
Tue, Jun 9, 2026


Volume 14, Issue 1 (1-2026)
J. Pediatr. Rev 2026, 14(1): 53-62 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rostami Maskopaii S, Farnia S, Abaskhanian A, Kalantary A. Exploring the Conditions of Lost Individuals in Need of Care: A Review of Caregivers of Children With Special Needs (Shadow Nurses). J. Pediatr. Rev 2026; 14 (1) :53-62
URL: http://jpr.mazums.ac.ir/article-1-784-en.html
URL: http://jpr.mazums.ac.ir/article-1-784-en.html



1- Mazandaran University of Medical Sciences, Sari, Iran. , somayehrostami4@yahoo.com
2- Department of Psychiatry, Psychiatry and Behavioral Sciences Research Center, School of Medicine, Addiction Institute, Zare Hospital, Mazandaran University of Medical Sciences, Sari, Iran.
3- Pediatric Infectious Diseases Research Center, Communicable Diseases Institute, Mazandaran University of Medical Sciences, Sari, Iran.
4- Ministry of Sports and Youth Affairs, Tehran, Iran.
2- Department of Psychiatry, Psychiatry and Behavioral Sciences Research Center, School of Medicine, Addiction Institute, Zare Hospital, Mazandaran University of Medical Sciences, Sari, Iran.
3- Pediatric Infectious Diseases Research Center, Communicable Diseases Institute, Mazandaran University of Medical Sciences, Sari, Iran.
4- Ministry of Sports and Youth Affairs, Tehran, Iran.
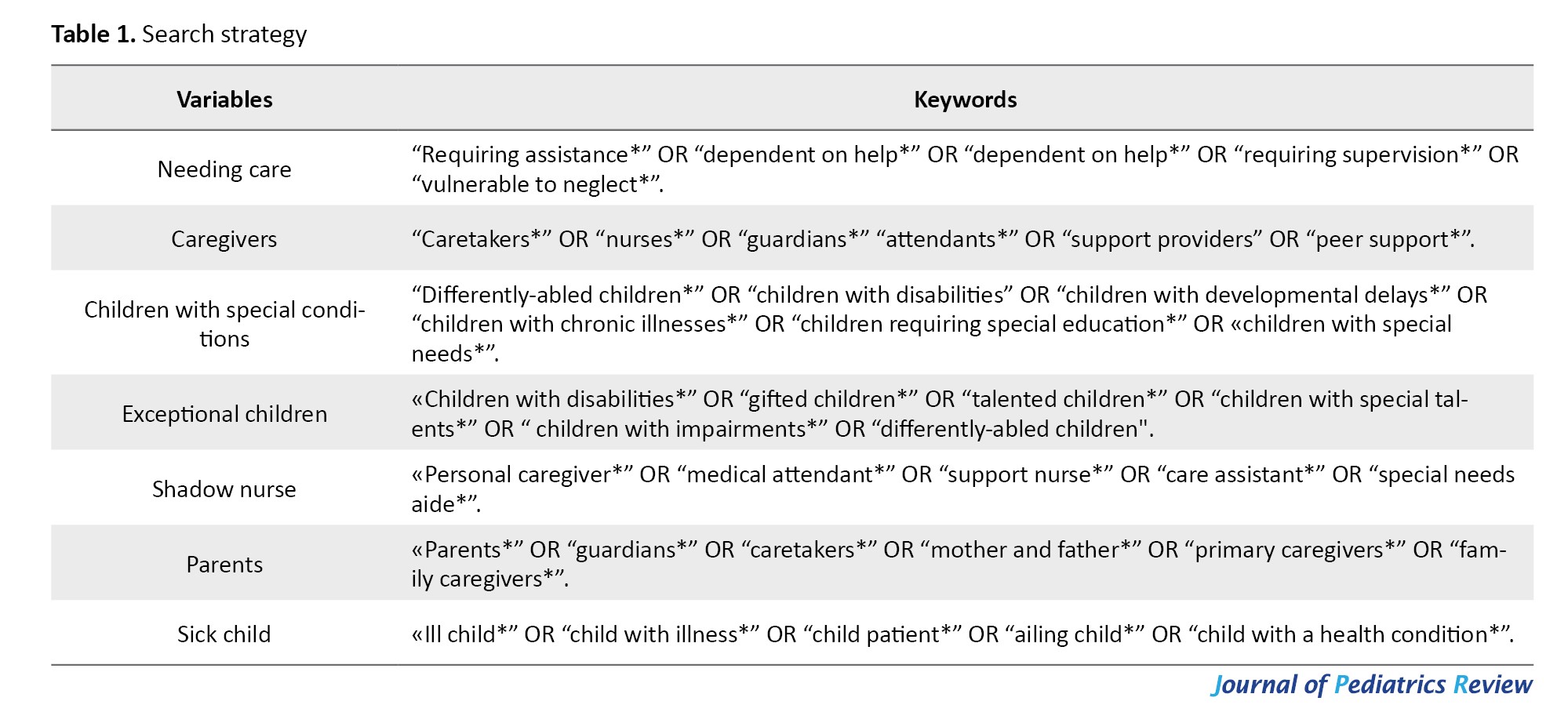
Keywords: Needing care, Caregivers, Children with special conditions, Exceptional children, Shadow nurse, Parents, Sick child
Full-Text [PDF 544 kb]
(356 Downloads)
| Abstract (HTML) (651 Views)
Full-Text: (110 Views)
Introduction
Achild’s illness or disability affects the whole family. A significant number of children around the world has some disability. According to the World Health Organization (WHO) and UNICEF, this figure includes more than 240 million children in the world, for every 10 children there is a disabled child (1/10). Since there are no exact statistics on the number of families with disabled children, given the number of disabled children (more than 240 million disabled children), it can be estimated that millions of families in the world have disabled children. It is noteworthy that 75% of children with disabilities live in developing countries, but in the United States, approximately one-fifth of families are responsible for caring for a child with a chronic health condition [1]. In any case, this impressive figure shows the urgent need to support these children. It shows the family as the most important and closest caregivers for children. Children inevitably experience illness during their early years, with conditions ranging from acute issues such as the common cold to chronic diseases like cystic fibrosis or disabilities [2]. Still, the hospitalization of a child is a source of risk, stress, and strain for parents [3-8]. Hospitalization represents a critical experience for ill children, significantly disrupting the equilibrium between the children and their families. Admission to the hospital exposes them to challenging and often distressing procedures that induce both physical and psychological discomfort [9].
A child’s illness generates substantial stress and anxiety across the entire family. Beyond impacting the child directly, it also influences parents, siblings, and other relatives [3-8]. Some illnesses improve over time, and the child regains his health, but some illnesses are chronic, and disabilities remain with the person for the rest of his life, which imposes a lot of pressure on the child and the family. It creates a psychological burden, a care burden, an economic burden, a social burden, etc., for all family members and leads to physical, mental, and psychological tensions.
