
Mon, Jul 13, 2026


Volume 14, Issue 2 (April 2026)
J. Pediatr. Rev 2026, 14(2): 187-196 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Akbari H, Talebian A, Zamanian F. Comparative Efficacy of Levetiracetam and Clobazam in Preventing Recurrent Febrile Seizures in Children. J. Pediatr. Rev 2026; 14 (2) :187-196
URL: http://jpr.mazums.ac.ir/article-1-797-en.html
URL: http://jpr.mazums.ac.ir/article-1-797-en.html



1- Social Determinants of Health (SDH) Research Center, Faculty of Public Health, Kashan University of Medical Sciences, Kashan, Iran.
2- Department of Pediatrics, Faculty of Medicine, Kashan University of Medical Sciences, Kashan, Iran.
3- Department of Pediatrics, Faculty of Medicine, Kashan University of Medical Sciences, Kashan, Iran. ,dr.fa_zamanyan@yahoo.com
2- Department of Pediatrics, Faculty of Medicine, Kashan University of Medical Sciences, Kashan, Iran.
3- Department of Pediatrics, Faculty of Medicine, Kashan University of Medical Sciences, Kashan, Iran. ,
Full-Text [PDF 418 kb]
(107 Downloads)
| Abstract (HTML) (259 Views)
Full-Text: (48 Views)
Introduction
Seizures are among the most common neurological emergencies in children, and febrile seizures (FS) are the most frequent seizure type in this population [1]. FS are defined as seizures occurring in the presence of a fever of at least 38 °C, and absence of central nervous system infection, and they typically affect children between 6 months and 6 years of age [2]. The male to female ratio is about 1.6:1 and most cases occur between 12 and 18 months [1, 3].
In 2010, the International League Against Epilepsy suggested that FS could be grouped based on the age of onset, either in infancy or later in childhood. FS are typically classified as simple or complex. Simple FS are isolated, generalized seizures lasting less than 15 minutes [4]. On the other hand, complex FS are focal, prolonged (>15 minutes), or recurrent within 24 hours, and may be associated with transient neurological deficits [5]. About 20–35% of FS are considered complex, and and this proportion may reach up to 45% in children <12 months [6, 7]. Another variant, known as biphasic FS, is reported to recur 20 hours after the initial seizure [8].
FS recur in approximately 25–50% of affected children. The primary factors for recurrence include seizures onset before one year of age, a positive family history of FS, low-grade fever at seizure onset, and a short duration of fever before the seizure [9]. For parents and caregivers, watching a seizure can be extremely distressing and can greatly impact their quality of life [6]. In many cases, parents perceive FS as a life-threatening event [2]. Even though FS are quite alarming, they are self-limiting with a benign course. Nevertheless, such events often prompt pediatric consultations, and the treatment approaches vary by clinical context [1, 10].
Multiple pharmacologic strategies have been evaluated to prevent FS recurrence [11]. Antipyretic medications such as acetaminophen and ibuprofen, may relieve feverrelated discomfort but do not prevent FS recurrence [12]. Intermittent oral benzodiazepines, such as clobazam (CLB), are sometimes used to prevent FS episodes in children at high risk. CLB may be administered orally, rectally, or sublingually [13]. Although effective, the use of benzodiazepines has declined due to concerns regarding sedation and other adverse effects [14, 15]. Levetiracetam (LEV) has been evaluated in various settings and is considered a promising option for FS prevention, and is commonly prescribed for infants and young children with epilepsy [16]. The common side effects of LEV include dizziness, drowsiness, irritability, a sore throat, fatigue, and weakness. On the more serious side, some children might experience hypersensitivity reactions, such as rashes, hives, itching, and even breathing problems, as well as unusual thoughts, dark-colored urine, excessive drowsiness, marked weakness, fever, and mood changes [17]. LEV is generally well tolerated [18]. Several factors, including quick action, few drug interactions, and the option for intermittent infusion (IV) delivery, make it proves to be an optimal choice for managing seizures [19]. Although, few studies directly compare LEV with other antiepileptics [14, 15], its favorable tolerability profile underscores the need for further comparative research across diverse populations. Direct head-to-head trials comparing LEV and CLB remain limited, particularly in diverse populations where genetic or environmental factors may modulate response. This gap hinders evidence-based selection, especially as systematic reviews highlight insufficient high-quality comparative data on intermittent prophylaxis [20, 21]. Therefore, this study aimed to compare the efficacy of LEV with CLB, a widely used and effective agent for FS prevention in children.
