmayr C, et al. Urinary tract infections in children: EAU/ESPU guidelines. Eur Urol. 2015; 67(3):546-58. [DOI:10.1016/j.eururo.2014.11.007] [PMID]
- White B. Diagnosis and treatment of urinary tract infections in children. Am Fam Physician. 2011; 83(4):409-15. [PMID]
- Mattoo TK, Shaikh N, Nelson CP. Contemporary Management of Urinary Tract Infection in Children. Pediatrics. 2021; 147(2):e2020012138. [DOI:10.1542/peds.2020-012138] [PMID]
- Shiraishi K, Yoshino K, Watanabe M, Matsuyama H, Tanikaze S. Risk factors for breakthrough infection in children with primary vesicoureteral reflux. J Urol. 2010; 183(4):1527-31.[DOI:10.1016/j.juro.2009.12.039] [PMID]
- Jang HC, Park YJ, Park JS. Predicting factors of breakthrough infection in children with primary vesicoureteral reflux. Yonsei Med J. 2012; 53(4):748-52. [PMID]
- Hellerstein S. Recurrent urinary tract infections in children. Pediatr Infect Dis. 1982; 1(4):271-81.[DOI:10.1097/00006454-198207000-00018] [PMID]
- Rushton HG. Urinary tract infections in children. Epidemiology, evaluation and management. Pediatr Clin North Am. 1997; 44(5):1133-69. [DOI:10.1016/S0031-3955(05)70551-4] [PMID]
- Beachey EH. Bacterial adherence: Adhesin-receptor interactions mediating the attachment of bacteria to mucosal surface. J Infect Dis. 1981; 143(3):325-45. [DOI:10.1093/infdis/143.3.325] [PMID]
- Roberts JA, Marklund BI, Ilver D, Haslam D, Kaack MB, Baskin G, et al. The Gal(alpha 1-4)Galspecific tip adhesin of Escherichia coli P- fimbriae is needed for pyelonephritis to occur in the normal urinary tract. Proc Natl Acad Sci USA. 1994; 91(25):11889-93. [DOI:10.1073/pnas.91.25.11889] [PMID]
- Schlager TA. Urinary tract infections in children younger than 5 years of age: Epidemiology, diagnosis, treatment, outcomes and prevention. Paediatr Drugs. 2001; 3(3):219-27. [DOI:10.2165/00128072-200103030-00004] [PMID]
- Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015; 13(5):269-84. [DOI:10.1038/nrmicro3432] [PMID]
- Bashir S, Haque A, Sarwar Y, Ali A, Anwar MI. Virulence profile of different phylogenetic groups of locally isolated community acquired uropathogenic E. coli from Faisalabad region of Pakistan. Ann Clin Microbiol Antimicrob. 2012; 11:23. [DOI:10.1186/1476-0711-11-23] [PMID]
- Goossens, H.; Ferech, M.; Vander Stichele, R. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet. 2005, 365(9459):579-87. [DOI: 10.1016/S0140-6736(05)17907-0] [PMID]
- Delbet J.D, Lorrot M, Ulinski T. An update on new antibiotic prophylaxis and treatment for urinary tract infections in children. Expert Opin Pharmacother. 2017; 18(15):1619-25. [DOI:10.1080/14656566.2017.1383383] [PMID]
- Shaikh N, Morone NE, Bost JE, Farrell MH. Prevalence of urinary tract infection in childhood: A meta-analysis. Pediatr Infect Dis J. 2008; 27(4):302-8. [DOI:10.1097/INF.0b013e31815e4122] [PMID]
- Kiros T, Zeleke M, Eyayu T, Workineh L, Damtie S, Andualem T, et al. Bacterial Etiology of urinary tract infection and antibiogram profile in children attending debre tabor comprehensive specialized hospital, Northwest Ethiopia. Interdiscip Perspect Infect Dis. 2023; 2023:1035113.[DOI:10.1155/2023/1035113] [PMID]
- Malla KK, Sharma MS, Malla T, Thapalial A. Clinical profile bacterial isolates and antibiotic susceptibility pattern in UTI in children-hospital based study. J Nepal Paeditr Soc. 2008; 28(2):52-61. [DOI:10.3126/jnps.v28i2.1388]