Not only does the sick child need support and care, but the child’s parents, caregivers, and child care providers do as well. Throughout a child’s hospitalization, care is provided not only to the child but also to their parents. Parents are considered vital members of the care team and are encouraged to remain with their child in the hospital ward. Their presence contributes to the child’s safety and reduces anxiety. Additionally, nurses support the child’s adjustment to the new environment by fostering interactions and collaboration between the child and the parent [10]. While parents or caregivers often embrace their role willingly, the extra demands and pressures of caregiving—frequently coupled with insufficient skills, resources, and support—expose them and their families to heightened risks of stress, diminished functioning, declining wellbeing, and a lower quality of life. In fact, the quality of individual, family, professional, and social life of family members will change due to the child’s illness [11]. However, improved emotional and psychological wellbeing among parents correlates with enhanced mental and physical health outcomes in their children [12-14]. Therefore, implementing strategies to build parental capacity and improve their wellbeing and quality of life is vital for comprehensively supporting the growth of children with disabilities [15]. To enhance children’s health outcomes, the caregiving needs of their parents must be prioritized [16].
Studies indicate that caregiving frequently imposes substantial stress, creating social, emotional, behavioral, and financial burdens on caregivers, which heightens their vulnerability to mental health issues like depression and anxiety, as well as physical ailments. Caregivers are just as susceptible to psychological stress as patients [16-20]. So, decisions must be made to prevent potential harm to the child and the child’s caregivers and parents, to mitigate hospitalization’s adverse effects on children. Parents should participate in all nursing interventions, and there should be effective communication among children, parents, and nurses. Providing clear medical information about the child’s condition addresses questions and alleviates parental anxiety [21].
Family-centered support for sick children is one of the basic and effective strategies for improving the child’s and the family’s physical, psychological, and social status. Experience has shown that when the families of sick children, especially parents, receive the necessary support, not only will the child have a greater chance of achieving treatment goals and personal growth, but family and marital relationships will also improve, and greater resilience to the stresses, pressures, and dangers of the disease will be achieved. Different support areas include psychological support (receiving counseling and education to cope with emotional pressures and accept new living conditions), financial support (providing medical, pharmaceutical, and care costs that are usually beyond the family’s ability), social support (creating connections with associations, support groups, and benefiting from the experiences of similar families to reduce isolation and increase hope), practical and executive support (facilitating access to medical services, rehabilitation, transportation, and special care), and informational support (access to educational resources and accurate information about the disease, care methods, and better management of the child’s condition).