Materials and Methods
This clinical trial involved 69 children diagnosed with FS who were referred to the Shahid Beheshti Specialized Hospital at Kashan University of Medical Sciences in Iran. A parallel-group, randomized clinical trial was used; patients received either CLB or LEV for treatment. Sample size was calculated assuming an 18% recurrence rate with CLB and 24% with LEV, using 95% confidence and 80% power, yielding 34 per group [15, 22, 23]. Observed rates (~6%) were lower, reducing power to detect small differences; this underpowering for subtle effects is a limitation.
Initially, all patients were thoroughly evaluated to rule out significant febrile diseases, such as meningitis and encephalitis. The inclusion criteria for the study were as follows:
1. Children aged between 6 months and 6 years who presented to the hospital with FS.
2. There was no previous history of seizures occurring without fever.
The exclusion criteria were
1. Patients exhibiting non-generalized seizures, seizures lasting more than 15 minutes, or seizures recurring several times within 24 hours.
2. Neurological impairment was defined as abnormal results on neurological examination, developmental delay, or progressive neurological disease.
3. Presence of metabolic disorders.
4. Seizures attributable to central nervous system infections, or secondary to other causes such as epilepsy, electrolyte disturbances, physical trauma, etc.
5. Abnormal electroencephalogram (EEG) findings.
6. Failure of parents to provide consent for the child’s continued participation in the study.
This detailed set of criteria ensured a well-defined study population and maintained the scientific validity of trial.
Randomization
Group allocation was performed using a random number table. Preprepared opaque sealed envelopes, created by an independent person, were used to assign patients to the two treatment groups (CLB and LEV), and the pediatric neurologist did the patient assignment.
Treatment with CLB
The CLB medication was given in a dose of 1 mg/kg per dose, administered twice daily for the first 48 hours of fever. The tablet was dissolved in the recommended amount of water, and this solution was administered orally to the child.
Treatment with LEV
LEV syrup medication was administered at a dose of 30 mg/kg per dose, twice daily for 48 hours following the onset of fever. The appropriate dose was measured using a dosing syringe and administered orally to the child.
Parents of the enrolled children were educated that, at the onset of any febrile illness, in addition to the specific treatment for the febrile condition and the administration of acetaminophen as prescribed by the physician, they should administer the prescribed doses of CLB and LEV exclusively during the first 48 hours of the febrile episode. After 48 hours, even if the fever persists, the administration of CLB and LEV should be discontinued.
Blinding
A single-blinded design was used for the study. While both the patients and the treating physicians were aware of the treatment allocations due to formulation differences (tablet vs syrup), the statistical analysis and interpretation of the results were performed in a blinded manner, without knowing which drug each participant received. This open-label approach risks performance/detection bias (e.g. differential side effect reporting).
Evaluation of treatment outcomes and drug side effects
A pre-treatment checklist was completed for every patient at the beginning of the study. The checklist recorded the number of fever episodes, drugrelated side effects, and recurrence of FS. Every three months, patients visited the hospital outpatient clinic, where they were examined by a specialist, and both the treatment outcomes and any drug-related side effects were evaluated. No external confirmation (e.g. ED records) or adherence monitoring was incorporated (no pill counts/syringe checks/biochemical assays). This is a limitation prone to recall and reporting bias, particularly in an unblinded study.
Study duration data and recording
The total study period was 9 months. Patients were scheduled for outpatient visits every 3 months, during which a specialist evaluated fever episodes, FS recurrence, and any drug-related side effects. Parents were provided with a checklist, along with detailed instructions on how to observe and record any instances of FS for their child or negative side effects from medicines. Parents were to keep a record of any such events in the checklist. At each follow-up visit, the specialist and resident, together with the parents, reviewed the completed checklists, (e.g. study-specific parental diary for fever episodes, seizures and side effects) after which the data were systematically recorded.
