
Tue, May 19, 2026


Volume 14, Issue 1 (1-2026)
J. Pediatr. Rev 2026, 14(1): 13-28 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abdollahi Abed L, Vatankhah S, Choopani A. Risk Factors of Child Mortality in Iran: A Systematic Review and Narrative Synthesis. J. Pediatr. Rev 2026; 14 (1) :13-28
URL: http://jpr.mazums.ac.ir/article-1-789-en.html
URL: http://jpr.mazums.ac.ir/article-1-789-en.html



1- Department of Health Services Management, School of Health Management and Information Sciences, Iran University of Medical Sciences Tehran, Iran.
2- Hospital Management Research Center, Iran University of Medical Sciences, Tehran, Iran. ,vatankhah_s@yahoo.com
3- Health Management and Economics Research Center, Health Management Research Institute, Iran University of Medical Sciences, Tehran, Iran.
2- Hospital Management Research Center, Iran University of Medical Sciences, Tehran, Iran. ,
3- Health Management and Economics Research Center, Health Management Research Institute, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 676 kb]
(133 Downloads)
| Abstract (HTML) (325 Views)
Full-Text: (71 Views)
Introduction
Child mortality is widely recognized as a key indicator of population health, social welfare, and national development [1]. It was identified as one of the millennium development goals to reduce the child mortality rate by two-thirds between 1990 and 2015 [1]. The sustainable development goals further emphasize the importance of eliminating all preventable deaths among children under 5 years of age, aiming to reduce their mortality rate to no more than 25 per 1,000 live births by 2030 [2]. According to United Nations Children's Fund (UNICEF), children aged 1 to 59 months account for more than half of 4.8 million under-5 deaths globally, with pneumonia, diarrhea, and malaria as leading causes in 2023 [3]. While global child mortality has declined—from 77 per 1,000 in 2000 to 37 in 2023—disparities remain stark, particularly in low- and middle-income countries [3]. In high-income countries, this rate is as low as 5 per 1000 live births, whereas in low-income countries, child mortality is 13 times higher than in high-income nations [2]. Child mortality is not evenly distributed across the globe; 1.08 million of these deaths occurred in sub-Saharan Africa and South Asia alone [2].
These deaths are largely preventable and are strongly associated with social determinants such as limited access to health care, poor nutrition, unsafe water, inadequate sanitation, and maternal education [2, 3]. In many countries, child mortality is also influenced by structural inequalities and regional disparities in health service coverage [4]. Globally, well-documented risk factors include maternal age, birth spacing, family income, household education, and rural residence [3].
In Iran, the under-5 mortality rate has declined from earlier decades to 11.7 per 1000 live births in 2023 [5]. A substantial proportion of under-5 deaths in Iran occur among infants under one year of age [6]. Injuries have been identified as the leading cause of death among children aged 1 to 59 months in Iran, affecting both genders equally, though with varying distribution across provinces [4]. Globally, unintentional injuries are among the most prominent causes of child mortality, a trend also confirmed by studies conducted in Iran [7-10]. Poverty stands out as a major social determinant of child health, and poverty reduction programs have been linked to decreases in under-5 mortality in numerous countries [11]. The health and survival of children under 5 are also closely linked to the socioeconomic conditions of their families, with higher mortality rates observed in lower socioeconomic strata [12].
Within the Iranian health system, child health is administratively separated into neonates (0–28 days) and older children (1–59 months), with each managed by distinct departments within the Ministry of Health and Medical Education. While risk factors associated with neonatal mortality in Iran have been specifically addressed in a separate study [13], risk factors affecting children aged 1 to 59 months have received less consolidated attention, and existing research remains fragmented, with a comprehensive synthesis of risk factors specific to the post-neonatal period lacking. Thus, this study investigated the risk factors of children aged 1 to 59 months. Given that under-5 mortality is a multifactorial outcome encompassing the child, the mother, and pregnancy-related events [14], a systematic understanding of these contributors is critical for designing targeted and effective, evidence-based interventions to reduce child mortality. This study aimed to systematically review and synthesize the available evidence on risk factors for mortality among children aged 1 to 59 months in Iran.
Materials and Methods
This study was designed as a systematic review employing a narrative synthesis approach—all stages of the research and its reporting adhered to the PRISMA 2020 checklist. The timeframe for included studies was set to 2010-2023 to reflect the current situation better. The literature search was conducted in October 2023.
Given that Persian is the official language of Iran, Persian-language studies were included alongside English-language articles published in international journals. Search was conducted in Persian databases, including Iranian Research Institute for Information Science and Technology (IranDoc) and Scientific Information Database (SID), and in international databases of ScienceDirect, PubMed, and ISI Web of Science, using a combination of keywords for “child mortality,” “child*,” “infant,” “under five,” “under-5,” “U5M,” “mortalit*,” “death,” and “Iran*” and their Persian equivalents. Search strategy used for PubMed is presented here as an example: (((child*[Title/Abstract] OR infant[Title/Abstract] OR U5M[Title/Abstract] OR “under five” [Title/Abstract] OR “under 5”[Title/Abstract]) AND (mortalit*[Title/Abstract] OR death* [Title/Abstract]) AND (Iran*[Title/Abstract])) OR ((“child mortality”[Mesh] OR “infant mortality”[Mesh]) AND “Iran”[Mesh])) AND (2010:2024[pdat]). Search strategies used for other databases are provided in the supplementary file. Additionally, Google Scholar citation check was used to identify potentially relevant studies. The reference lists of the included articles were manually reviewed for additional sources.
A highly sensitive search strategy was employed. Although this strategy resulted in the retrieval of some irrelevant material, efforts were made to screen and assess all potentially relevant articles. This search strategy was refined through multiple iterations of keyword combinations to capture the broadest possible range of literature on under-5 mortality risk factors.
The inclusion criteria for the study stipulated that the article must focus on mortality in children aged 1 to 59 months or under 5 years; be conducted within Iran or in one or more of its cities, provinces, or hospitals; utilize multivariate regression to analyze risk factors; report odds ratios (OR); and be published in either Persian or English. On the other hand, studies were excluded if they focused on a specific disease or a particular subgroup of children, examined deaths from a single cause, lacked full text, included stillbirths in under-5 mortality figures, or were duplicate publications from the same dataset.
The study population comprised all articles, theses, and reports related to mortality among children aged 1 to 59 months in Iran. In line with the aforementioned categorization, articles covering mortality in children under 1 year, under 5 years, and specifically aged 1 to 59 months were included. No restrictions were placed on study type, and all study designs, including cohort and case-control studies that reported OR, could have been included in the review.
All retrieved articles were stored and managed using EndNote software, version X20. Data extraction was carried out using a pre-designed table containing two sections: General and specific information. General information included the year of publication, author, and study location. Specific information included study period, objectives, study design, age group studied, data collection tools and methods, sample size, statistical analysis techniques, significant and non-significant findings, and reported limitations. Two researchers performed data extraction from the articles. In the event of any disagreement, the issue was resolved by a third party.
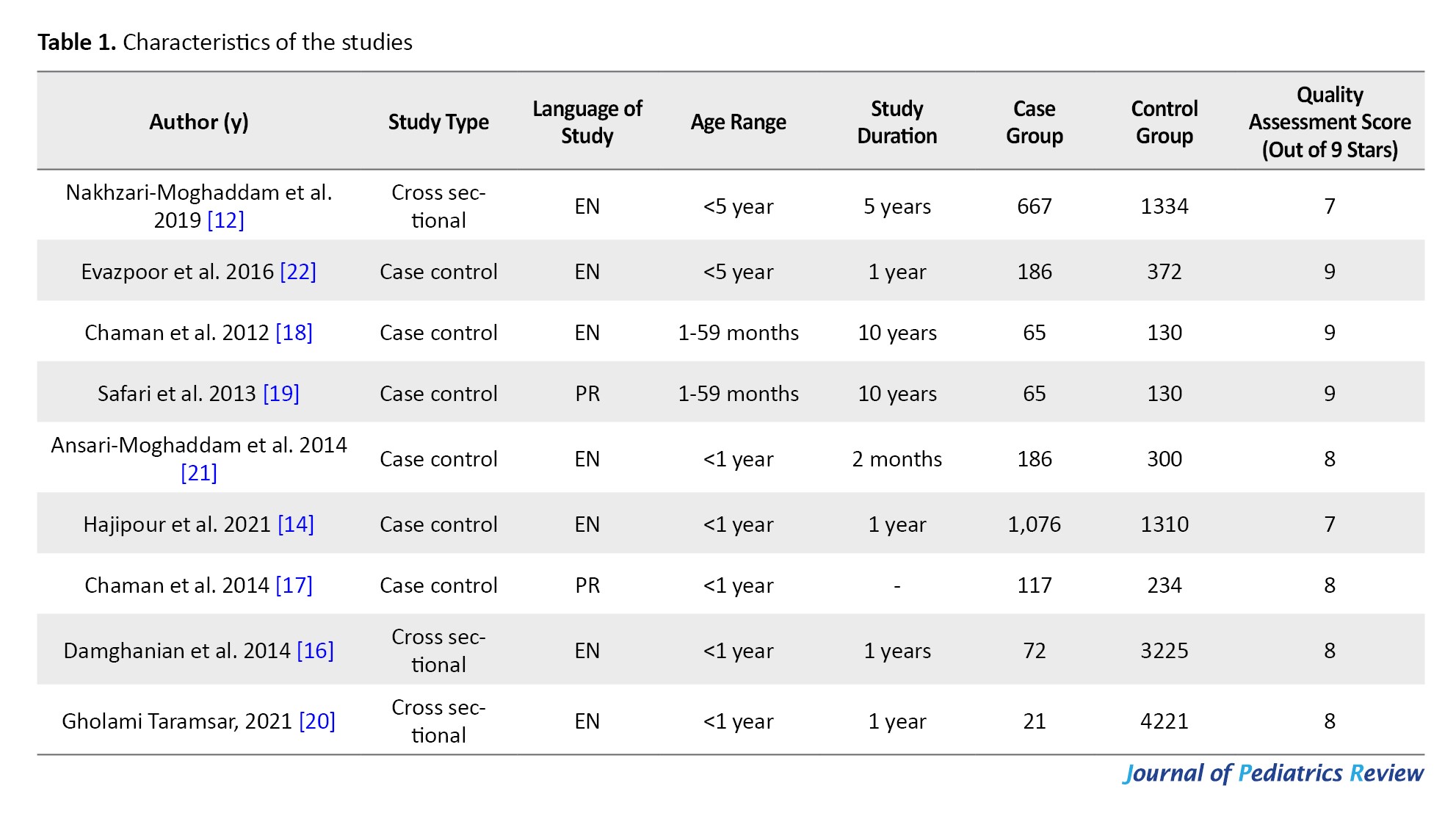
Ultimately, 6 case-control studies and 3 cross-sectional studies met the inclusion criteria. To assess their quality, the Newcastle-Ottawa scale was employed, following evidence from a systematic review and meta-analysis evaluating quality assessment tools [15]. This tool provides separate checklists for case-control and cross-sectional studies, with a maximum score of nine stars. Studies scoring 7 or higher were categorized as high-quality. All included studies in this review were assessed and determined to be of high quality (Table 1).
Heterogeneity assessment
Given the considerable heterogeneity among the included studies, conducting a meta-analysis was deemed inappropriate. This heterogeneity arose from several factors, including differences in target populations (e.g. age groups, geographic locations), variations in the classification and definition of risk factors, and diverse methods for outcome measurement. These discrepancies limited the comparability of study findings and posed significant challenges for synthesizing data quantitatively.
Moreover, the number of studies available for each specific risk factor was relatively small (fewer than 9 in most cases), which further constrained the statistical power and reliability of any pooled analysis. Due to these qualitative and quantitative limitations, a formal heterogeneity assessment (e.g. I2 statistic) and meta-analysis were not performed. Instead, a narrative synthesis approach was adopted to summarize and interpret the findings descriptively.
Results
Out of 2886 articles initially retrieved, 9 studies met the inclusion criteria and were included in this systematic review. The process of article selection and exclusion at each stage is illustrated in Figure 1.