Family-centered practice, the primary framework for supporting children with developmental delays and disabilities, addresses stressors while leveraging family strengths to enhance overall family functioning [22]. In this regard, family-centered support is a comprehensive approach that places not only the child, but also the entire family on the path to empowerment and coping with the crisis, and prevents negative psychological and social consequences. Creating such support can maintain the mental health of children, parents, and other family members and enhance their level of cooperation and adaptation.
The health and quality of life of patients are as important as those of their parents, companions, and caregivers. In this article, caregivers include parents, siblings, grandparents, educators, and child care providers, although everyone in direct contact with the child, in the family and social environment, is part of the chain of caregivers for children with special needs. The present study points to those who are missing and need support and care—the forgotten who have a very important mission in caring for sick and disabled children. Accordingly, the purpose of the present study is to investigate the circumstances of missing persons in need of care, with a focus on caregivers of children with special needs. In this study, shadow nurses are referred to as parents, caregivers, and nurses of sick children. To give power to sick children, their parents must also be empowered, and their quality of life must be improved. They need more support and care than parents of normal or healthy children. This study emphasizes the need for tailored support systems—such as education, counseling, and community resources—to reinforce caregiver resilience and improve coping, thereby enhancing the quality of life for children and their families.
Materials and Methods
This systematic review adhered to PRISMA guidelines and searched databases including PubMed, Scopus, Web of Science, UpToDate, Google Scholar, and Embase. Keywords from Table 1 were combined using Boolean operators to identify relevant Persian and English articles published between 2011 and 2025.
Caregivers of children with special needs include children with acute or chronic disabilities, physical, mental, sensory, or developmental disabilities, or specific and chronic illnesses (CI) who require specialized and daily care. Caregivers must be adults (usually over 18). They may include parents, family members, day care nurses, social workers, and other formal or informal caregivers responsible for the child’s ongoing daily care.
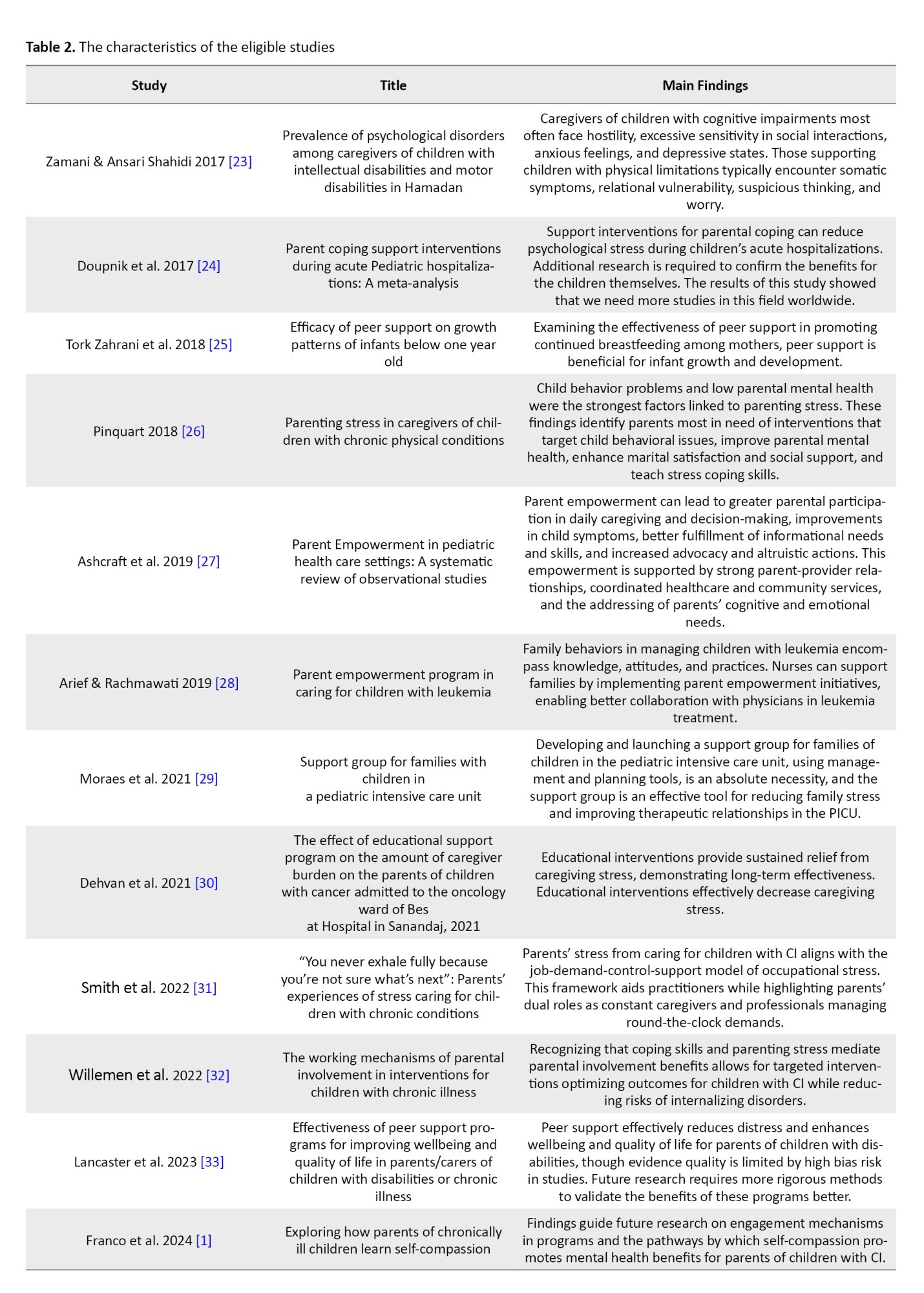
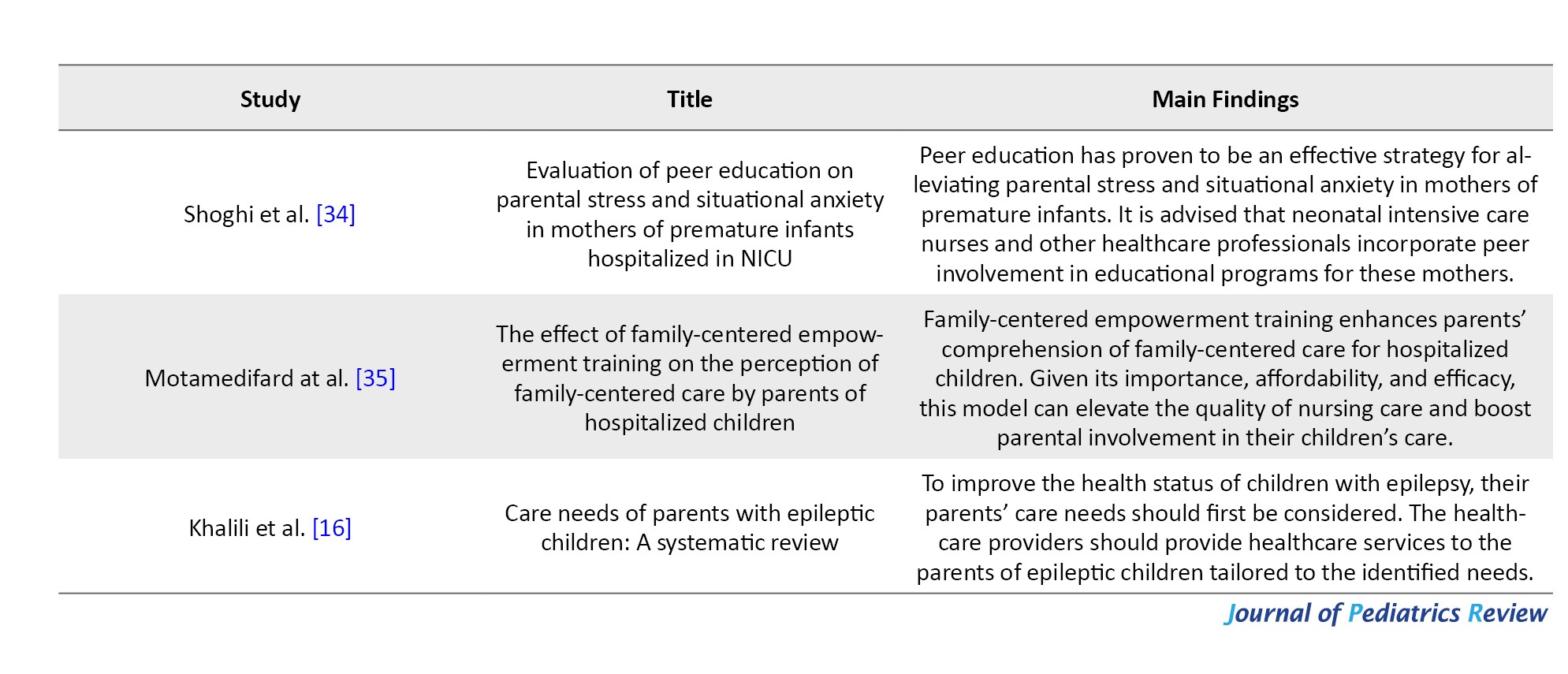
The children in care must have special needs, including requiring daily care, chronic or long-term disabilities, or specific medical conditions (children with disabilities, gifted children, talented children, children with special talents, children with impairments, differently-abled children). First, researcher one screened the titles and abstracts of all retrieved articles. Selected relevant articles then underwent full-text evaluation. In the second stage, the researcher number two conducted the content analysis of the selected articles. After extracting the eligible articles, the general data, study characteristics, and results were summarized in Table 2.