Statistical analysis
The study data were analyzed using SPSS software, version 22. For comparing FS recurrence and the occurrence of drug side effects between the two groups, the independent sample t-test and chi-square tests were utilized. In addition, logistic regression was performed to assess the effect of possible confounders. No significant confounders were identified (all P>0.05).
Results
In this study, 69 children with FS who had no history of neurological or metabolic disorders were included. Of these, 34 children received CLB and 35 received LEV. All participants were in the age range of 6 to 60 months. The Mean±SD was 23.77±13.31 months. Additionally, 40 children were female, while the remaining 29 were male.
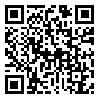
As illustrated in Table 1, among the children treated with CLB, 4(11.8%) were 12 months old or younger, while 10(28.6%) in the LEV group were younger than 12 months; the remaining children in both groups were older than 12 months.
Regarding gender distribution, 7 children (64.7%) in the CLB group were male compared with 4 children (51.4%) in the LEV group, with the rest being female. On average, participants in the CLB group were 23.5 months old, whereas those in the LEV group were 23.9 months old. No significant differences were observed between the groups in terms of age or gender (P>0.05).
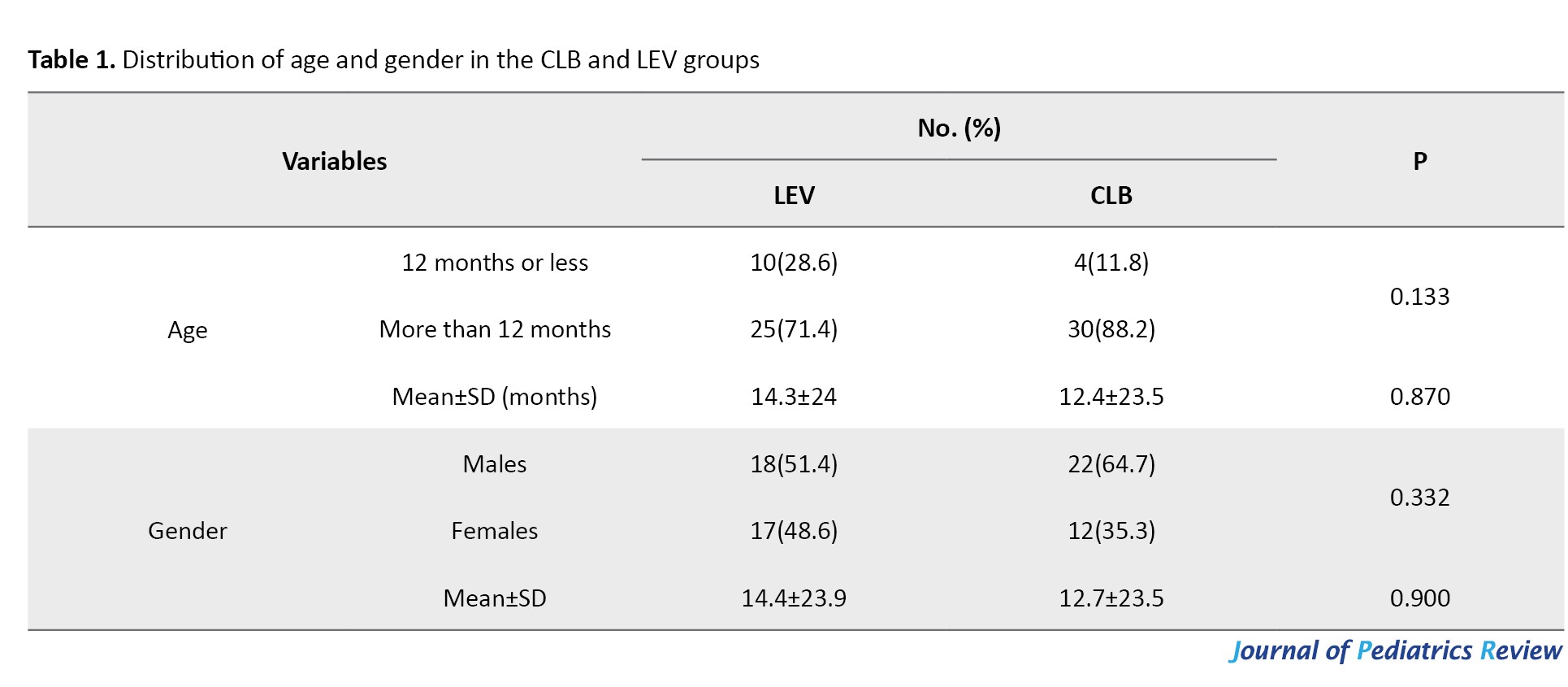
As illustrated in Table 2, the results showed that regarding initial fever, 11.8% of children in the CLB group had a fever above 38 °C, whereas none of the children in the LEV group had a fever above this level.