- Gebremariam G, Legese H, Woldu Y, Araya T, Hagos K, GebreyesusWasihun A. Bacteriological profile, risk factors and antimicrobial susceptibility patterns of symptomatic urinary tract infection among students of Mekelle University, northern Ethiopia. BMC Infect Dis. 2019; 19(1):950. [DOI:10.1186/s12879-019-4610-2] [PMID]
- Elale AK, Manilal A, Tadesse D, Seid M, Dubale A. Magnitude and associated factors of bacterial urinary tract infections among paediatric patients in Arba Minch, southern Ethiopia. New Microbes New Infect. 2023; 51:101083. [DOI:10.1016/j.nmni.2023.101083] [PMID]
- Winberg J, Bergström T, Jacobsson B. Morbidity, age and sex distribution, recurrences and renal scarring in symptomatic urinary tract infection in childhood. Kidney Int Suppl. 1975; 4:S101-6. [PMID]
- Schlager TA. Urinary tract infections in infants and children. Infect Dis Clin North Am. 2003; 17(2):353-65, ix. [DOI:10.1016/S0891-5520(03)00009-6] [PMID]
- Sinha R, Mukherjee D, Sengupta J, saha S, Banerjee S. Yield of imaging performed as per Indian Society of Pediatric Nephrology guidelines in children with urinary tract infection. Indian Pediatr. 2017; 54(9):749-51. [DOI:10.1007/s13312-017-1168-1] [PMID]
- Wils Gliam, Fletcher JT, Alexander SI, Craig JC. Vesicoureteral reflux. J Am Soc Nephrol. 2008; 19(5):847-62. [DOI:10.1681/ASN.2007020245] [PMID]
- Ashraf M, Kumar V, Bano RA, Wani KA, Ahmed J, Ahmed K. Spectrum of Renal and Urinary Tract Diseases in Kashmiri Children. J Clin Diagn Res. 2016; 10(6):SM01-2. [DOI:10.7860/JCDR/2016/20222.7999] [PMID]
- Shaikh N, Hoberman A, Wise B, Kurs-Lasky M, Kearney D, Naylor S, et al. Dysfunctional elimination syndrome: is it related to urinary tract infection or vesicoureteral reflux diagnosed early in life? Pediatrics. 2003; 112(5):1134-7.[DOI:10.1542/peds.112.5.1134] [PMID]
- Shaikh N, Hoberman A, Keren R, Gotman N, Docimo SG, Mathews R, et al Recurrent Urinary Tract Infections in Children With Bladder and Bowel Dysfunction. Pediatrics. 2016; 137(1):e20152982. [DOI:10.1542/peds.2015-2982] [PMID]
- Kalita D, Fahima I, Mahibur R, Clinical profile and antibiotic sensitivity pattern of community acquired urinary tract infections in children attending a tertiary care hospital in Assam, India. J Clin Diagnos Res. 2023; 17: 17(3): SC34-37.[DOI:10.7860/JCDR/2023/62444.17654]
- Pooja P, Garala RN. Bacteriological profile and antibiotic susceptibility pattern (antibiogram) of urinary tract infections in paediatric patients. J Res Med Den Sci. 2014; 2(1):20-3. [Link]
- Younis N, Quol K, Al-Momani T, Al-Awaisheh F, Al-Kayed D. Antibiotic resistance in children with recurrent or complicated urinary tract infection. JNMA J Nepal Med Assoc. 2009; 48(173):14-9. [PMID]
- Maraki S, Mantadakis E, Michailidis L, Samonis G. Changing antibiotic susceptibilities of community-acquired uropathogens in Greece, 2005-2010. J Microbiol Immunol Infect. 2013; 46(3):202-9. [DOI:10.1016/j.jmii.2012.05.012] [PMID]
Type of Study: Original Article |
Subject:
Pediatrics
Received: 2025/07/26 | Accepted: 2025/11/23 | Published: 2026/01/1
Received: 2025/07/26 | Accepted: 2025/11/23 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