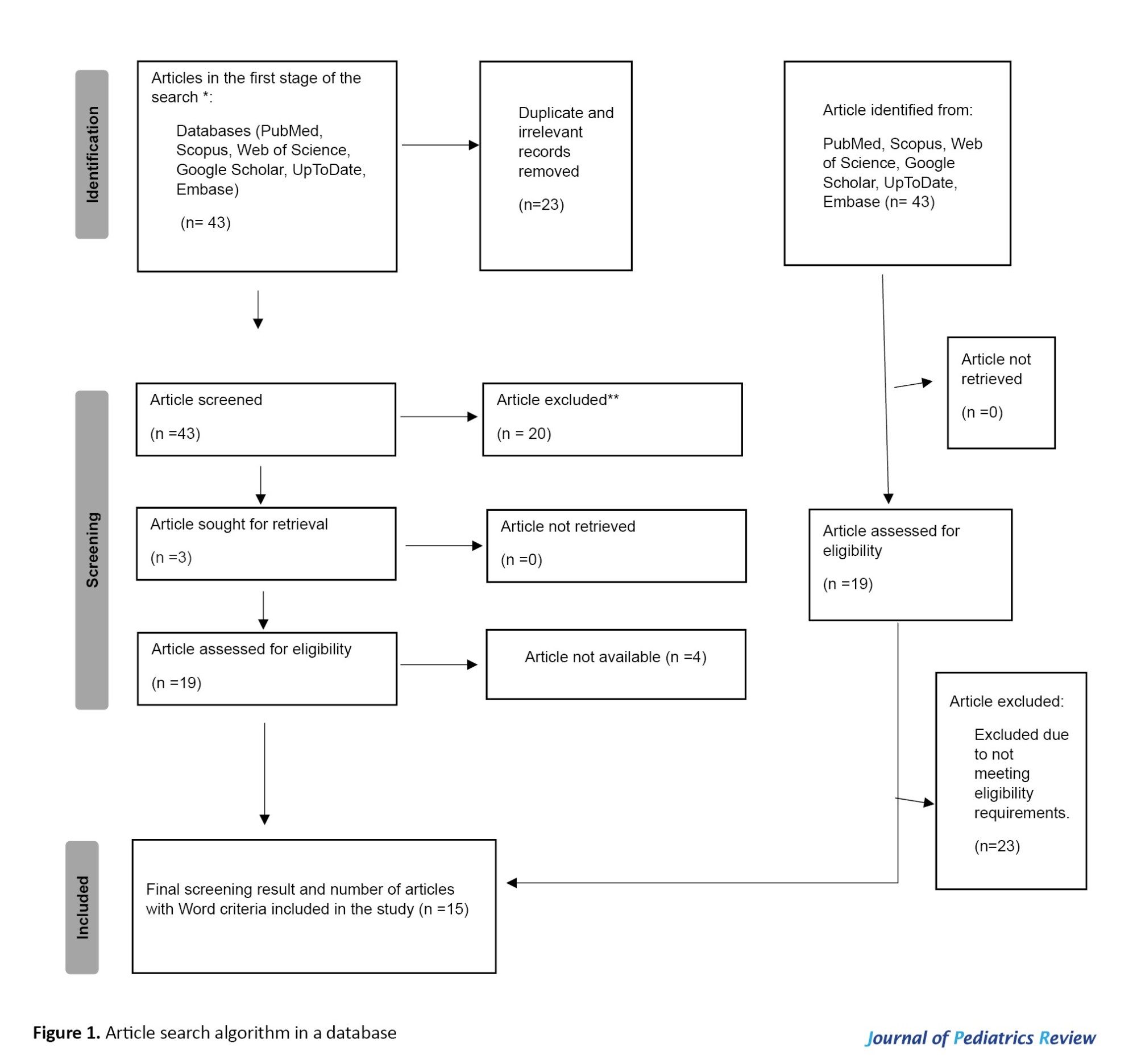
Articles not directly related to caregivers of children with disabilities or to unrelated populations were excluded to maintain specificity. Data extraction was performed by researchers one and two together. Sources were filtered based on criteria such as publication date, study type, and journal reputation. The extracted data was subjected to content analysis. Finally, the results were categorized and presented in this article (Figure 1).
Results
The findings were organized into thematic categories illustrating the multidimensional conditions faced by caregivers, including emotional stress, lack of support, social isolation, financial strain, and empowerment interventions. The review also highlights recommended support strategies and policies to improve caregiver wellbeing. This methodology ensures a structured, comprehensive analysis of the existing scholarship, enabling a holistic understanding of the complex realities experienced by caregivers of children with special needs (especially parents), also known as shadow nurses.
Discussion
Focusing solely on the child’s illness should not lead to neglecting the needs and wellbeing of those around them, especially the parents and caregivers of the sick child. Caring for a sick child places a great deal of physical, psychological, and emotional strain on the family and caregivers. If this support and care are not provided to the parents and those around them, it may lead to physical and mental exhaustion, chronic stress, and even a decrease in the quality of care for the child. Comprehensive and effective care occurs when the “family and caregivers” are supported and cared for in line with the “sick child.” This approach strengthens the support system, making it more stable and effective while enhancing quality of life for both the child and family. Parents or caregivers of ill children face multifaceted challenges spanning psychosocial, physical, social, economic, and cultural domains. They often endure high stress, anxiety, tension, and burnout from constant condition management, compounded by limited healthcare access, which leads to social isolation, financial strain, educational barriers, and rejection. Therefore, addressing these challenges is essential not only for the wellbeing of caregivers but also for the overall health outcomes of the children in their care. Topics such as caregiver support for chronic childhood illnesses, parental empowerment in pediatric healthcare, psychological assistance for parents of ill children, quality of life among caregivers of children with special health needs, social support effects on parents of hospitalized children, and interventions to alleviate caregiving burden in pediatric nursing all relate to supporting caregivers of sick children, particularly their parents.
Some children thrive in normal conditions with health and medical support and proper care. Still, due to the pressures and tensions during the child’s illness, the health of the parents and caregivers of the child is at risk, and some of these conditions remain permanent, and the parents bear the damage as a burden until the end of their lives. Therefore, in exchange for caring for the child, care for the parents must also be provided. This care can be financial support, health support, medical support, social support, emotional support, psychological support. A support-oriented educational program includes an educational and support section that, if implemented, increases parents’ level of information about disease recognition, adaptation skills, stress coping methods, disease recognition methods, causes and symptoms, prognosis, problem-solving development, time management, how to access resources and support services and charitable associations, and reduces the burden of parental care [36-38]. Interventions that assist parents in managing hospitalization through communication, empathy, education, tangible resources, or similar approaches effectively enhance parental wellbeing during and following their child’s hospital stay [24]. Interventions and supports should address reducing child behavioral problems, improving parental mental health, increasing marital quality and overall social support, and coping skills with stressors [26]. Research highlights the importance of developing educational, psychological, and social support initiatives to alleviate parental psychological distress. Self-compassion programs and online interventions have demonstrated effectiveness in lowering parental stress levels [1]. Family involvement takes precedence across all support modalities. When parents engage in cognitive-behavioral programs for children with chronic conditions, it enhances children’s proactive coping skills, reduces parental stress, and ultimately reduces psychological issues in children [32]. Family-centered empowerment programs enhance parents’ understanding of family-centered care principles among hospitalized children [35].
The challenges facing families with sick children are deep and widespread, and simply using the general word “support” alone cannot address these problems. In fact, what families with sick children need is systematic support, based on specific, scientific protocols, carried out in an organized and purposeful manner, to ensure the physical, mental, and social health of the entire family. It has highlighted challenges such as feeling unheard, chronic stress, and a change in identity for parents of sick children. Some research has highlighted the need for better access to support, more effective communication with healthcare professionals, and regular assessment of parental stress. Because parental stress is higher in families with sick children and requires more attention and support [26], caregivers of children with special needs face significant mental health challenges, primarily stemming from inadequate adjustment to their child’s disability and unmet personal needs [23]. Stress levels fluctuate based on disease severity and duration, the child’s age, parental gender and psychological status, marital satisfaction, relationship quality, and available support [26]. These differences will damage the foundation of the family. Decision-makers and policymakers at the micro and macro levels of society need to pay special attention to this issue.
What is important is that parents with sick children were motivated to participate in support programs because they were receptive to change and believed in the program’s value. They usually followed the support program and had a strong desire to improve their quality of life. In addition, empowering parents can increase their participation in daily care and treatment decisions, improve the management of the child’s symptoms, strengthen their information needs and skills, and enhance their advocacy capacity [27]. Empowerment programs not only improve parents’ skills but also support parents and caregivers throughout the child’s treatment process. So, empowering parents empowers children.