Additionally, 14.7% of children in the CLB group versus 9.22% in the LEV group had a family history of FS, and a family history of epilepsy was reported in 17.6% of children in the CLB group compared with 14.3% in the LEV group. Furthermore, seizures occurring 24 hours after the onset of fever were observed in 41.2% of cases in the CLB group and 94.3% in the LEV group. No statistically significant relationship were observed between the groups receiving different treatments and initial fever, family history of FS, family history of epilepsy, or the occurrence of seizures within the first 24 hours (P>0.05).
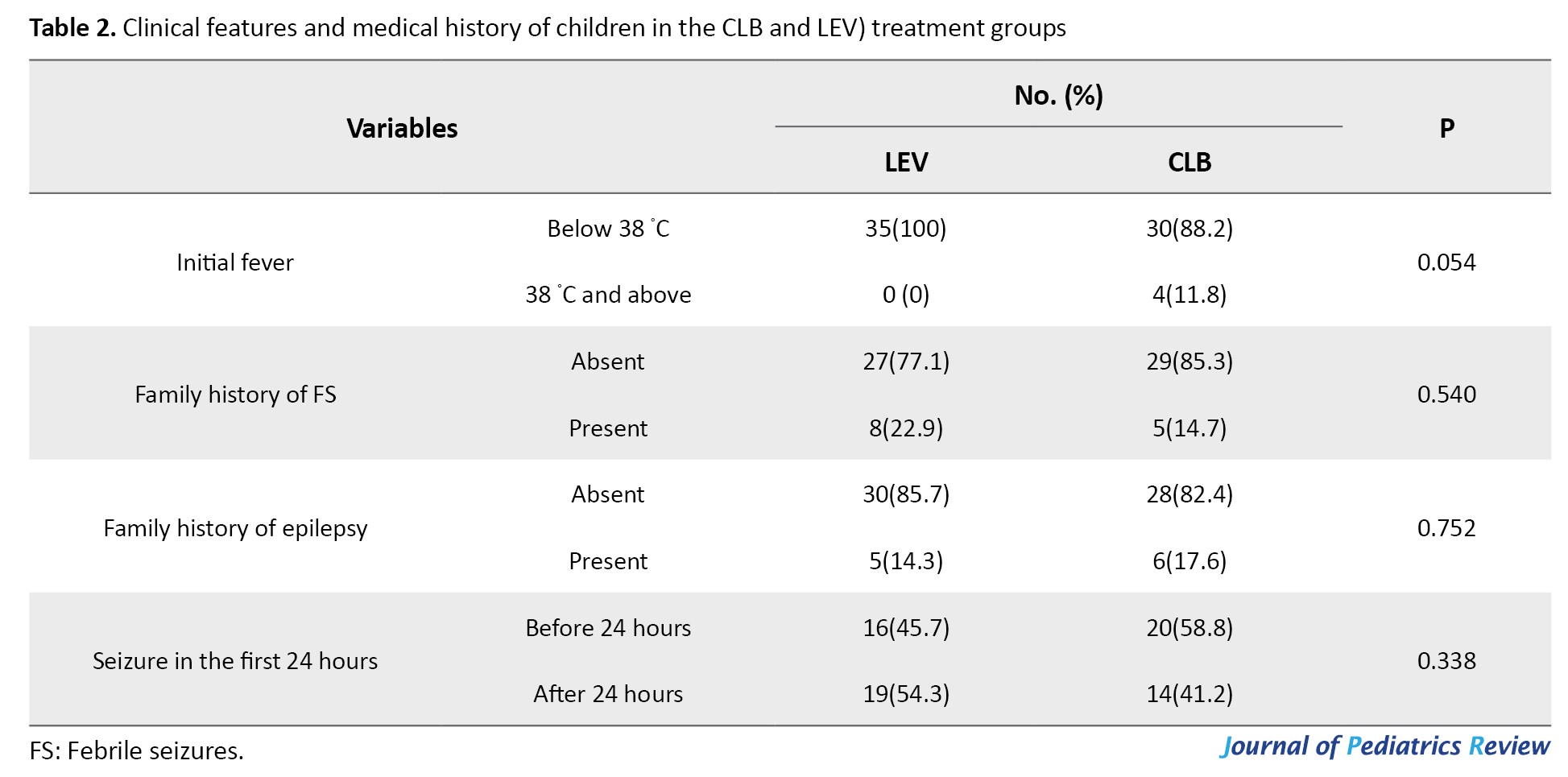
As illustrated in Table 3, our study findings indicate that in the CLB treatment group, 5.9% of the children experienced FS recurrence, compared to 5.7% in the LEV group.