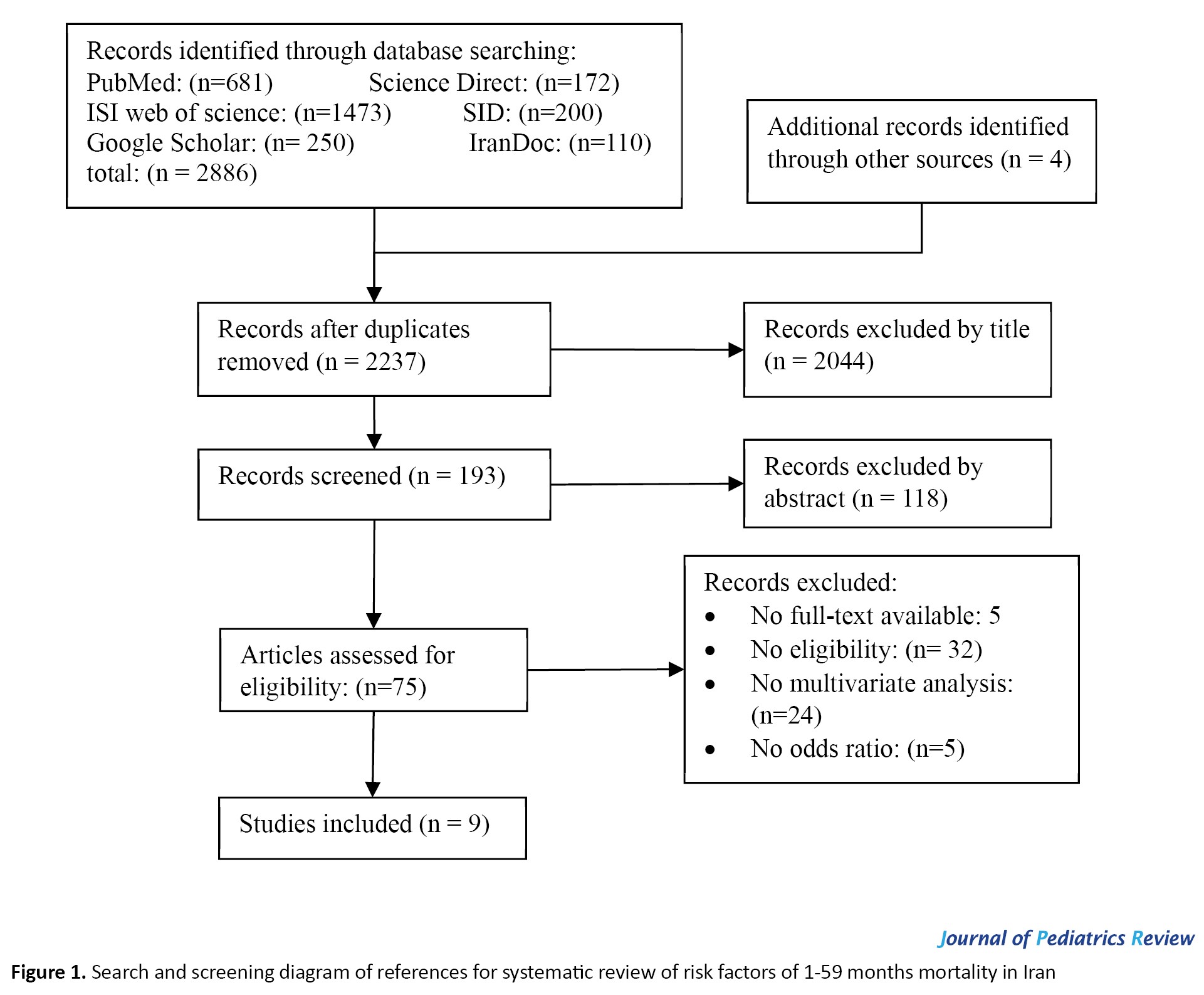 The included studies were grouped by child age into three categories: 5 studies focused on children under 1 year, 2 on children aged 1 to 59 months, and 2 on children under 5 years. Geographically, 4 studies were conducted in Shahroud. Others were conducted in Semnan, Zahedan, Zabol cities, and 1 multi-province study covering Hormozgan, Fars, Golestan, Kohgiluyeh and Boyer-Ahmad, South Khorasan, Kermanshah, Hamedan, and Yazd. Tables 2, 3 and 4 present the OR reported in the included studies, grouped by age.
The included studies were grouped by child age into three categories: 5 studies focused on children under 1 year, 2 on children aged 1 to 59 months, and 2 on children under 5 years. Geographically, 4 studies were conducted in Shahroud. Others were conducted in Semnan, Zahedan, Zabol cities, and 1 multi-province study covering Hormozgan, Fars, Golestan, Kohgiluyeh and Boyer-Ahmad, South Khorasan, Kermanshah, Hamedan, and Yazd. Tables 2, 3 and 4 present the OR reported in the included studies, grouped by age.
.jpg)
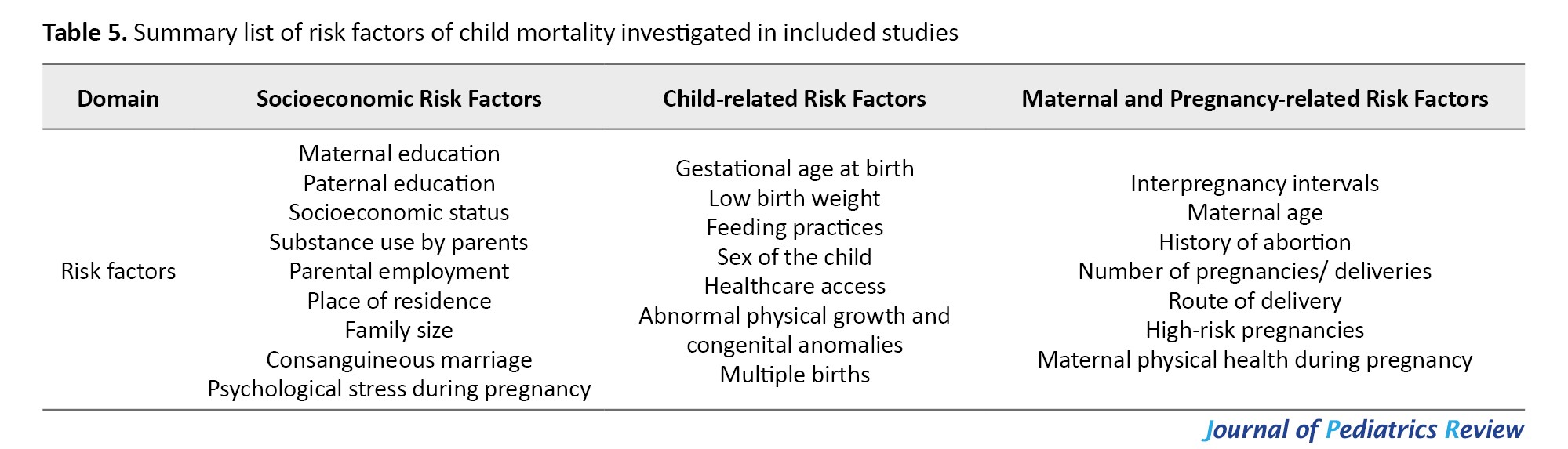
The included studies identified a wide range of risk factors associated with child mortality, grouped into three domains: Socioeconomic factors, maternal and pregnancy-related factors, and child-related factors. These were analyzed based on statistical significance and the age group studied. Table 5 lists the child mortality investigated in the included studies in Iran.
Socioeconomic risk factors
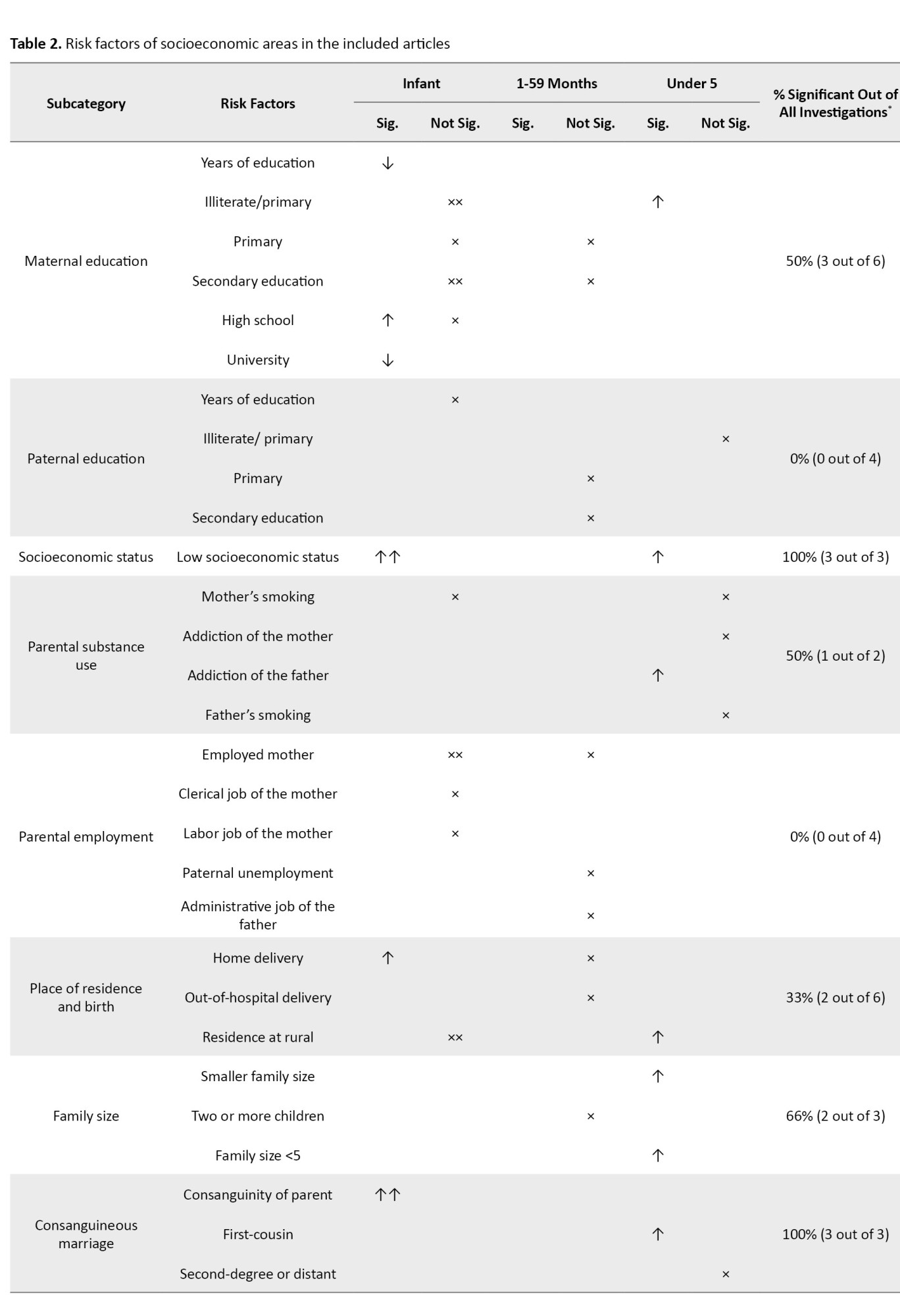
This category comprised 9 specific risk factors, with a total frequency of 33 instances across studies, of which 16(48%) were statistically significant.
Among socioeconomic variables, maternal education was one of the most frequently reported and influential factors. In 6 studies, higher maternal education was significantly associated with lower child mortality. Higher years of maternal education were significantly associated with reduced mortality among children under 1 year (OR=0.92) [16]. For instance, university-level and high school education reduced infant mortality by 60% and 55%, respectively [14]. Additionally, mothers with no formal education or only primary education had more than double the odds of under-five child mortality (OR=2.20) [12]. However, in four studies, primary and middle school education levels did not show significant associations with mortality [14, 17-19].
In contrast, paternal education was not significantly associated with child mortality in any of the four studies that evaluated this factor [12, 16, 18, 19].
Low socioeconomic status consistently emerged as a strong risk factor. All three studies examining this variable reported significant associations, with increased odds of child mortality [16, 20], particularly in children under 5 (OR=7.80) [12].
Smoking and substance abuse by parents were evaluated in two studies. While maternal smoking did not show a significant association [14], paternal addiction increased the risk of under-5 mortality by 2.6 times [12].
Parental employment status, including maternal employment and occupation type (e.g. laborer or civil servant), was examined in four studies. None of them reported significant associations with mortality [14, 16, 17, 19].