Strategies for supporting parents with sick children include comprehensive psychological, financial, social, educational, and practical support that is provided systematically and purposefully to ensure the health and empowerment of the family: psychological support, financial support, social support, informational and educational support, practical and executive support, and continuous and planned support. Together, these strategies empower parents, reduce psychological and economic burden, increase family satisfaction and health, and improve the quality of care for the sick child. For example, support group technology in pediatric care is an effective strategy to foster interaction, provide emotional support, build interpersonal connections, and facilitate family adjustment to having a hospitalized child. These groups also create opportunities to express emotions, needs, expectations, and concerns, thereby strengthening social support networks [29, 39]. Programs linking parents with peers facing similar challenges effectively alleviate psychological distress and enhance wellbeing and quality of life for caregivers of children with special needs [33]. Peer support can significantly reduce parental psychological burden, improve caregivers’ mental health, and reduce parental stress [25, 34, 40].
Conclusion
Ensuring simple, practical access to counseling and support services for families of sick children plays a crucial role in fostering their mental and emotional tranquility. This support not only alleviates parents’ internal stress and worries but also boosts their motivation and hope for active participation in their child’s care and treatment. As mentioned, early intervention is not only effective in accelerating the growth and recovery of children but also lays the foundation for better, continuous, and more efficient care by promoting family awareness and support. Special attention is needed in supporting parents, especially “shadow nurses” (parents and caregivers who play the main role in care but are less visible and less supported). In many cases, these parents play a key role in the treatment and care process more than the child themselves, and therefore: Their mental, physical, and social status should be continuously assessed. They need to benefit from multilateral and coordinated support from various institutions and organizations. Collaboration among health, welfare, education, municipal, university, sports organizations, and other relevant institutions is essential for designing and implementing special support programs for parents. Support structures should be such that assessment, education, counseling, financial support, and welfare services are provided to families in an integrated and continuous manner. Supporting caregivers of children with special needs is fundamental to preserving the wellbeing of these families. Essential services such as specialized training, insurance coverage, and parental guidance form the backbone of this support. Equally vital are the informal networks—friends, family, and local communities—that provide emotional and practical assistance, alleviating daily stresses and enhancing caregivers’ mental health. By nurturing both formal and informal support systems, we can build resilient families that not only sustain caregivers but also foster the holistic development and care of children.
In essence, implementing this approach demands developing a comprehensive, systematic, multi-sectoral support framework that prioritizes families and acknowledges their pivotal role in caring for and treating ill children.
Study limitations
The limitations of studies on parents of sick children include several issues, the most important of which can be summarized as follows: the diversity and complexity of disease conditions, the psychological burden and stress on parents, limited access and sampling, environmental and social effects, data inconsistencies and information deficiencies, and methodological limitations. These limitations suggest that researchers should pay special attention to careful sampling, covering the diverse conditions of children and families, the types of disease and disability among children, and using combined quantitative and qualitative methods, while accounting for environmental and systemic factors in the design of future studies to obtain more comprehensive and practical results. Paying attention to these limitations indicates the conditions for conducting more detailed studies, so that, if the management of treatment and rehabilitation of sick children is carried out correctly, not only the child but also the family will enjoy an appropriate quality of life throughout their lives.
Ethical Considerations
Compliance with ethical guidelines
This article is a meta-analysis with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflicts of interest
The authors declared no conflict of interest.
References
Achild’s illness or disability affects the whole family. A significant number of children around the world has some disability. According to the World Health Organization (WHO) and UNICEF, this figure includes more than 240 million children in the world, for every 10 children there is a disabled child (1/10). Since there are no exact statistics on the number of families with disabled children, given the number of disabled children (more than 240 million disabled children), it can be estimated that millions of families in the world have disabled children. It is noteworthy that 75% of children with disabilities live in developing countries, but in the United States, approximately one-fifth of families are responsible for caring for a child with a chronic health condition [1]. In any case, this impressive figure shows the urgent need to support these children. It shows the family as the most important and closest caregivers for children. Children inevitably experience illness during their early years, with conditions ranging from acute issues such as the common cold to chronic diseases like cystic fibrosis or disabilities [2]. Still, the hospitalization of a child is a source of risk, stress, and strain for parents [3-8]. Hospitalization represents a critical experience for ill children, significantly disrupting the equilibrium between the children and their families. Admission to the hospital exposes them to challenging and often distressing procedures that induce both physical and psychological discomfort [9].
A child’s illness generates substantial stress and anxiety across the entire family. Beyond impacting the child directly, it also influences parents, siblings, and other relatives [3-8]. Some illnesses improve over time, and the child regains his health, but some illnesses are chronic, and disabilities remain with the person for the rest of his life, which imposes a lot of pressure on the child and the family. It creates a psychological burden, a care burden, an economic burden, a social burden, etc., for all family members and leads to physical, mental, and psychological tensions.
Not only does the sick child need support and care, but the child’s parents, caregivers, and child care providers do as well. Throughout a child’s hospitalization, care is provided not only to the child but also to their parents. Parents are considered vital members of the care team and are encouraged to remain with their child in the hospital ward. Their presence contributes to the child’s safety and reduces anxiety. Additionally, nurses support the child’s adjustment to the new environment by fostering interactions and collaboration between the child and the parent [10]. While parents or caregivers often embrace their role willingly, the extra demands and pressures of caregiving—frequently coupled with insufficient skills, resources, and support—expose them and their families to heightened risks of stress, diminished functioning, declining wellbeing, and a lower quality of life. In fact, the quality of individual, family, professional, and social life of family members will change due to the child’s illness [11]. However, improved emotional and psychological wellbeing among parents correlates with enhanced mental and physical health outcomes in their children [12-14]. Therefore, implementing strategies to build parental capacity and improve their wellbeing and quality of life is vital for comprehensively supporting the growth of children with disabilities [15]. To enhance children’s health outcomes, the caregiving needs of their parents must be prioritized [16].
Studies indicate that caregiving frequently imposes substantial stress, creating social, emotional, behavioral, and financial burdens on caregivers, which heightens their vulnerability to mental health issues like depression and anxiety, as well as physical ailments. Caregivers are just as susceptible to psychological stress as patients [16-20]. So, decisions must be made to prevent potential harm to the child and the child’s caregivers and parents, to mitigate hospitalization’s adverse effects on children. Parents should participate in all nursing interventions, and there should be effective communication among children, parents, and nurses. Providing clear medical information about the child’s condition addresses questions and alleviates parental anxiety [21].
Family-centered support for sick children is one of the basic and effective strategies for improving the child’s and the family’s physical, psychological, and social status. Experience has shown that when the families of sick children, especially parents, receive the necessary support, not only will the child have a greater chance of achieving treatment goals and personal growth, but family and marital relationships will also improve, and greater resilience to the stresses, pressures, and dangers of the disease will be achieved. Different support areas include psychological support (receiving counseling and education to cope with emotional pressures and accept new living conditions), financial support (providing medical, pharmaceutical, and care costs that are usually beyond the family’s ability), social support (creating connections with associations, support groups, and benefiting from the experiences of similar families to reduce isolation and increase hope), practical and executive support (facilitating access to medical services, rehabilitation, transportation, and special care), and informational support (access to educational resources and accurate information about the disease, care methods, and better management of the child’s condition).