The mean number of recurrences was 0.54±0.12 in the CLB group and 0.37±0.09 in the LEV group. No statistically significant relationship was observed between FS recurrence status and the treatment groups (P>0.05).
Based on Table 4, the percentage of children experiencing side effects was 58.5% in the CLB group and 60% in the LEV group.
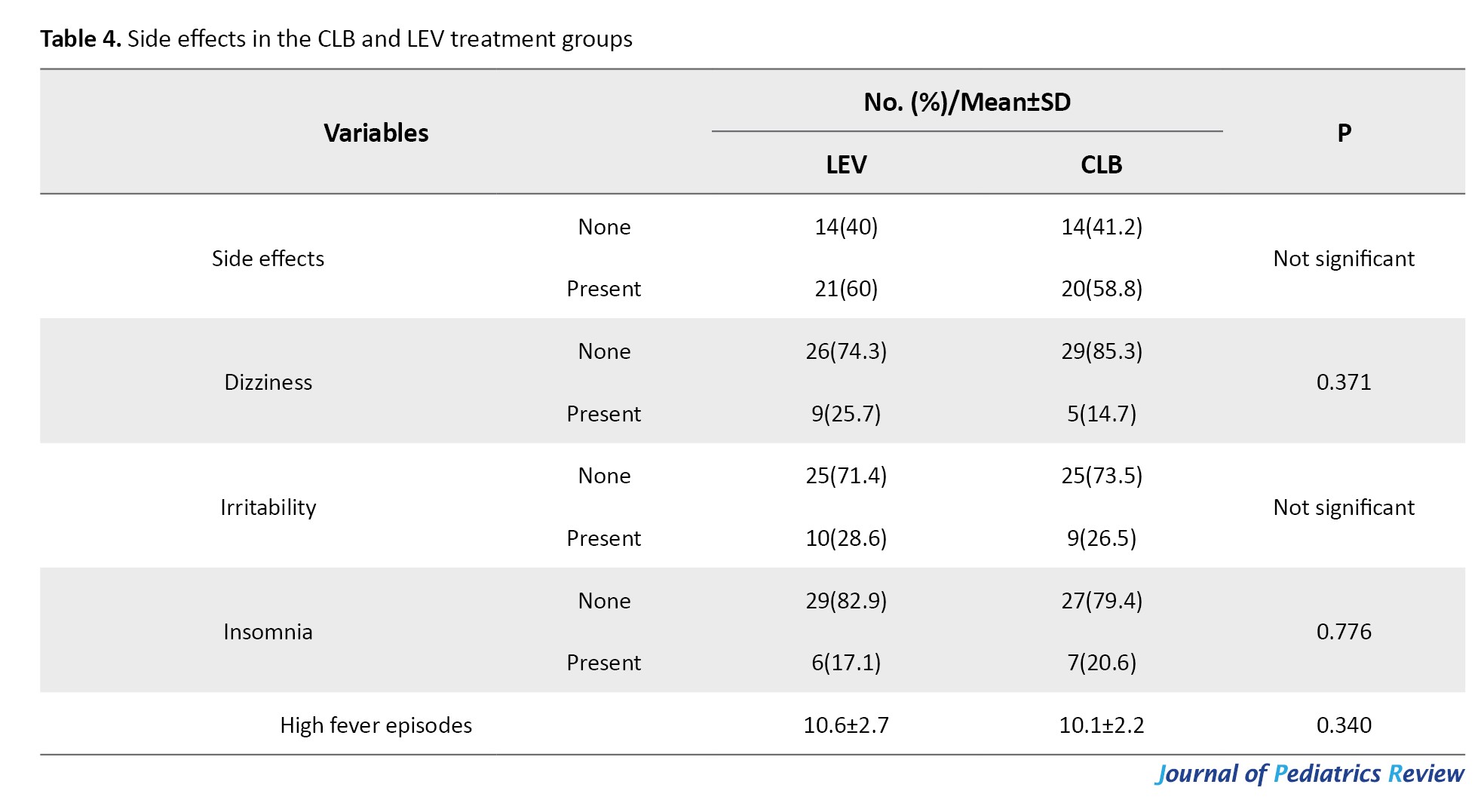
The frequency of dizziness was 14.7% in the CLB group and 25.7% in the LEV group. Similarly, irritability was reported in 26.5% of children in the CLB group and 28.6% of children in the LEV group, while insomnia was observed in 20.6% of CLB children and 17.1% of LEV children. Moreover, the percentage of high fever episodes during the treatment period was 10.1% in the CLB group and 10.6% in the LEV group. Nevertheless, no significant differences were observed in the frequency of side effects between the two treatment groups (P>0.05).
Discussion
In our study, the mean age of the children was 23.77±13.31 months in both the CLB and LEV treatment groups, with 64.7% and 51.4% of the patients being male, respectively. A family history of febrile seizure was noted in 14.7% of CLB-treated children and 22.9% in the children who received LEV, while 17.6% and 14.3% had a history of epilepsy, respectively. No significant variations between the treatment groups were observed for age, gender or a family history of FS and epilepsy (P>0.05). The recurrence rate of FS was 5.9% in the CLB group and 5.7% in the LEV group, and the mean number of recurrences was 0.54±0.12 for the CLB group compared to 0.37±0.09 for the LEV group. This difference was not statistically significant (P>0.05).
With regard to safety, side effects were observed in 58.8% of children in the CLB group, while 60% of children in the LEV group experienced side effects. Moreover, the mean number of high fever episodes during the treatment period was 10.1 in the CLB group and 10.6 in the LEV group. However, no statistically significant difference was observed between the groups in terms of possible harmful effects (P>0.05).