The place of residence and the delivery location were investigated in 6 studies. Home delivery was significantly associated with increased infant mortality by 5.8 times in Zahedan City, Iran [21], but not in other cities [18], while living in rural areas was a risk factor for under-5 mortality (OR=1.79) [22], but not in all studies investigated [14, 16]. Out-of-hospital delivery was examined in one study, which found no significant effect [19].
Family size showed mixed results. One study found that smaller families (less than 5 members) had higher under-5 mortality rates (OR=2.60) [12], whereas others found no significant associations [19, 22].
Consanguineous marriage was identified as a risk factor in three studies. First-cousin marriage significantly increased mortality risk with OR of 1.44 [14], 2.37 [16], and 3.92 [22], while marriages among more distant relatives did not show significant effects [22].
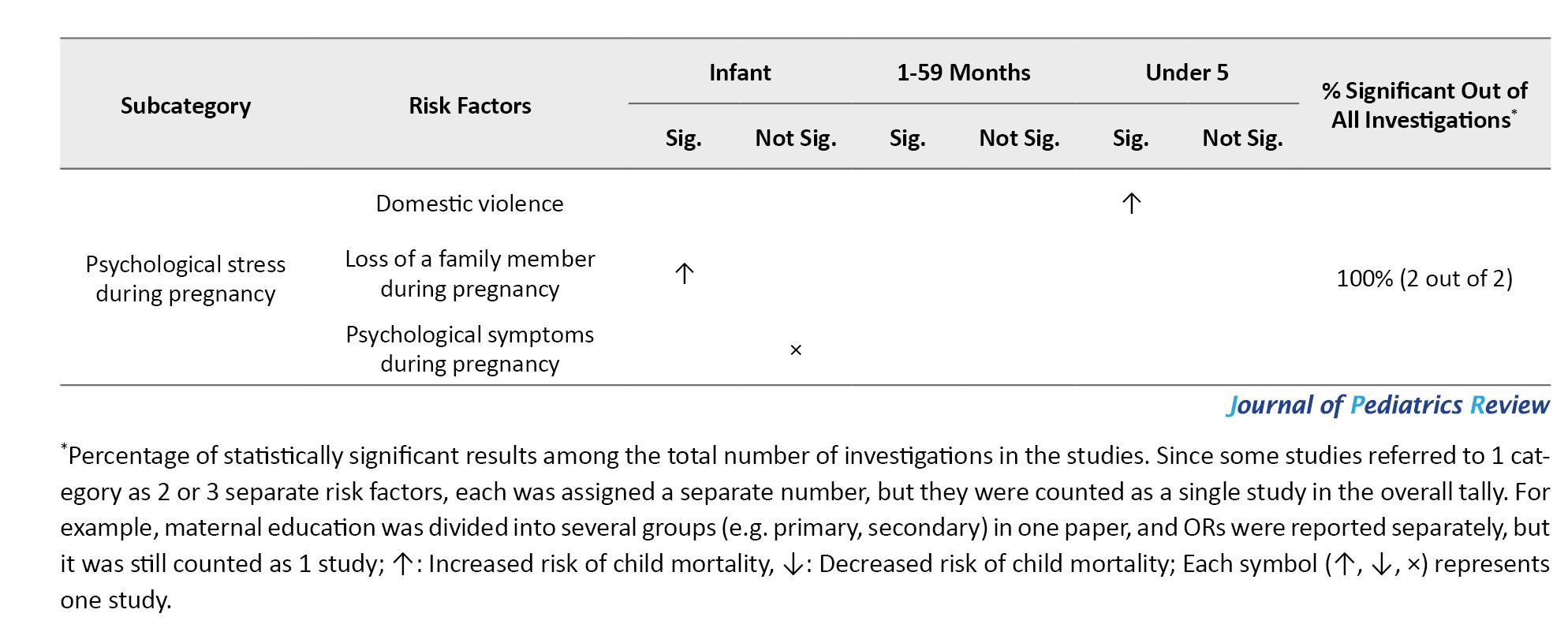
Psychological stress during pregnancy, specifically domestic violence, tripled the risk of under-five mortality [22], and loss of a family member during pregnancy increased infant mortality by 1.6 times [14]. However, general psychological symptoms during pregnancy did not show significant associations [14].
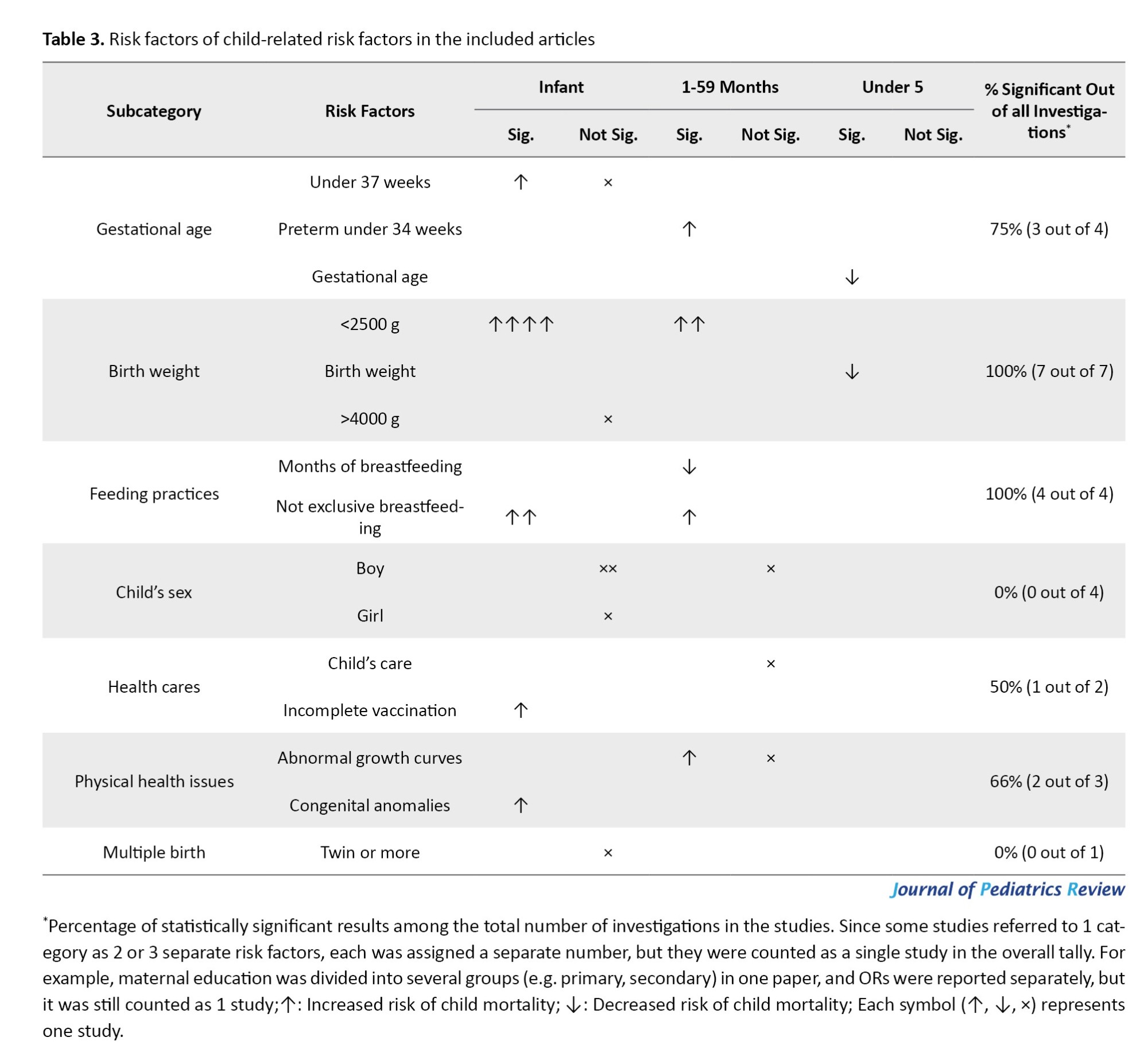
Child-related risk factors
This domain included 7 subcategories, totaling 25 instances, of which 17(68%) were statistically significant.
Gestational age at birth was assessed in 4 studies. Preterm birth, especially before 34 weeks, significantly increased the risk of mortality among children aged 1 to 59 months by 5 times [19]. Each additional week of gestation was associated with a 15% reduction in under-five mortality [22]. However, not all studies found statistically significant results for infants born at less than 37 weeks [21], but one did, showing a significant association with increased infant mortality (OR=3.50) [17].
Low birth weight (LBW) (<2500 g) was the most consistent and significant risk factor, with all seven studies reporting strong associations with increased mortality. [14, 16-19, 21, 22]. Each additional kilogram of birth weight was associated with an approximate 64% reduction in under-5 mortality [22]. LBW significantly increased child mortality with OR ranging from 2.83 [16] to 42.10 [21]. In contrast, high birth weight (>4000 g) did not show significant effects [14].
Feeding practices were evaluated in four studies. Exclusive breastfeeding reduced mortality among children aged 1 to 59 months [18], while the use of formula or other substitutes increased the risk by more than two [16] and four times in infant mortality [21].
The sex of the child did not show any significant association with mortality in any of the 4 studies that examined this variable [14, 16, 19, 21].
Healthcare access was evaluated in two studies. Incomplete vaccination was associated with a 14.9-fold increase in infant mortality in one study [21], while general child care access did not show consistent effects [19].
Abnormal physical growth and congenital anomalies were examined in three studies. One study found that abnormal growth was significantly associated with higher mortality among children aged 1-59 months (OR=7) [19], whereas another did not [18]. Congenital anomalies increased the risk of mortality among children under one year by 11.80 times [20].
Multiple births (e.g. twins) were not significantly associated with increased mortality [14].
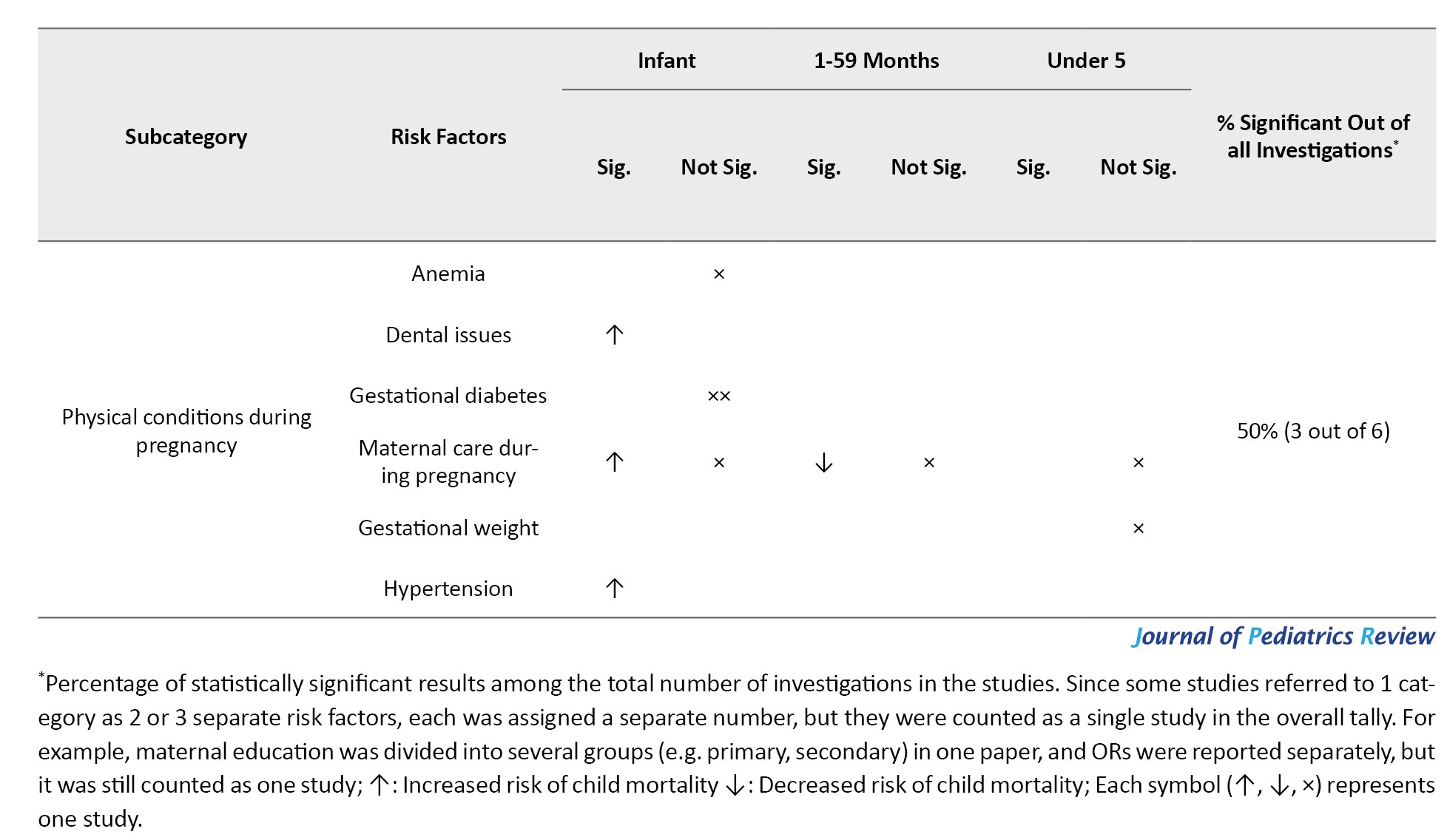
Maternal and pregnancy-related risk factors
This group included 7 specific factors, with 30 mentions across studies, of which 11(36%) were statistically significant.