Family-centered practice, the primary framework for supporting children with developmental delays and disabilities, addresses stressors while leveraging family strengths to enhance overall family functioning [22]. In this regard, family-centered support is a comprehensive approach that places not only the child, but also the entire family on the path to empowerment and coping with the crisis, and prevents negative psychological and social consequences. Creating such support can maintain the mental health of children, parents, and other family members and enhance their level of cooperation and adaptation.
The health and quality of life of patients are as important as those of their parents, companions, and caregivers. In this article, caregivers include parents, siblings, grandparents, educators, and child care providers, although everyone in direct contact with the child, in the family and social environment, is part of the chain of caregivers for children with special needs. The present study points to those who are missing and need support and care—the forgotten who have a very important mission in caring for sick and disabled children. Accordingly, the purpose of the present study is to investigate the circumstances of missing persons in need of care, with a focus on caregivers of children with special needs. In this study, shadow nurses are referred to as parents, caregivers, and nurses of sick children. To give power to sick children, their parents must also be empowered, and their quality of life must be improved. They need more support and care than parents of normal or healthy children. This study emphasizes the need for tailored support systems—such as education, counseling, and community resources—to reinforce caregiver resilience and improve coping, thereby enhancing the quality of life for children and their families.
Materials and Methods
This systematic review adhered to PRISMA guidelines and searched databases including PubMed, Scopus, Web of Science, UpToDate, Google Scholar, and Embase. Keywords from Table 1 were combined using Boolean operators to identify relevant Persian and English articles published between 2011 and 2025.
Caregivers of children with special needs include children with acute or chronic disabilities, physical, mental, sensory, or developmental disabilities, or specific and chronic illnesses (CI) who require specialized and daily care. Caregivers must be adults (usually over 18). They may include parents, family members, day care nurses, social workers, and other formal or informal caregivers responsible for the child’s ongoing daily care.
The children in care must have special needs, including requiring daily care, chronic or long-term disabilities, or specific medical conditions (children with disabilities, gifted children, talented children, children with special talents, children with impairments, differently-abled children). First, researcher one screened the titles and abstracts of all retrieved articles. Selected relevant articles then underwent full-text evaluation. In the second stage, the researcher number two conducted the content analysis of the selected articles. After extracting the eligible articles, the general data, study characteristics, and results were summarized in Table 2.
Articles not directly related to caregivers of children with disabilities or to unrelated populations were excluded to maintain specificity. Data extraction was performed by researchers one and two together. Sources were filtered based on criteria such as publication date, study type, and journal reputation. The extracted data was subjected to content analysis. Finally, the results were categorized and presented in this article (Figure 1).
Results
The findings were organized into thematic categories illustrating the multidimensional conditions faced by caregivers, including emotional stress, lack of support, social isolation, financial strain, and empowerment interventions. The review also highlights recommended support strategies and policies to improve caregiver wellbeing. This methodology ensures a structured, comprehensive analysis of the existing scholarship, enabling a holistic understanding of the complex realities experienced by caregivers of children with special needs (especially parents), also known as shadow nurses.
Discussion
Focusing solely on the child’s illness should not lead to neglecting the needs and wellbeing of those around them, especially the parents and caregivers of the sick child. Caring for a sick child places a great deal of physical, psychological, and emotional strain on the family and caregivers. If this support and care are not provided to the parents and those around them, it may lead to physical and mental exhaustion, chronic stress, and even a decrease in the quality of care for the child. Comprehensive and effective care occurs when the “family and caregivers” are supported and cared for in line with the “sick child.” This approach strengthens the support system, making it more stable and effective while enhancing quality of life for both the child and family. Parents or caregivers of ill children face multifaceted challenges spanning psychosocial, physical, social, economic, and cultural domains. They often endure high stress, anxiety, tension, and burnout from constant condition management, compounded by limited healthcare access, which leads to social isolation, financial strain, educational barriers, and rejection. Therefore, addressing these challenges is essential not only for the wellbeing of caregivers but also for the overall health outcomes of the children in their care. Topics such as caregiver support for chronic childhood illnesses, parental empowerment in pediatric healthcare, psychological assistance for parents of ill children, quality of life among caregivers of children with special health needs, social support effects on parents of hospitalized children, and interventions to alleviate caregiving burden in pediatric nursing all relate to supporting caregivers of sick children, particularly their parents.
Some children thrive in normal conditions with health and medical support and proper care. Still, due to the pressures and tensions during the child’s illness, the health of the parents and caregivers of the child is at risk, and some of these conditions remain permanent, and the parents bear the damage as a burden until the end of their lives. Therefore, in exchange for caring for the child, care for the parents must also be provided. This care can be financial support, health support, medical support, social support, emotional support, psychological support. A support-oriented educational program includes an educational and support section that, if implemented, increases parents’ level of information about disease recognition, adaptation skills, stress coping methods, disease recognition methods, causes and symptoms, prognosis, problem-solving development, time management, how to access resources and support services and charitable associations, and reduces the burden of parental care [36-38]. Interventions that assist parents in managing hospitalization through communication, empathy, education, tangible resources, or similar approaches effectively enhance parental wellbeing during and following their child’s hospital stay [24]. Interventions and supports should address reducing child behavioral problems, improving parental mental health, increasing marital quality and overall social support, and coping skills with stressors [26]. Research highlights the importance of developing educational, psychological, and social support initiatives to alleviate parental psychological distress. Self-compassion programs and online interventions have demonstrated effectiveness in lowering parental stress levels [1]. Family involvement takes precedence across all support modalities. When parents engage in cognitive-behavioral programs for children with chronic conditions, it enhances children’s proactive coping skills, reduces parental stress, and ultimately reduces psychological issues in children [32]. Family-centered empowerment programs enhance parents’ understanding of family-centered care principles among hospitalized children [35].
The challenges facing families with sick children are deep and widespread, and simply using the general word “support” alone cannot address these problems. In fact, what families with sick children need is systematic support, based on specific, scientific protocols, carried out in an organized and purposeful manner, to ensure the physical, mental, and social health of the entire family. It has highlighted challenges such as feeling unheard, chronic stress, and a change in identity for parents of sick children. Some research has highlighted the need for better access to support, more effective communication with healthcare professionals, and regular assessment of parental stress. Because parental stress is higher in families with sick children and requires more attention and support [26], caregivers of children with special needs face significant mental health challenges, primarily stemming from inadequate adjustment to their child’s disability and unmet personal needs [23]. Stress levels fluctuate based on disease severity and duration, the child’s age, parental gender and psychological status, marital satisfaction, relationship quality, and available support [26]. These differences will damage the foundation of the family. Decision-makers and policymakers at the micro and macro levels of society need to pay special attention to this issue.
What is important is that parents with sick children were motivated to participate in support programs because they were receptive to change and believed in the program’s value. They usually followed the support program and had a strong desire to improve their quality of life. In addition, empowering parents can increase their participation in daily care and treatment decisions, improve the management of the child’s symptoms, strengthen their information needs and skills, and enhance their advocacy capacity [27]. Empowerment programs not only improve parents’ skills but also support parents and caregivers throughout the child’s treatment process. So, empowering parents empowers children.