Following our study findings, the research by Shabani et al. (2024) indicated that the mean time to the first seizure recurrence after intervention was significantly longer in the LEV group than in the control group. In addition, the mean number of FS recurrences in the LEV group was significantly lower compared to the control group [24]. Similarly, the clinical trial by Hu et al. (2018), which evaluated the efficacy of intermittent oral LEV in preventing FS, showed that LEV can effectively prevent febrile seizure recurrences [25]. Hu et al. (2014) showed that patients receiving LEV significantly reduced the risk of FS recurrences, which suggests this oral treatment is effective in preventing FS [18]. In the study by Xu et al. (2016), the results showed no significant difference between LEV and phenytoin in terms of FS prevention [26]. In addition, Farzaneh Bajestani et al. (2021) studied oral LEV solution and oral diazepam tablets for children from 6 to 60 months when they had FS. No significant differences were observed between groups in the total seizure time, the frequency of seizures, or the average span in between them [27]. Offringa et al. (2017) found that after 50 weeks of treatment with LEV, the recurrence rate and seizure frequency in children were 15.5% and 12.4%, respectively, leading to the conclusion that LEV may be effective in preventing seizure recurrences and reducing their frequency [21]. In contrast to our study, Chaudhary et al. (2016) compared the effect of LEV with that of CLB in reducing febrile seizure recurrences in children. While LEV and CLB were both effective in preventing FS, the CLB group had fewer relapses than the LEV group [28]. In support of these results, Offringa et al. (2021) observed that CLB reduced the rate of febrile seizure recurrences more than placebo during a six-month period [20].