Short interpregnancy intervals were evaluated in 5 studies [14, 16, 17, 19, 22]. An interval of less than 1 year (OR=2.70) and 1 to 3 years (OR=1.40) was associated with increased infant mortality [14]. However, in another study, intervals of less than three years were not consistently statistically significant among children aged 1-59 months [19].
Maternal age was examined in 4 studies. Only one significant finding was reported: Mothers aged 18–35 had lower infant mortality than those younger than 18 or older than 35 [14]. Other studies did not find significant associations [16, 17, 19].
A history of abortion was evaluated in two studies, both of which found significant associations with increased mortality. A history of at least one abortion was associated with a 3-fold increase in infant mortality [21]. One abortion was associated with an increase in under-five mortality (OR=2.20), while multiple abortions did not show additional risk in the same study [22].
The number of pregnancies/deliveries was assessed in 5 studies. First parity (OR=1.53) [14] and higher parity, especially third (OR=11.25) and fourth pregnancies (OR=25), were associated with significantly increased infant mortality in some studies [20], though not all findings were statistically significant [16, 17, 19, 20].
Method of delivery (e.g. cesarean section) was not associated with mortality in any of the 3 studies that evaluated this factor [16, 19, 21].
High-risk pregnancies did not show significant associations with child mortality across the three studies that assessed them [16-18].
Maternal physical health during pregnancy was evaluated in 6 studies. Conditions such as dental issues (OR=2.49) and hypertension (OR=1.62) were significantly associated with increased infant mortality [14]. However, other conditions, including anemia [14], gestational weight gain [22], and gestational diabetes [14, 21], were not consistently significant. Antenatal care was also a critical factor; fewer than four visits during pregnancy increased mortality by over 15 times in one study [21], whereas more frequent care was associated with reduced child mortality (1-59 months) by 15% [18], though not all findings were statistically significant [16, 19].
Discussion
This systematic review aimed to identify and synthesize the risk factors associated with mortality among children aged 1 to 59 months in Iran, and identified a wide range of modifiable risk factors. Key findings highlighted the significant roles of LBW (<2500 g), low maternal education, lack of breastfeeding, and higher parity in increasing child mortality. The risk factors clustered into three domains: Socioeconomic, child-related, and maternal/pregnancy-related. Each domain contributes uniquely to child mortality, underscoring the multifactorial nature of under-five deaths. Among the three domains of risk factors, child-related factors emerged as the most influential. The findings are discussed below in the same framework used for the results.
Socioeconomic risk factors
Among the socioeconomic determinants, maternal education emerged as a consistently protective factor, consistent with the global literature linking higher maternal education to better health-seeking behavior, improved child care practices, and greater autonomy in accessing health services [3, 23, 24]. Its importance likely stems from the role of maternal knowledge in improving child care and hygiene practices, nutrition, immunization, and access to health services [14, 25]. Each additional year of maternal education reduced under-5 mortality by 3% [23]. UNICEF has identified low maternal education as a global determinant of under-5 mortality [3]. In Iran, although the female literacy rate (ages 15-24] exceeded 98.93% in 2022, regional disparities persist (42-98.93%), especially in rural and underserved provinces [26]. Provinces such as Sistan and Baluchestan report young female literacy rates as low as 69%, compared to nearly 100% in Semnan province [27]. Therefore, enhancing access to education for adolescent girls and mothers through targeted interventions could contribute meaningfully to reducing child mortality.
Although 4 studies included in this review found no significant association between paternal education and under-5 child mortality, this finding should be interpreted with caution. One possible explanation is the study design of the included studies, which were not cohort studies, making it difficult to establish a strong causal relationship. Future research should further investigate these mediating factors to clarify the role of paternal education in child survival in Iran. However, in another study, children whose fathers had completed 12 years of schooling experienced 17% lower under-5 mortality compared to those with illiterate fathers [23]. The influence of paternal education may also be reflected in income, as demonstrated in another study that found fathers’ education and family income were important indicators of the resources available to ensure their children’s health and safety [1]. Therefore, expanding access to secondary and tertiary education for girls, especially in rural and low-income communities, can yield long-term health dividends [28, 29].
Low socioeconomic status was another robust predictor of child mortality, with all studies reporting significant associations. This finding aligns with the literature, which shows that poverty limits access to nutrition, clean water, and healthcare, thereby increasing vulnerability to preventable diseases [3, 24]. Generally, children born in high-income countries face considerably lower mortality risks [3]. In Iran, although significant strides have been made in expanding health coverage, income inequality remains a major barrier to equity in child health outcomes [30-32]. Policymakers should expand poverty alleviation programs, such as conditional cash transfers, nutritional assistance, and reductions in out-of-pocket health expenditures through free child health services, in lower-income communities to mitigate structural disadvantage [33, 34].
As another socioeconomic risk factor, paternal substance abuse increased the risk of child mortality by more than two-fold, possibly due to reduced household income and caregiving capacity [35]. However, maternal smoking did not show a consistent or significant effect, aligning with some previous studies but contrasting with others that have found significant associations in different contexts [24, 36-38]. Integrated addiction prevention and treatment services and family support programs should be scaled up, particularly in provinces with high substance use prevalence [39, 40].
Meanwhile, first-cousin marriages significantly increased child mortality, likely due to genetic disorders and congenital anomalies [41]. Iran has one of the highest rates of consanguinity globally, estimated at 30% in some regions [42]. Premarital genetic counseling and community-based education programs could help mitigate this risk while respecting cultural norms [16].
Interestingly, parental employment and occupation were not significantly associated with child mortality. This result might be due to regional homogeneity. Most studies were conducted in rural settings where occupational variation is minimal. However, one study found that maternal employment reduced under-5 mortality, possibly because it was associated with higher levels of education and awareness among employed mothers [14]. A study in Ethiopia revealed that unemployed parents had a 40% higher likelihood of under-5 child mortality compared to those who were employed [43]. Parental employment also had a positive impact on skilled delivery and the number of antenatal care visits [43].
Place of residence showed mixed results. Only 2 of the 6 studies examining the place of birth and residence reported significant associations. Home delivery and rural residence were associated with increased mortality in some cases but were not universally significant across studies, likely reflecting regional differences in healthcare access and delivery systems [24]. Limited geographic variability in the study samples might explain this result. Moreover, home delivery was reported in studies conducted in Sistan and Baluchestan Province [21]. So, these findings cannot be generalized to the entire country. Promoting childbirth in health facilities can help lower under-5 mortality rates [25]. In line with this, a study in India found that home deliveries were more common among illiterate mothers, and neonatal and infant mortality rates were also higher in this group [44]. Nonetheless, UNICEF has reported that rural residence increases the risk of under-5 mortality by 1.5 times [3], and a study in China found substantial provincial disparities ranging from 4 to 34 deaths per 1000 live births [45]. To address health disparities across geographic regions and urban and rural areas, access to primary healthcare services must be equitable and fair [24, 25, 46].
Findings of this review showed that a family size of fewer than 5 members increased under-5 child mortality by 2.5 times, while studies in other countries have reported the opposite. A study in Ethiopia showed that families with 3 to 6 children had higher under-5 mortality compared to those with only 1 or 2 children [47]. This discrepancy may be related to contextual factors such as parental education level, economic status, or the distribution of caregiving resources within the household [48]. In addition, smaller families might have limited caregiving experience or lower social support.
Psychological stress during pregnancy, including exposure to domestic violence and loss of close family members, was also significantly associated with increased child mortality. These findings underscore the broader maternal psychosocial context of child health [24]. Mental health screening during antenatal care (ANC) and referral pathways for psychosocial support are embedded within maternal health services in Iran [49]. Other studies also reported the impact of violence on pregnant women on child mortality [50-52].
Child-related risk factors
LBW was the most consistent and significant child-related risk factor across all studies. Children weighing less than 2500 g at birth had substantially elevated risks of mortality, with OR reaching 42 in some studies. Similarly, preterm birth, particularly before 34 weeks of gestation, was associated with substantially increased mortality risk [1]. These findings are consistent with global evidence that prematurity and LBW are leading causes of neonatal and post-neonatal mortality due to increased susceptibility to infections, hypothermia, and poor growth, as well as impaired neurodevelopment and non-communicable diseases [1, 16, 53, 54]. In Iran, the prevalence of prematurity is around 10%, but rates reach nearly 20% in some provinces [55]. In response, targeted prenatal nutrition programs, better management of maternal infections and pregnancy complications, and improved monitoring of fetal growth are essential to reducing the burden of prematurity and LBW and associated mortality [56].
Feeding practices also showed a strong association with survival. Exclusive breastfeeding significantly reduced the risk of death, while formula feeding or early introduction of other foods increased it. This finding aligns with World Health Organization (WHO) recommendations that exclusive breastfeeding for the first six months can prevent 13% of under-five deaths globally [57]. In Iran, exclusive breastfeeding rates have declined in recent years, mainly due to urbanization and marketing of formula milk [58]. Policy interventions may include promoting breastfeeding through baby-friendly hospital initiatives, maternity leave policies, and breastfeeding-friendly policies in workplaces and public spaces, especially targeting first-time and working mothers [48, 59].
No significant association was found between child sex and mortality in this study, which may reflect increasing gender equity in child care practices. With growing public awareness and maternal education, cultural preferences for one gender over the other are diminishing [19]. However, global data show that male children generally have higher under-5 mortality [60, 61], although the observed differences may be marginal in some regions [12].
While multiple births did not show significant associations with mortality in this review, incomplete vaccination did. Notably, infants with incomplete immunization had a 14-fold higher risk of death. Given Iran’s historically strong immunization coverage [62], this condition may reflect emerging gaps in access or awareness in marginalized populations [63]. Ensuring universal immunization through outreach in nomadic, rural, and informal urban settlements is vital, as is combating misinformation about vaccines.
Maternal and pregnancy-related risk factors
Among maternal factors, short interpregnancy intervals (especially <12 months) significantly elevated the risk of child mortality. This result may reflect maternal nutrient depletion [25] and inadequate recovery time between pregnancies [48], both of which compromise fetal development and caregiving capacity [64, 65]. So, a birth spacing of at least 2 years is recommended [24]. Health workers should counsel couples on optimal birth spacing and ensure access to family planning resources in both urban and rural areas [66, 67].
Maternal age and number of pregnancies had mixed associations; first-time pregnancies and advanced parity (third or higher) were linked with increased mortality in some studies. The increased risk in primigravida women may be related to inexperience and lower confidence in infant care, while high parity could signal cumulative maternal health burdens [24]. Earlier studies have indicated that maternal age below 18 is associated with increased risk of preterm birth and LBW [14]. Another study showed that children of older mothers may have better nutrition and education [68]. Thus, antenatal education programs should be tailored for both first-time mothers and those with high parity to address specific knowledge and health gaps.
Notably, high-risk pregnancy and cesarean delivery were not significantly associated with child mortality, suggesting that their effects may be mediated through other conditions, such as prematurity or birth complications, rather than acting as independent predictors.