Strategies for supporting parents with sick children include comprehensive psychological, financial, social, educational, and practical support that is provided systematically and purposefully to ensure the health and empowerment of the family: psychological support, financial support, social support, informational and educational support, practical and executive support, and continuous and planned support. Together, these strategies empower parents, reduce psychological and economic burden, increase family satisfaction and health, and improve the quality of care for the sick child. For example, support group technology in pediatric care is an effective strategy to foster interaction, provide emotional support, build interpersonal connections, and facilitate family adjustment to having a hospitalized child. These groups also create opportunities to express emotions, needs, expectations, and concerns, thereby strengthening social support networks [29, 39]. Programs linking parents with peers facing similar challenges effectively alleviate psychological distress and enhance wellbeing and quality of life for caregivers of children with special needs [33]. Peer support can significantly reduce parental psychological burden, improve caregivers’ mental health, and reduce parental stress [25, 34, 40].
Conclusion
Ensuring simple, practical access to counseling and support services for families of sick children plays a crucial role in fostering their mental and emotional tranquility. This support not only alleviates parents’ internal stress and worries but also boosts their motivation and hope for active participation in their child’s care and treatment. As mentioned, early intervention is not only effective in accelerating the growth and recovery of children but also lays the foundation for better, continuous, and more efficient care by promoting family awareness and support. Special attention is needed in supporting parents, especially “shadow nurses” (parents and caregivers who play the main role in care but are less visible and less supported). In many cases, these parents play a key role in the treatment and care process more than the child themselves, and therefore: Their mental, physical, and social status should be continuously assessed. They need to benefit from multilateral and coordinated support from various institutions and organizations. Collaboration among health, welfare, education, municipal, university, sports organizations, and other relevant institutions is essential for designing and implementing special support programs for parents. Support structures should be such that assessment, education, counseling, financial support, and welfare services are provided to families in an integrated and continuous manner. Supporting caregivers of children with special needs is fundamental to preserving the wellbeing of these families. Essential services such as specialized training, insurance coverage, and parental guidance form the backbone of this support. Equally vital are the informal networks—friends, family, and local communities—that provide emotional and practical assistance, alleviating daily stresses and enhancing caregivers’ mental health. By nurturing both formal and informal support systems, we can build resilient families that not only sustain caregivers but also foster the holistic development and care of children.
In essence, implementing this approach demands developing a comprehensive, systematic, multi-sectoral support framework that prioritizes families and acknowledges their pivotal role in caring for and treating ill children.
Study limitations
The limitations of studies on parents of sick children include several issues, the most important of which can be summarized as follows: the diversity and complexity of disease conditions, the psychological burden and stress on parents, limited access and sampling, environmental and social effects, data inconsistencies and information deficiencies, and methodological limitations. These limitations suggest that researchers should pay special attention to careful sampling, covering the diverse conditions of children and families, the types of disease and disability among children, and using combined quantitative and qualitative methods, while accounting for environmental and systemic factors in the design of future studies to obtain more comprehensive and practical results. Paying attention to these limitations indicates the conditions for conducting more detailed studies, so that, if the management of treatment and rehabilitation of sick children is carried out correctly, not only the child but also the family will enjoy an appropriate quality of life throughout their lives.
Ethical Considerations
Compliance with ethical guidelines
This article is a meta-analysis with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflicts of interest
The authors declared no conflict of interest.
References
- Franco PL, Knox MC, Gulbas LE, Gregory K. Exploring how parents of chronically ill children learn self-compassion. Discov Psychol. 2024; 4(1):175. [DOI:10.1007/s44202-024-00287-3]
- Cahayag V. Hospitalization and child development: Effects on sleep, developmental stages, and separation anxiety. [Bachelor thesis]. Marin County: Dominican University of California; 2020. [Link]
- Oxley R. Parents› experiences of their child›s admission to paediatric intensive care. Nurs child Young People. 2015; 27(4). [DOI:10.7748/ncyp.27.4.16.e564] [PMID]
- Franck LS, Wray J, Gay C, Dearmun AK, Lee K, Cooper BA. Predictors of parent post-traumatic stress symptoms after child hospitalization on general pediatric wards: A prospective cohort study. Int J Nurs Stud. 2015;52(1):10-21. [DOI:10.1016/j.ijnurstu.2014.06.011] [PMID]
- Rapoport A, Weingarten K. Improving quality of life in hospitalized children. Pediatr Clin. 2014; 61(4):749-60. [DOI:10.1016/j.pcl.2014.04.010] [PMID]
- Diaz-Caneja A, Gledhill J, Weaver T, Nadel S, Garralda E. A child›s admission to hospital: A qualitative study examining the experiences of parents. Intensive Care Med. 2005; 31(9):1248-54. [DOI:10.1007/s00134-005-2728-8] [PMID]
- Bent KN, Keeling A, Routson J. Home from the PICU: Are parents ready? Am J Matern Child Nurs. 1996; 21(2):80-4. [DOI:10.1097/00005721-199603000-00011] [PMID]
- Placencia F, McCullough L. Biopsychosocial risks of parental care for high-risk neonates: Implications for evidence-based parental counseling. J Perinatol. 2012; 32(5):381-6. [DOI:10.1038/jp.2011.109] [PMID]
- Barros I, Lourenço M, Nunes E, Charepe Z. Nursing interventions promoting child/youth/family adaptation to hospitalization: A scoping review. Enferm Glob. 2021; 20(1):577-95. [DOI:10.6018/eglobal.413211]
- Witanowska J, Warmuz-Wancisiewicz AI, Ullman A. Hospitalization as a difficult situation for children in the opinion of parents and nursery personnel. Polish Nursing/Pielegniarstwo Polskie. 2019; 72(2). [Link]
- Bhopti A, Brown T, Lentin P. Family quality of life: A key outcome in early childhood intervention services-A scoping review. J Early Interv. 2016; 38(4):191-211. [DOI:10.1177/1053815116673182]
- National Research Council (US) and Institute of Medicine (US) Committee on Depression, Parenting Practices, and the Healthy Development of Children. Depression in parents, parenting, and children: Opportunities to improve identification, treatment, and prevention. Washington (DC): National Academies Press; 2009. [DOI: 10.17226/12565] [PMID]
- Landolt MA, Ystrom E, Sennhauser FH, Gnehm HE, Vollrath ME. The mutual prospective influence of child and parental post-traumatic stress symptoms in pediatric patients. J Child Psychol Psychiatry. 2012; 53(7):767-74. [DOI:10.1111/j.1469-7610.2011.02520.x] [PMID]
- Als LC, Picouto MD, Hau SM, Nadel S, Cooper M, Pierce CM, et al. Mental and physical wellbeing following admission to pediatric intensive care. Pediatr Crit Care Med. 2015; 16(5):e141-e9. [DOI:10.1097/PCC.0000000000000424] [PMID]
- Bailey Jr DB, Bruder MB, Hebbeler K, Carta J, Defosset M, Greenwood C, et al. Recommended outcomes for families of young children with disabilities. J Early Interv. 2006; 28(4):227-51. [DOI:10.1177/105381510602800401]
- Khalili A, Cheraghi F, Fayyazi A, Soltanian A, Shamsaei F. Care Needs of Parents With Epileptic Children: A systematic review. J Pediatr Rev. 2025; 13(1):5-16. [DOI:10.32598/jpr.13.1.1166.2]
- Nevin SM, Wakefield CE, Schilstra CE, McGill BC, Bye A, Palmer EE. The information needs of parents of children with early-onset epilepsy: A systematic review. Epilepsy Behav. 2020; 112:107382. [DOI:10.1016/j.yebeh.2020.107382] [PMID]
- Hussain MM, Zulfiqar Z, Ishfaq K, Ghaffari AS. Psychosocial and economic problems faced by parent›s of children with epilepsy. Rev Educ Adm Law. 2021; 4(2):521-30. [DOI:10.47067/real.v4i2.167]
- Seid S, Demilew D, Yimer S, Mihretu A. Prevalence and associated factors of mental distress among caregivers of patients with epilepsy in Ethiopia: A cross-sectional study design. Psychiatry J. 2018; 2018(1):2819643. [DOI:10.1155/2018/2819643] [PMID]
- Zhang M, Zhang H, Hu S, Zhang M, Fang Y, Hu J, et al. Investigation of anxiety, depression, sleep, and family function in caregivers of children with epilepsy. Front Neurol. 2021; 12:744017. [DOI:10.3389/fneur.2021.744017] [PMID]
- Suparto TA, Somantri B, Andriani S, Puspita APW, Rohaedi S, Amalia L, et al. Parents› roles in overcoming the impact of hospitalization on preschool children. Paper presented at: 4th International Conference on Sport Science, Health, and Physical Education (ICSSHPE 2019). 8 AND 9 october 2019; Bandung, Indonesia. [Link]
- Dunst CJ, Trivette CM. Capacity-building family-systems intervention practices. Family support and family caregiving across disabilities. Oxfordshire: Routledge; 2014. [Link]
- Zamani N, Ansari Shahidi M. [Prevalence of psychological disorders among caregivers of children with intellectual disabilities and motor disabilities in Hamadan [Persian]. Q J Child Ment Health. 2017; 4(3):119-29. [Link]
- Doupnik SK, Hill D, Palakshappa D, Worsley D, Bae H, Shaik A, et al. Parent coping support interventions during acute pediatric hospitalizations: A meta-analysis. Pediatrics. 2017; 140(3). [DOI:10.1542/peds.2016-4171] [PMID]
- Torkzahrani S, Karamolahi Z, Akbarzadeh Ba, Chehreh H. [Eficacy of peer support on growth patterns of infants below one year old (Persian)]. J Ilam Uni Med Sci. 2018: 26(1):176-86. [Link]
- Pinquart M. Parenting stress in caregivers of children with chronic physical condition-A meta-analysis. Stress Health. 2018; 34(2):197-207. [DOI:10.1002/smi.2780] [PMID]
- Ashcraft LE, Asato M, Houtrow AJ, Kavalieratos D, Miller E, Ray KN. Parent empowerment in pediatric healthcare settings: A systematic review of observational studies. Patient Cent Outcomes Res. 2019; 12(2):199-212. [DOI:10.1007/s40271-018-0336-2] [PMID]
- Arief YS, Rachmawati PD. Parent empowerment program in caring for children with leukemia. Enferm Clin. 2019; 29:897-9. [DOI:10.1016/j.enfcli.2019.04.136]
- Moraes ES, Silva CCd, Melo LdL, Mendes-Castillo AMC. Support group for families with children in a pediatric intensive care unit. Rev Bras Enferm. 2021; 75(2):e20210097. [DOI:10.1590/0034-7167-2021-0097] [PMID]
- Dehvan F, Naderi P, Seidi J. [The effect of educational support program on the amount of caregiver burden on the parents of children with cancer admitted to the oncology Ward of Besat Hospital in Sanandaj, 2021 (Persian)]. SJKU 2023; 28(3):87-100. [Link]
- Smith S, Tallon M, Clark C, Jones L, Mörelius E. «You Never Exhale Fully Because You›re Not Sure What›s NEXT»: Parents› experiences of stress caring for children with chronic conditions. Front Pediatr. 2022; 10:902655. [DOI:10.3389/fped.2022.902655] [PMID]
- Willemen AM, Kuzminskaite E, Maurice-Stam H, Grootenhuis MA, Last BF, Schuengel C, et al. The working mechanisms of parental involvement in interventions for children with chronic illness. J Child Fam Stud. 2022; 31(11):3037-46. [DOI:10.1007/s10826-022-02329-7]
- Lancaster K, Bhopti A, Kern ML, Taylor R, Janson A, Harding K. Effectiveness of peer support programmes for improving wellbeing and quality of life in parents/carers of children with disability or chronic illness: A systematic review. Child Care Health Dev. 2023; 49(3):485-96. [DOI:10.1111/cch.13063] [PMID]
- Shoghi M, Heidari Rohban A, Kheradmand M. Evaluation of peer education on parental stress and situational anxiety in mothers of premature infants hospitalized in NICU (Persian)]. J Mazandaran Uni Med Sci. 2024; 34(234):101-13. [Link]
- Motamedifard S, Movahedimoghadam F, Motamed F, Begjani J. The effect of family-centered empowerment training on the perception of family-centered care by parents of hospitalized children.J Emerg Health Care. 2024;13(4):0-. [Link]
- Northouse LL, Katapodi MC, Song L, Zhang L, Mood DW. Interventions with family caregivers of cancer patients: meta-analysis of randomized trials. CA A Cancer J Clin. 2010; 60(5):317-39. [DOI:10.3322/caac.20081] [PMID]
- Setiawan A, Keliat BA, Rustina Y, Prasetyo S. The effectiveness of educative, supportive, and administrative cycle (ESA-C) clinical supervision model in improving the performance of public hospital nurses. KnE Life Sci. 2019; 41-56-41-56. [DOI:10.18502/kls.v4i15.5734]
- Khorami Markani A, saheli S, sakhaei S, khalkhali H. [Assessment the effect of family centered care educational program on home care knowledge among care givers of patients with chronic renal failure under hemodialysis (Persian)]. Nurs Mid J. 2015; 13(5):386-94 2015. [Link]
- Balbino FS, Yamanaka CI, Balieiro M, Mandetta MA. Parent›s support group as a transforming experience for families at a neonatal unit. Escola Anna Nery. 2015; 19:297-302. [DOI:10.5935/1414-8145.20150040]
- Rajai N, Pishgooie SAH, Habibi H, Manochehri Z. The effect of peer-based education on the psychological burden of family caregivers of patients with schizophrenia admitted to the military hospital. Mil Caring Sci. 2019; 6(1):16-26. [DOI:10.29252/mcs.6.1.16]
Type of Study: Review Article |
Subject:
Exceptional children
Received: 2025/02/18 | Accepted: 2025/05/15 | Published: 2026/01/1
Received: 2025/02/18 | Accepted: 2025/05/15 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