However, poor maternal physical health, especially dental problems and hypertension during pregnancy, was significantly associated with increased mortality risk. Routine screening and management of maternal conditions, including non-obstetric issues like oral health, should be incorporated into prenatal protocols. Similarly, antenatal care (ANC) was a critical protective factor. Inadequate ANC (fewer than four visits) was associated with more than a 15-fold increase in child mortality, echoing WHO guidelines that emphasize early and frequent antenatal visits [69]. This finding emphasizes the life-saving role of comprehensive pregnancy monitoring [24]. Although Iran’s health system provides free ANC through its primary care network, service utilization varies. To improve the situation, universal, high-quality antenatal care coverage—especially for high-risk pregnancies—should be ensured through community health outreach and mobile clinics in underserved areas [69].
A history of abortion was another significant predictor of infant and under-five mortality in Iran. While this may reflect underlying maternal health risks or reproductive complications, it also underscores the need for post-abortion care and monitoring in subsequent pregnancies. The impact of abortion history on LBW and infection is reported in the literature, which contributes to child mortality [70]. Implications of this finding may be enhanced monitoring of women with previous abortions during prenatal care, and prioritizing them for early interventions can improve outcomes.
Conclusion
This systematic review identified a wide range of risk factors influencing child mortality in Iran, particularly among children aged 1 to 59 months. The most consistently significant determinants were modifiable and included maternal education, socioeconomic status, birth outcomes (such as LBW and prematurity), and healthcare-related factors, such as breastfeeding and antenatal care. The challenges identified in this review, including high consanguinity rates and significant urban-rural disparities in health outcomes, reflect conditions in many low- and middle-income countries. Therefore, the findings have broader relevance and can inform child survival strategies in similar contexts. Moreover, addressing the modifiable risk factors outlined here contributes directly to achieving sustainable development goal 3.2, which aims to reduce under-5 mortality to at least 25 deaths per 1000 live births by 2030.
Strengths and limitations
This review is the first to systematically synthesize evidence on mortality risk factors among children aged 1 to 59 months in Iran, addressing a critical gap in national child health research. It followed preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines, applied rigorous quality assessment using the Newcastle-Ottawa scale, and included both Persian and English sources for broad coverage. Organizing findings into socioeconomic, maternal, and child-related domains enhanced clarity for policy use.
However, the study has limitations. The number of eligible studies for each particular risk factor was small, and heterogeneity in designs and variable definitions limited comparability and precluded meta-analysis. All included studies were observational, restricting causal inference. Additionally, potential publication bias and the exclusion of gray literature may have led to the omission of relevant data. Most studies were conducted in only a few regions, particularly Shahroud, which may limit generalizability. More regionally diverse, methodologically rigorous studies are needed to clarify causal pathways further and inform targeted interventions.
Policy implications
Based on these findings, we recommend integrating maternal literacy programs into Iran’s primary healthcare system, prioritizing provinces with low female literacy rates. Enhancing baby-friendly hospital initiatives and promoting breastfeeding-friendly workplace policies can help increase exclusive breastfeeding rates. Expanding poverty alleviation efforts, such as conditional cash transfers and nutritional support targeted at low-income families, is essential. Effective implementation of these multifaceted strategies requires coordination among the Ministry of Health, the Ministry of Education, and Social Welfare organizations. Health policymakers should consider regional disparities when designing interventions and prioritize high-risk populations identified in this review.
Future research should aim to increase geographic and methodological diversity by including more provinces and employing longitudinal cohort studies. Investigating the impacts of emerging factors such as climate change, conflict, and migration on child mortality is essential. Furthermore, studies focused on the implementation, uptake, and scalability of interventions targeting maternal education, breastfeeding promotion, and poverty reduction will be critical for informing effective health policies.
This systematic review identified several modifiable risk factors associated with child mortality in Iran, many of which align with global findings. To advance child survival efforts, future studies should employ longitudinal designs and incorporate underexplored determinants. Additionally, implementation research evaluating the effectiveness of targeted interventions in diverse Iranian settings is needed to guide policy.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.REC.1400.137).
Funding
This study was extracted from the PhD dissertation of Leila Abdollahi Abed, approved by the Department of Health Services Management, School of Health Management and Information Sciences, Iran University of Medical Sciences, Tehran, Iran. This study was financially supported by Iran University of Medical Sciences, Tehran, Iran (Project No.: 19904-37-1-0).
Authors contributions
Conceptualisation and study design: Soudabeh Vatankhah and Leila Abdollahi Abed; Supervision: Soudabeh Vatankhah; Data collection and process: Azam Choopani, Leila Abdollahi Abed; Data analysis and interpretation: Azam Choopani and Leila Abdollahi Abed; Investigation and writing the original draft: Leila Abdollahi Abed; Review and editing: Soudabeh Vatankhah and Azam Choopani; Final approval: All authors.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank Iran University of Medical Sciences, Tehran, Iran, for providing the facilities for this research.
References
Child mortality is widely recognized as a key indicator of population health, social welfare, and national development [1]. It was identified as one of the millennium development goals to reduce the child mortality rate by two-thirds between 1990 and 2015 [1]. The sustainable development goals further emphasize the importance of eliminating all preventable deaths among children under 5 years of age, aiming to reduce their mortality rate to no more than 25 per 1,000 live births by 2030 [2]. According to United Nations Children's Fund (UNICEF), children aged 1 to 59 months account for more than half of 4.8 million under-5 deaths globally, with pneumonia, diarrhea, and malaria as leading causes in 2023 [3]. While global child mortality has declined—from 77 per 1,000 in 2000 to 37 in 2023—disparities remain stark, particularly in low- and middle-income countries [3]. In high-income countries, this rate is as low as 5 per 1000 live births, whereas in low-income countries, child mortality is 13 times higher than in high-income nations [2]. Child mortality is not evenly distributed across the globe; 1.08 million of these deaths occurred in sub-Saharan Africa and South Asia alone [2].
These deaths are largely preventable and are strongly associated with social determinants such as limited access to health care, poor nutrition, unsafe water, inadequate sanitation, and maternal education [2, 3]. In many countries, child mortality is also influenced by structural inequalities and regional disparities in health service coverage [4]. Globally, well-documented risk factors include maternal age, birth spacing, family income, household education, and rural residence [3].
In Iran, the under-5 mortality rate has declined from earlier decades to 11.7 per 1000 live births in 2023 [5]. A substantial proportion of under-5 deaths in Iran occur among infants under one year of age [6]. Injuries have been identified as the leading cause of death among children aged 1 to 59 months in Iran, affecting both genders equally, though with varying distribution across provinces [4]. Globally, unintentional injuries are among the most prominent causes of child mortality, a trend also confirmed by studies conducted in Iran [7-10]. Poverty stands out as a major social determinant of child health, and poverty reduction programs have been linked to decreases in under-5 mortality in numerous countries [11]. The health and survival of children under 5 are also closely linked to the socioeconomic conditions of their families, with higher mortality rates observed in lower socioeconomic strata [12].
Within the Iranian health system, child health is administratively separated into neonates (0–28 days) and older children (1–59 months), with each managed by distinct departments within the Ministry of Health and Medical Education. While risk factors associated with neonatal mortality in Iran have been specifically addressed in a separate study [13], risk factors affecting children aged 1 to 59 months have received less consolidated attention, and existing research remains fragmented, with a comprehensive synthesis of risk factors specific to the post-neonatal period lacking. Thus, this study investigated the risk factors of children aged 1 to 59 months. Given that under-5 mortality is a multifactorial outcome encompassing the child, the mother, and pregnancy-related events [14], a systematic understanding of these contributors is critical for designing targeted and effective, evidence-based interventions to reduce child mortality. This study aimed to systematically review and synthesize the available evidence on risk factors for mortality among children aged 1 to 59 months in Iran.
Materials and Methods
This study was designed as a systematic review employing a narrative synthesis approach—all stages of the research and its reporting adhered to the PRISMA 2020 checklist. The timeframe for included studies was set to 2010-2023 to reflect the current situation better. The literature search was conducted in October 2023.
Given that Persian is the official language of Iran, Persian-language studies were included alongside English-language articles published in international journals. Search was conducted in Persian databases, including Iranian Research Institute for Information Science and Technology (IranDoc) and Scientific Information Database (SID), and in international databases of ScienceDirect, PubMed, and ISI Web of Science, using a combination of keywords for “child mortality,” “child*,” “infant,” “under five,” “under-5,” “U5M,” “mortalit*,” “death,” and “Iran*” and their Persian equivalents. Search strategy used for PubMed is presented here as an example: (((child*[Title/Abstract] OR infant[Title/Abstract] OR U5M[Title/Abstract] OR “under five” [Title/Abstract] OR “under 5”[Title/Abstract]) AND (mortalit*[Title/Abstract] OR death* [Title/Abstract]) AND (Iran*[Title/Abstract])) OR ((“child mortality”[Mesh] OR “infant mortality”[Mesh]) AND “Iran”[Mesh])) AND (2010:2024[pdat]). Search strategies used for other databases are provided in the supplementary file. Additionally, Google Scholar citation check was used to identify potentially relevant studies. The reference lists of the included articles were manually reviewed for additional sources.
A highly sensitive search strategy was employed. Although this strategy resulted in the retrieval of some irrelevant material, efforts were made to screen and assess all potentially relevant articles. This search strategy was refined through multiple iterations of keyword combinations to capture the broadest possible range of literature on under-5 mortality risk factors.
The inclusion criteria for the study stipulated that the article must focus on mortality in children aged 1 to 59 months or under 5 years; be conducted within Iran or in one or more of its cities, provinces, or hospitals; utilize multivariate regression to analyze risk factors; report odds ratios (OR); and be published in either Persian or English. On the other hand, studies were excluded if they focused on a specific disease or a particular subgroup of children, examined deaths from a single cause, lacked full text, included stillbirths in under-5 mortality figures, or were duplicate publications from the same dataset.
The study population comprised all articles, theses, and reports related to mortality among children aged 1 to 59 months in Iran. In line with the aforementioned categorization, articles covering mortality in children under 1 year, under 5 years, and specifically aged 1 to 59 months were included. No restrictions were placed on study type, and all study designs, including cohort and case-control studies that reported OR, could have been included in the review.
All retrieved articles were stored and managed using EndNote software, version X20. Data extraction was carried out using a pre-designed table containing two sections: General and specific information. General information included the year of publication, author, and study location. Specific information included study period, objectives, study design, age group studied, data collection tools and methods, sample size, statistical analysis techniques, significant and non-significant findings, and reported limitations. Two researchers performed data extraction from the articles. In the event of any disagreement, the issue was resolved by a third party.
Ultimately, 6 case-control studies and 3 cross-sectional studies met the inclusion criteria. To assess their quality, the Newcastle-Ottawa scale was employed, following evidence from a systematic review and meta-analysis evaluating quality assessment tools [15]. This tool provides separate checklists for case-control and cross-sectional studies, with a maximum score of nine stars. Studies scoring 7 or higher were categorized as high-quality. All included studies in this review were assessed and determined to be of high quality (Table 1).
Heterogeneity assessment
Given the considerable heterogeneity among the included studies, conducting a meta-analysis was deemed inappropriate. This heterogeneity arose from several factors, including differences in target populations (e.g. age groups, geographic locations), variations in the classification and definition of risk factors, and diverse methods for outcome measurement. These discrepancies limited the comparability of study findings and posed significant challenges for synthesizing data quantitatively.
Moreover, the number of studies available for each specific risk factor was relatively small (fewer than 9 in most cases), which further constrained the statistical power and reliability of any pooled analysis. Due to these qualitative and quantitative limitations, a formal heterogeneity assessment (e.g. I2 statistic) and meta-analysis were not performed. Instead, a narrative synthesis approach was adopted to summarize and interpret the findings descriptively.
Results
Out of 2886 articles initially retrieved, 9 studies met the inclusion criteria and were included in this systematic review. The process of article selection and exclusion at each stage is illustrated in Figure 1.
The included studies identified a wide range of risk factors associated with child mortality, grouped into three domains: Socioeconomic factors, maternal and pregnancy-related factors, and child-related factors. These were analyzed based on statistical significance and the age group studied. Table 5 lists the child mortality investigated in the included studies in Iran.
Socioeconomic risk factors
This category comprised 9 specific risk factors, with a total frequency of 33 instances across studies, of which 16(48%) were statistically significant.
Among socioeconomic variables, maternal education was one of the most frequently reported and influential factors. In 6 studies, higher maternal education was significantly associated with lower child mortality. Higher years of maternal education were significantly associated with reduced mortality among children under 1 year (OR=0.92) [16]. For instance, university-level and high school education reduced infant mortality by 60% and 55%, respectively [14]. Additionally, mothers with no formal education or only primary education had more than double the odds of under-five child mortality (OR=2.20) [12]. However, in four studies, primary and middle school education levels did not show significant associations with mortality [14, 17-19].
In contrast, paternal education was not significantly associated with child mortality in any of the four studies that evaluated this factor [12, 16, 18, 19].
Low socioeconomic status consistently emerged as a strong risk factor. All three studies examining this variable reported significant associations, with increased odds of child mortality [16, 20], particularly in children under 5 (OR=7.80) [12].
Smoking and substance abuse by parents were evaluated in two studies. While maternal smoking did not show a significant association [14], paternal addiction increased the risk of under-5 mortality by 2.6 times [12].
Parental employment status, including maternal employment and occupation type (e.g. laborer or civil servant), was examined in four studies. None of them reported significant associations with mortality [14, 16, 17, 19].
The place of residence and the delivery location were investigated in 6 studies. Home delivery was significantly associated with increased infant mortality by 5.8 times in Zahedan City, Iran [21], but not in other cities [18], while living in rural areas was a risk factor for under-5 mortality (OR=1.79) [22], but not in all studies investigated [14, 16]. Out-of-hospital delivery was examined in one study, which found no significant effect [19].
Family size showed mixed results. One study found that smaller families (less than 5 members) had higher under-5 mortality rates (OR=2.60) [12], whereas others found no significant associations [19, 22].
Consanguineous marriage was identified as a risk factor in three studies. First-cousin marriage significantly increased mortality risk with OR of 1.44 [14], 2.37 [16], and 3.92 [22], while marriages among more distant relatives did not show significant effects [22].
Psychological stress during pregnancy, specifically domestic violence, tripled the risk of under-five mortality [22], and loss of a family member during pregnancy increased infant mortality by 1.6 times [14]. However, general psychological symptoms during pregnancy did not show significant associations [14].
Child-related risk factors
This domain included 7 subcategories, totaling 25 instances, of which 17(68%) were statistically significant.
Gestational age at birth was assessed in 4 studies. Preterm birth, especially before 34 weeks, significantly increased the risk of mortality among children aged 1 to 59 months by 5 times [19]. Each additional week of gestation was associated with a 15% reduction in under-five mortality [22]. However, not all studies found statistically significant results for infants born at less than 37 weeks [21], but one did, showing a significant association with increased infant mortality (OR=3.50) [17].
Low birth weight (LBW) (<2500 g) was the most consistent and significant risk factor, with all seven studies reporting strong associations with increased mortality. [14, 16-19, 21, 22]. Each additional kilogram of birth weight was associated with an approximate 64% reduction in under-5 mortality [22]. LBW significantly increased child mortality with OR ranging from 2.83 [16] to 42.10 [21]. In contrast, high birth weight (>4000 g) did not show significant effects [14].
Feeding practices were evaluated in four studies. Exclusive breastfeeding reduced mortality among children aged 1 to 59 months [18], while the use of formula or other substitutes increased the risk by more than two [16] and four times in infant mortality [21].
The sex of the child did not show any significant association with mortality in any of the 4 studies that examined this variable [14, 16, 19, 21].
Healthcare access was evaluated in two studies. Incomplete vaccination was associated with a 14.9-fold increase in infant mortality in one study [21], while general child care access did not show consistent effects [19].
Abnormal physical growth and congenital anomalies were examined in three studies. One study found that abnormal growth was significantly associated with higher mortality among children aged 1-59 months (OR=7) [19], whereas another did not [18]. Congenital anomalies increased the risk of mortality among children under one year by 11.80 times [20].
Multiple births (e.g. twins) were not significantly associated with increased mortality [14].
Maternal and pregnancy-related risk factors
This group included 7 specific factors, with 30 mentions across studies, of which 11(36%) were statistically significant.
Short interpregnancy intervals were evaluated in 5 studies [14, 16, 17, 19, 22]. An interval of less than 1 year (OR=2.70) and 1 to 3 years (OR=1.40) was associated with increased infant mortality [14]. However, in another study, intervals of less than three years were not consistently statistically significant among children aged 1-59 months [19].
Maternal age was examined in 4 studies. Only one significant finding was reported: Mothers aged 18–35 had lower infant mortality than those younger than 18 or older than 35 [14]. Other studies did not find significant associations [16, 17, 19].
A history of abortion was evaluated in two studies, both of which found significant associations with increased mortality. A history of at least one abortion was associated with a 3-fold increase in infant mortality [21]. One abortion was associated with an increase in under-five mortality (OR=2.20), while multiple abortions did not show additional risk in the same study [22].
The number of pregnancies/deliveries was assessed in 5 studies. First parity (OR=1.53) [14] and higher parity, especially third (OR=11.25) and fourth pregnancies (OR=25), were associated with significantly increased infant mortality in some studies [20], though not all findings were statistically significant [16, 17, 19, 20].
Method of delivery (e.g. cesarean section) was not associated with mortality in any of the 3 studies that evaluated this factor [16, 19, 21].
High-risk pregnancies did not show significant associations with child mortality across the three studies that assessed them [16-18].
Maternal physical health during pregnancy was evaluated in 6 studies. Conditions such as dental issues (OR=2.49) and hypertension (OR=1.62) were significantly associated with increased infant mortality [14]. However, other conditions, including anemia [14], gestational weight gain [22], and gestational diabetes [14, 21], were not consistently significant. Antenatal care was also a critical factor; fewer than four visits during pregnancy increased mortality by over 15 times in one study [21], whereas more frequent care was associated with reduced child mortality (1-59 months) by 15% [18], though not all findings were statistically significant [16, 19].
Discussion
This systematic review aimed to identify and synthesize the risk factors associated with mortality among children aged 1 to 59 months in Iran, and identified a wide range of modifiable risk factors. Key findings highlighted the significant roles of LBW (<2500 g), low maternal education, lack of breastfeeding, and higher parity in increasing child mortality. The risk factors clustered into three domains: Socioeconomic, child-related, and maternal/pregnancy-related. Each domain contributes uniquely to child mortality, underscoring the multifactorial nature of under-five deaths. Among the three domains of risk factors, child-related factors emerged as the most influential. The findings are discussed below in the same framework used for the results.
Socioeconomic risk factors
Among the socioeconomic determinants, maternal education emerged as a consistently protective factor, consistent with the global literature linking higher maternal education to better health-seeking behavior, improved child care practices, and greater autonomy in accessing health services [3, 23, 24]. Its importance likely stems from the role of maternal knowledge in improving child care and hygiene practices, nutrition, immunization, and access to health services [14, 25]. Each additional year of maternal education reduced under-5 mortality by 3% [23]. UNICEF has identified low maternal education as a global determinant of under-5 mortality [3]. In Iran, although the female literacy rate (ages 15-24] exceeded 98.93% in 2022, regional disparities persist (42-98.93%), especially in rural and underserved provinces [26]. Provinces such as Sistan and Baluchestan report young female literacy rates as low as 69%, compared to nearly 100% in Semnan province [27]. Therefore, enhancing access to education for adolescent girls and mothers through targeted interventions could contribute meaningfully to reducing child mortality.
Although 4 studies included in this review found no significant association between paternal education and under-5 child mortality, this finding should be interpreted with caution. One possible explanation is the study design of the included studies, which were not cohort studies, making it difficult to establish a strong causal relationship. Future research should further investigate these mediating factors to clarify the role of paternal education in child survival in Iran. However, in another study, children whose fathers had completed 12 years of schooling experienced 17% lower under-5 mortality compared to those with illiterate fathers [23]. The influence of paternal education may also be reflected in income, as demonstrated in another study that found fathers’ education and family income were important indicators of the resources available to ensure their children’s health and safety [1]. Therefore, expanding access to secondary and tertiary education for girls, especially in rural and low-income communities, can yield long-term health dividends [28, 29].
Low socioeconomic status was another robust predictor of child mortality, with all studies reporting significant associations. This finding aligns with the literature, which shows that poverty limits access to nutrition, clean water, and healthcare, thereby increasing vulnerability to preventable diseases [3, 24]. Generally, children born in high-income countries face considerably lower mortality risks [3]. In Iran, although significant strides have been made in expanding health coverage, income inequality remains a major barrier to equity in child health outcomes [30-32]. Policymakers should expand poverty alleviation programs, such as conditional cash transfers, nutritional assistance, and reductions in out-of-pocket health expenditures through free child health services, in lower-income communities to mitigate structural disadvantage [33, 34].
As another socioeconomic risk factor, paternal substance abuse increased the risk of child mortality by more than two-fold, possibly due to reduced household income and caregiving capacity [35]. However, maternal smoking did not show a consistent or significant effect, aligning with some previous studies but contrasting with others that have found significant associations in different contexts [24, 36-38]. Integrated addiction prevention and treatment services and family support programs should be scaled up, particularly in provinces with high substance use prevalence [39, 40].
Meanwhile, first-cousin marriages significantly increased child mortality, likely due to genetic disorders and congenital anomalies [41]. Iran has one of the highest rates of consanguinity globally, estimated at 30% in some regions [42]. Premarital genetic counseling and community-based education programs could help mitigate this risk while respecting cultural norms [16].
Interestingly, parental employment and occupation were not significantly associated with child mortality. This result might be due to regional homogeneity. Most studies were conducted in rural settings where occupational variation is minimal. However, one study found that maternal employment reduced under-5 mortality, possibly because it was associated with higher levels of education and awareness among employed mothers [14]. A study in Ethiopia revealed that unemployed parents had a 40% higher likelihood of under-5 child mortality compared to those who were employed [43]. Parental employment also had a positive impact on skilled delivery and the number of antenatal care visits [43].
Place of residence showed mixed results. Only 2 of the 6 studies examining the place of birth and residence reported significant associations. Home delivery and rural residence were associated with increased mortality in some cases but were not universally significant across studies, likely reflecting regional differences in healthcare access and delivery systems [24]. Limited geographic variability in the study samples might explain this result. Moreover, home delivery was reported in studies conducted in Sistan and Baluchestan Province [21]. So, these findings cannot be generalized to the entire country. Promoting childbirth in health facilities can help lower under-5 mortality rates [25]. In line with this, a study in India found that home deliveries were more common among illiterate mothers, and neonatal and infant mortality rates were also higher in this group [44]. Nonetheless, UNICEF has reported that rural residence increases the risk of under-5 mortality by 1.5 times [3], and a study in China found substantial provincial disparities ranging from 4 to 34 deaths per 1000 live births [45]. To address health disparities across geographic regions and urban and rural areas, access to primary healthcare services must be equitable and fair [24, 25, 46].
Findings of this review showed that a family size of fewer than 5 members increased under-5 child mortality by 2.5 times, while studies in other countries have reported the opposite. A study in Ethiopia showed that families with 3 to 6 children had higher under-5 mortality compared to those with only 1 or 2 children [47]. This discrepancy may be related to contextual factors such as parental education level, economic status, or the distribution of caregiving resources within the household [48]. In addition, smaller families might have limited caregiving experience or lower social support.
Psychological stress during pregnancy, including exposure to domestic violence and loss of close family members, was also significantly associated with increased child mortality. These findings underscore the broader maternal psychosocial context of child health [24]. Mental health screening during antenatal care (ANC) and referral pathways for psychosocial support are embedded within maternal health services in Iran [49]. Other studies also reported the impact of violence on pregnant women on child mortality [50-52].
Child-related risk factors
LBW was the most consistent and significant child-related risk factor across all studies. Children weighing less than 2500 g at birth had substantially elevated risks of mortality, with OR reaching 42 in some studies. Similarly, preterm birth, particularly before 34 weeks of gestation, was associated with substantially increased mortality risk [1]. These findings are consistent with global evidence that prematurity and LBW are leading causes of neonatal and post-neonatal mortality due to increased susceptibility to infections, hypothermia, and poor growth, as well as impaired neurodevelopment and non-communicable diseases [1, 16, 53, 54]. In Iran, the prevalence of prematurity is around 10%, but rates reach nearly 20% in some provinces [55]. In response, targeted prenatal nutrition programs, better management of maternal infections and pregnancy complications, and improved monitoring of fetal growth are essential to reducing the burden of prematurity and LBW and associated mortality [56].
Feeding practices also showed a strong association with survival. Exclusive breastfeeding significantly reduced the risk of death, while formula feeding or early introduction of other foods increased it. This finding aligns with World Health Organization (WHO) recommendations that exclusive breastfeeding for the first six months can prevent 13% of under-five deaths globally [57]. In Iran, exclusive breastfeeding rates have declined in recent years, mainly due to urbanization and marketing of formula milk [58]. Policy interventions may include promoting breastfeeding through baby-friendly hospital initiatives, maternity leave policies, and breastfeeding-friendly policies in workplaces and public spaces, especially targeting first-time and working mothers [48, 59].
No significant association was found between child sex and mortality in this study, which may reflect increasing gender equity in child care practices. With growing public awareness and maternal education, cultural preferences for one gender over the other are diminishing [19]. However, global data show that male children generally have higher under-5 mortality [60, 61], although the observed differences may be marginal in some regions [12].
While multiple births did not show significant associations with mortality in this review, incomplete vaccination did. Notably, infants with incomplete immunization had a 14-fold higher risk of death. Given Iran’s historically strong immunization coverage [62], this condition may reflect emerging gaps in access or awareness in marginalized populations [63]. Ensuring universal immunization through outreach in nomadic, rural, and informal urban settlements is vital, as is combating misinformation about vaccines.
Maternal and pregnancy-related risk factors
Among maternal factors, short interpregnancy intervals (especially <12 months) significantly elevated the risk of child mortality. This result may reflect maternal nutrient depletion [25] and inadequate recovery time between pregnancies [48], both of which compromise fetal development and caregiving capacity [64, 65]. So, a birth spacing of at least 2 years is recommended [24]. Health workers should counsel couples on optimal birth spacing and ensure access to family planning resources in both urban and rural areas [66, 67].
Maternal age and number of pregnancies had mixed associations; first-time pregnancies and advanced parity (third or higher) were linked with increased mortality in some studies. The increased risk in primigravida women may be related to inexperience and lower confidence in infant care, while high parity could signal cumulative maternal health burdens [24]. Earlier studies have indicated that maternal age below 18 is associated with increased risk of preterm birth and LBW [14]. Another study showed that children of older mothers may have better nutrition and education [68]. Thus, antenatal education programs should be tailored for both first-time mothers and those with high parity to address specific knowledge and health gaps.
Notably, high-risk pregnancy and cesarean delivery were not significantly associated with child mortality, suggesting that their effects may be mediated through other conditions, such as prematurity or birth complications, rather than acting as independent predictors.
However, poor maternal physical health, especially dental problems and hypertension during pregnancy, was significantly associated with increased mortality risk. Routine screening and management of maternal conditions, including non-obstetric issues like oral health, should be incorporated into prenatal protocols. Similarly, antenatal care (ANC) was a critical protective factor. Inadequate ANC (fewer than four visits) was associated with more than a 15-fold increase in child mortality, echoing WHO guidelines that emphasize early and frequent antenatal visits [69]. This finding emphasizes the life-saving role of comprehensive pregnancy monitoring [24]. Although Iran’s health system provides free ANC through its primary care network, service utilization varies. To improve the situation, universal, high-quality antenatal care coverage—especially for high-risk pregnancies—should be ensured through community health outreach and mobile clinics in underserved areas [69].
A history of abortion was another significant predictor of infant and under-five mortality in Iran. While this may reflect underlying maternal health risks or reproductive complications, it also underscores the need for post-abortion care and monitoring in subsequent pregnancies. The impact of abortion history on LBW and infection is reported in the literature, which contributes to child mortality [70]. Implications of this finding may be enhanced monitoring of women with previous abortions during prenatal care, and prioritizing them for early interventions can improve outcomes.
Conclusion
This systematic review identified a wide range of risk factors influencing child mortality in Iran, particularly among children aged 1 to 59 months. The most consistently significant determinants were modifiable and included maternal education, socioeconomic status, birth outcomes (such as LBW and prematurity), and healthcare-related factors, such as breastfeeding and antenatal care. The challenges identified in this review, including high consanguinity rates and significant urban-rural disparities in health outcomes, reflect conditions in many low- and middle-income countries. Therefore, the findings have broader relevance and can inform child survival strategies in similar contexts. Moreover, addressing the modifiable risk factors outlined here contributes directly to achieving sustainable development goal 3.2, which aims to reduce under-5 mortality to at least 25 deaths per 1000 live births by 2030.
Strengths and limitations
This review is the first to systematically synthesize evidence on mortality risk factors among children aged 1 to 59 months in Iran, addressing a critical gap in national child health research. It followed preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines, applied rigorous quality assessment using the Newcastle-Ottawa scale, and included both Persian and English sources for broad coverage. Organizing findings into socioeconomic, maternal, and child-related domains enhanced clarity for policy use.
However, the study has limitations. The number of eligible studies for each particular risk factor was small, and heterogeneity in designs and variable definitions limited comparability and precluded meta-analysis. All included studies were observational, restricting causal inference. Additionally, potential publication bias and the exclusion of gray literature may have led to the omission of relevant data. Most studies were conducted in only a few regions, particularly Shahroud, which may limit generalizability. More regionally diverse, methodologically rigorous studies are needed to clarify causal pathways further and inform targeted interventions.
Policy implications
Based on these findings, we recommend integrating maternal literacy programs into Iran’s primary healthcare system, prioritizing provinces with low female literacy rates. Enhancing baby-friendly hospital initiatives and promoting breastfeeding-friendly workplace policies can help increase exclusive breastfeeding rates. Expanding poverty alleviation efforts, such as conditional cash transfers and nutritional support targeted at low-income families, is essential. Effective implementation of these multifaceted strategies requires coordination among the Ministry of Health, the Ministry of Education, and Social Welfare organizations. Health policymakers should consider regional disparities when designing interventions and prioritize high-risk populations identified in this review.
Future research should aim to increase geographic and methodological diversity by including more provinces and employing longitudinal cohort studies. Investigating the impacts of emerging factors such as climate change, conflict, and migration on child mortality is essential. Furthermore, studies focused on the implementation, uptake, and scalability of interventions targeting maternal education, breastfeeding promotion, and poverty reduction will be critical for informing effective health policies.
This systematic review identified several modifiable risk factors associated with child mortality in Iran, many of which align with global findings. To advance child survival efforts, future studies should employ longitudinal designs and incorporate underexplored determinants. Additionally, implementation research evaluating the effectiveness of targeted interventions in diverse Iranian settings is needed to guide policy.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.REC.1400.137).
Funding
This study was extracted from the PhD dissertation of Leila Abdollahi Abed, approved by the Department of Health Services Management, School of Health Management and Information Sciences, Iran University of Medical Sciences, Tehran, Iran. This study was financially supported by Iran University of Medical Sciences, Tehran, Iran (Project No.: 19904-37-1-0).
Authors contributions
Conceptualisation and study design: Soudabeh Vatankhah and Leila Abdollahi Abed; Supervision: Soudabeh Vatankhah; Data collection and process: Azam Choopani, Leila Abdollahi Abed; Data analysis and interpretation: Azam Choopani and Leila Abdollahi Abed; Investigation and writing the original draft: Leila Abdollahi Abed; Review and editing: Soudabeh Vatankhah and Azam Choopani; Final approval: All authors.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank Iran University of Medical Sciences, Tehran, Iran, for providing the facilities for this research.
References
- Abbasi M, Tajvar M, Karami B. Determinants of under-five child mortality in Iran: A systematic review. 2021. preprint. [DOI:10.21203/rs.3.rs-948344/v1]
- UNICEF. Levels and trends in child mortality. New York: UNICEF; 2021. [Link]
- UNICEF, WHO. Levels and trends in child mortality-report 2024. New York: UNICEF; 2025. [Link]
- Motlagh ME, Kelishadi R, Barakati SH, Lornejad HR, Amiri M, Poursafa P. Distribution of mortality among 1 - 59 month-old children across Iranian provinces in 2009: The national mortality surveillance system. Arch Iran Med. 2013; 16(1):29-33. [PMID]
- UNICEF. Child mortality estimates [Internet]. 2025. [Updated 12 January 2026]. Available from: [Link]
- Shakeri MT, Yousefi R, Gholian Aval M, Salari M, Amini M, et al. [Age distribution, trends, and projections of under-5 mortality in Khorasan Razavi province: Time-Series Analyses (Persian)]. Iran J Epidemiol. 2021; 16(4):343-51. [Link]
- Izadi N, Shetabi HR, Bakhtiari S, Janatalmakan M, Parabi M, Ahmadi K. [The rate and causes of infant mortaliry in the hospitals of Kermanshah Province during 2011-2014 (Perian)]. J Rafsanjan Univ Med Sci. 2016; 15(2):129-38. [Link]
- Rahbar M, Ahmadi M, Lornejad H, Habibelahi A, Sanaei-Shoar T, Mesdeaghinia A. Mortality causes in children 1-59 Months in Iran. Iran J Public Health. 2013; 42(Supple1):93-7. [PMID]
- Azarbakhsh H, Rezaei F, Hamedi A, Hassanzadeh J, Razeghi A, Mirahmadizadeh A. Unintentional injuries in children in the south of Iran, 2004-2019: A trend analysis of mortality rates. BMJ Paediatr Open. 2023; 7(1):e002144. [DOI:10.1136/bmjpo-2023-002144] [PMID]
- Mohammadi G, Ghorbani R, Khosravifar S, Babakhanian M. Medical Causes of Death in Iranian Children Aged 1-59 Months: A systematic review and meta-analysis. J Pediatr Rev. 2024; 12(3):243-52. [DOI:10.32598/jpr.12.3.1207.1]
- Rasella D, Basu S, Hone T, Paes-Sousa R, Ocké-Reis CO, Millett C. Child morbidity and mortality associated with alternative policy responses to the economic crisis in Brazil: A nationwide microsimulation study. PLoS Med. 2018; 15(5):e1002570. [DOI:10.1371/journal.pmed.1002570] [PMID]
- Nakhzari-Moghaddam M, Yavari P, Abadi A, Rostami-Gooran N. Association of socioeconomic risk factors with under 5-year mortality in Zabol, Iran, during 2011-2015. Med J Islam Repub Iran. 2019; 33:61. [DOI:10.47176/mjiri.33.61] [PMID]
- Daemi A, Ravaghi H, Jafari M. Risk factors of neonatal mortality in Iran: A systematic review. Med J Islam Repub Iran. 2019; 33(1):528-34. [DOI:10.47176/mjiri.33.87]
- Hajipour M, Taherpour N, Fateh H, Yousefi E, Etemad K, Zolfizadeh F, et al. Predictive factors of infant mortality using data mining in Iran. J Compr Pediatr. 2021; 12(1). [DOI:10.5812/compreped.108575]
- Zeng X, Zhang Y, Kwong JS, Zhang C, Li S, Sun F, et al. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. J Evid Based Med. 2015; 8(1):2-10. [DOI:10.1111/j.1756-5391.2008.00003.x] [PMID]
- Damghanian M, Shariati M, Mirzaiinajmabadi K, Yunesian M, Emamian MH. Socioeconomic inequality and its determinants regarding infant mortality in iran. Iran Red Crescent Med J. 2014; 16(6):e17602. [DOI:10.5812/ircmj.17602] [PMID]
- Chaman R, Zolfaghari P, Sohrabi MB, Gholami Taramsari M, Amiri M. [Risk factors of infant mortality rate in north east of Iran (Persian)]. Hakim Res J. 2014; 17(2):96-101. [Link]
- Chaman R, Alami A, Emamian Mh, Naieni Kh, Mirmohammadkhani M, Ahmadnezhad E, et al. Important risk factors of mortality among children aged 1-59 months in rural areas of Shahroud, Iran: A community-based nested case-control study. Int J Prev Med. 2012; 3(12):875-9. [DOI:10.4103/2008-7802.104859] [PMID]
- Safari H, Nooripour S, Emadi Z, Shakeri R, Jandaghi J. Associated factors of mortality of children aged 1 to 59 months in rural areas of Semnan: A nested case-controlstudy based on 10 years of surveillance data. Koomesh. 2014; 15(3):282-8. [Link]
- Gholami Taramsar M, Moeini SR, Kazemipour S. Socioeconomic status and infant mortality rate. Int J Health Stud. 2021; 7(1):33-6. [Link]
- Ansari-Moghaddam A, Sadeghi-Bojd S, Imani M, Movahedinia S, Pourrashidi A, Mohammadi M. A multivariate analysis of factors associated with infant mortality in South-East of Iran. J Pak Med Assoc. 2014; 64(10):1123-6. [PMID]
- Evazpoor A, Edalati A, Hyppönen E, Fararouei M, Parisai Z. Deaths of children aged under 5 years and related factors in the Islamic Republic of Iran: A populationbased case-control study. East Mediterr Health J. 2016; 22(6):368-74. [DOI:10.26719/2016.22.6.368] [PMID]
- Balaj M, York HW, Sripada K, Besnier E, Vonen HD, Aravkin A, et al. Parental education and inequalities in child mortality: A global systematic review and meta-analysis. Lancet. 2021; 398(10300):608-20. [DOI:10.1016/S0140-6736(21)00534-1] [PMID]
- Faruk MO, Zahangir MS, Akhter S, Prome JF, Akter N, Tasnim J. A review of the impact of socioeconomic, demographic and cultural factors on child mortality. Discover Public Health. 2025; 22(1):141. [DOI:10.1186/s12982-025-00534-5]
- Geremew BM, Gelaye KA, Melesse AW, Akalu TY, Baraki AG. Factors affecting under-five mortality in Ethiopia: A multilevel negative binomial model. Pediatric Health Med Ther. 2020; 525-34. [DOI:10.2147/PHMT.S290715] [PMID]
- World Bank Group. Female literacy rate, ages 15-24. Washington: World Bank Group; 2025. [Link]
- Joulaei H, Maharlouei N, Lankarani KB, Razzaghi A, Akbari M. Narrative review of women’s health in Iran: challenges and successes. Int J Equity Health. 2016; 15(1):25. [DOI:10.1186/s12939-016-0316-x] [PMID]
- Mohammadi Y, Parsaeian M, Mehdipour P, Khosravi A, Larijani B, Sheidaei A, et al. Measuring Iran’s success in achieving millennium development goal 4: A systematic analysis of under-5 mortality at national and subnational levels from 1990 to 2015. Lancet Glob Health. 2017; 5(5):e537-e44. [DOI:10.1016/S2214-109X(17)30105-5] [PMID]
- Wu H. The effect of maternal education on child mortality in Bangladesh. Popul Dev Rev. 2022; 48(2):475-503. [DOI:10.1111/padr.12467]
- Pickett KE, Wilkinson RG. Income inequality and health: A causal review. Soc Sci Med. 2015; 128:316-26. [DOI:10.1016/j.socscimed.2014.12.031] [PMID]
- Olson ME, Diekema D, Elliott BA, Renier CM. Impact of income and income inequality on infant health outcomes in the United States. Pediatrics. 2010; 126(6):1165-73. [DOI:10.1542/peds.2009-3378] [PMID]
- Yang-Huang J, van Grieken A, You Y, Jaddoe VW, Steegers EA, Duijts L, et al. Changes in family poverty status and child health. Pediatrics. 2021; 147(4):e2020016717. [DOI:10.1542/peds.2020-016717] [PMID]
- Njuguna J. Impact of a Conditional Cash Transfer Program Aimed at Promoting Maternal and Child Health Services in Kakamega County, Kenya. J Health Care Poor Underserved. 2019; 30:329-38. [DOI:10.1353/hpu.2019.0024] [PMID]
- Meitei WB. The Synergy Between undernutrition and under-five mortality in India: A spatially explicit structural equation modelling approach. Spat Demogr. 2025; 13(1):2. [DOI:10.1007/s40980-024-00135-x]
- Mancheri H, Alavi M, Sabzi Z, Maghsoudi J. The effects of addiction on children and women: A qualitative study. Int J Pediatr Mashhad. 2020; 8(10):12165-76. [Link]
- Anderson TM, Lavista Ferres JM, Ren SY, Moon RY, Goldstein RD, Ramirez JM, et al. Maternal smoking before and during pregnancy and the risk of sudden unexpected infant death. Pediatrics. 2019; 143(4). [DOI:10.1542/peds.2018-3325] [PMID]
- Andriani H, Putri S, Kosasih RI, Kuo HW. Parental Smoking and Under-Five Child Mortality in Southeast Asia: Evidence from Demographic and Health Surveys. Int J Environ Res Public Health. 2019; 16(23):4756. [DOI:10.3390/ijerph16234756] [PMID]
- Sun J, Liu X, Zhao M, Magnussen CG, Xi B. Dose-response association between maternal smoking during pregnancy and the risk of infant death: A nationwide, population-based, retrospective cohort study. EClinicalMedicine. 2023; 57:101858. [DOI:10.1016/j.eclinm.2023.101858] [PMID]
- Rahmati A, Zeraat Herfeh F, Hosseini SO. Effective factors in first drug use experience among male and female addicts: A qualitative study. Int J High Risk Behav Addict. 2018; 7(4):1-8. [DOI:10.5812/ijhrba.66547]
- Mardani M, Alipour F, Rafiey H, Fallahi-Khoshknab M, Arshi M. Challenges in addiction-affected families: A systematic review of qualitative studies. BMC Psychiatry. 2023; 23(1):439. [DOI:10.1186/s12888-023-04927-1] [PMID]
- Khayat AM, Alshareef BG, Alharbi SF, AlZahrani MM, Alshangity BA, Tashkandi NF. Consanguineous Marriage and Its Association With Genetic Disorders in Saudi Arabia: A Review. Cureus. 2024; 16(2):e53888. [DOI:10.7759/cureus.53888]
- Mahdieh N. Consanguineous Marriages and Common Mutations in Iran: Two Key Points to Consider. J Adv Med Biomed Res. 2024; 32(153). [Link]
- Liranso E, Yang F. The influence of parental occupational status on under-five mortality in Ethiopia. Biodemography Soc Biol. 2024; 69(3):163-82. [DOI:10.1080/19485565.2024.2376568] [PMID]
- Das U, Chaplot B, Azamathulla HM. The role of place of delivery in preventing neonatal and infant mortality rate in India. Geographies. 2021; 1(1):47-62. [DOI:10.3390/geographies1010004]
- Song P, Theodoratou E, Li X, Liu L, Chu Y, Black RE, et al. Causes of death in children younger than five years in China in 2015: An updated analysis. J Glob Health. 2016; 6(2):020802. [DOI:10.7189/jogh.06.020802] [PMID]
- Gardiner FW, Bishop L, de Graaf B, Campbell J, Gale L, Quinlan F. Equitable patient access to primary healthcare in Australia. Canberra: The Royal Flying Doctor Service of Australia. 2020. [Link]
- Ekholuenetale M, Wegbom AI, Tudeme G, Onikan A. Household factors associated with infant and under-five mortality in sub-Saharan Africa countries. Int J Child Care Educ Policy. 2020; 14(1):10. [DOI:10.1186/s40723-020-00075-1]
- Ahmed Z, Kamal A, Kamal A. Statistical analysis of factors affecting child mortality in Pakistan. J Coll Physicians Surg Pak. 2016; 26(6):543-4. [PMID]
- Kharaghani R, Shariati M, Yunesian M, Keramat A, Moghisi A. The Iranian integrated maternal health care guideline based on evidence-based medicine and American guidelines: A comparative study. Mod Care J. 2016; 13(2):e9455. [DOI:10.17795/modernc.9455]
- Varghese S, Prasad JH, Jacob KS. Domestic violence as a risk factor for infant and child mortality: A community-based case-control study from southern India. Natl Med J India. 2013; 26(3):142-6.2-6. [PMID]
- Rawlings S, Siddique Z. Domestic violence and child mortality in the developing world. Oxf Bull Econ Stat. 2020; 82(4):723-50. [DOI:10.1111/obes.12357]
- Memiah P, Bond T, Opanga Y, Kingori C, Cook C, Mwangi M, et al. Neonatal, infant, and child mortality among women exposed to intimate partner violence in East Africa: A multi-country analysis. BMC Women’s Health. 2020; 20(1):10. [DOI:10.1186/s12905-019-0867-2] [PMID]
- World Health Organization. Every newborn: An action plan to end preventable deaths. Geneva: World Health Organization; 2014. [Link]
- World Health Organization. Born too soon: The global action report on preterm birth. Geneva: World Health Organization;2012. [Link]
- Sharifi N, Khazaeian S, Pakzad R, Chehreh H. Investigating the prevalence of preterm birth in Iranian population: A systematic review and meta-analysis. J Caring Sci. 2017; 6(4):371. [DOI:10.15171/jcs.2017.035] [PMID]
- Albarqi MN. The impact of prenatal care on the prevention of neonatal outcomes: A systematic review and meta-analysis of global health interventions. Healthcare. 2025; MDPI. [DOI:10.3390/healthcare13091076] [PMID]
- Victora CG, Bahl R, Barros AJ, França GV, Horton S, Krasevec J, et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet. 2016; 387(10017):475-90. [DOI:10.1016/S0140-6736(15)01024-7] [PMID]
- Kelishadi R, Rashidian A, Jari M, Khosravi A, Khabiri R, Elahi E, et al. National survey on the pattern of breastfeeding in Iranian infants: The IrMIDHS study. Med J Islam Repub Iran. 2016; 30:425. [PMID]
- World Health Organization. Guideline: Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services. Geneva: World Health Organization; 2017. [Link]
- Momenifar MVR, Ahmadinia HMR. Survey of the mortality trend of children under 5 years old and the economic and health status of their families during the years 2011-2020 in Rafsanjan City: A descriptive study. J Rafsanjan Univ Med Sci. 2023; 22(4):401-18. [DOI:10.61186/jrums.22.4.401]
- Chao F, Masquelier B, You D, Hug L, Liu Y, Sharrow D, et al. Sex differences in mortality among children, adolescents, and young people aged 0-24 years: a systematic assessment of national, regional, and global trends from 1990 to 2021. Lancet Glob Health. 2023; 11(10):e1519-e30. [DOI:10.1016/S2214-109X(23)00376-5] [PMID]
- Khazaei S, Ayubi E, Mansori K. High immunization coverage in children as one of the major achievements for the health system in Iran. J Pediatr Perspect. 2016; 4(7):2167-9. [Link]
- Zahraei SM, Izadi S, Gouya MM, Shahri SMH, Mohammadi M. Immunization coverage of children aged 24-35 months in the Islamic Republic of Iran: a national cluster coverage survey. Eastern Mediterranean Health Journal. 2022; 28(2):121-9. [DOI:10.26719/emhj.21.059] [PMID]
- Mahmoudiani S, Khosravi R, Javadi A. [The status and determinants of birth interval in the rural women of Fars Province, Iran (Persian)]. Iran J Nurs. 2020; 33(123):35-46. [Link]
- Saadati M, Bagheri A. Factors affecting preferred birth interval in Iran: Parametric survival analysis. Int J Cult Herit. 2019; 4:40-8. [Link]
- Dehesh T, Salarpour E, Malekmohammadi N, Kermani SA. Associated factors of pregnancy spacing among women of reproductive age Group in South of Iran: Cross-sectional study. BMC Pregnancy Childbirth. 2020; 20(1):554. [DOI:10.1186/s12884-020-03250-x] [PMID]
- Razeghi-Nasrabad HB, Hosseini-Chavoshi M, Abbasi-Shavazi MJ. An Analysis of the Second Birth Interval in Tehran, Iran: Trends and Correlates. J Midwifery Reprod Health. 2025; 13(2). [Link]
- Kim YN, Choi DW, Kim DS, Park EC, Kwon JY. Maternal age and risk of early neonatal mortality: A national cohort study. Sci Rep. 2021;11(1):814. [DOI:10.1038/s41598-021-80968-4] [PMID]
- WHO. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: WHO; 2016. [Link]
- Feleke BE, Feleke TE. A longitudinal study on the effects of previous stillbirth or abortion on subsequent pregnancies and infants. Eur J Public Health. 2021; 31(6):1237-41. [DOI:10.1093/eurpub/ckab134] [PMID]
Type of Study: Review Article |
Subject:
Management of health services in children
Received: 2025/07/13 | Accepted: 2025/10/18 | Published: 2026/01/1
Received: 2025/07/13 | Accepted: 2025/10/18 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