The equivalence observed in our trial (recurrence rates of 5.9% for CLB and 5.7% for LEV) may be attributed to comparable pharmacodynamic profiles: LEV modulates synaptic vesicle protein 2A (SV2A) to inhibit excessive neuronal firing, whereas CLB enhances gammaaminobutyric acid (GABAA) receptor activity [29]. The unexpectedly low recurrence rate in both arms (~6% versus anticipated 18–24%) likely reflects several factors, including the enrollment of simple FS cases, potential underreporting via parental checklists, and the limited 9-month follow-up duration. These elements, while enhancing internal validity within a low-risk cohort, constrain detection of subtle inter-group differences and limit external applicability to children with complex FS or neurodevelopmental comorbidities.
Critical comparison with prior literature reveals methodological heterogeneity as a key driver of divergent outcomes. For instance, Chaudhary et al. (2016) reported CLB superiority, possibly due to variations in dosing regimens, population demographics, or blinding status [28]. Ethnic and genetic factors influencing drug metabolism or seizure susceptibility may further contribute to inconsistencies across studies; such variables merit targeted investigation in future multi-ethnic trials.
In the present study, 14.7% of children in the CLB treatment group and 22.9% in the LEV group had a family history of FS. Similar studies have pointed out that LEV is effective in treating focal, myoclonic, and tonic-colonic epilepsies [26]. Besides, LEV prevents repetitive neuronal firing by inhibiting the generation of consecutive action potentials [29]. LEV is not extensively metabolized in the body and is mostly removed through the urine. When administered orally, the medicine is quickly and almost fully absorbed by children. Because this drug lacks significant hepatic metabolism and has low protein binding, the risk of side effects is very low, and monitoring in routine blood tests is unnecessary [30]. Another study indicated that the risk of recurrent FS is approximately 30–40%, which may be attributed to both genetic and environmental factors. Furthermore, the risk of FS recurrence is higher when seizures occur at an early age and when the child has a family history of FS [31]. According to Li et al., administering 1000–2500 mg of LEV every day provided effective control of myoclonic seizures in adolescents, with no patients experiencing any side effects [32].
Our study showed that the LEV therapy was highly effective, and no major negative effects occurred. LEV has been found not to be associated with serious systemic side effects [27]. Furthermore, allergic eruptions due to LEV are extremely rare, showing a significant difference when compared with other antiepileptic drugs [33]. A systematic review by Chen et al. (2018) confirmed that the side effects of LEV are acceptable [34]. In addition, Xu et al. (2016) found that, in the prevention of FS, LEV is associated with fewer drug-related side effects than phenytoin [26]. The results from Hu et al. (2014) indicated that only one patient out of the group had drowsiness after being given LEV. To clarify, it is difficult to say if the symptom was due to the drug or is simply due to the fever, as this patient had no past history of side effects. Moreover, no other side effects were observed in the remaining patients. Overall, intermittent LEV treatment has proven to be safe for patients with FS [18].
Strengths of the current investigation include its randomized design, a priori sample size calculation grounded in established recurrence estimates, predefined inclusion/exclusion criteria that ensured cohort homogeneity, and regular specialist oversight during follow-up visits. Weaknesses encompass the single-blind approach (introducing risks of performance and detection bias), reliance on an unvalidated parental checklist without objective verification (e.g. emergency department records or video confirmation), absence of formal adherence monitoring (pill counts, syringe returns, or biochemical assays), and reduced statistical power owing to lower-than-expected event rates.
This investigation provides supportive evidence that intermittent oral LEV and CLB yield comparable efficacy and tolerability in preventing FS recurrence among children with predominantly simple seizures. Larger, multi-center, double-blind randomized controlled trials incorporating validated seizure diaries, objective adherence measures, extended follow-up periods, and inclusion of complex FS cases are recommended to confirm these findings and enhance generalizability.
Conclusion
The present study indicated that LEV and CLB have similar effects in preventing FS in children, as no statistically significant differences were observed between the groups in recurrence rates or sideeffect incidence. This study provides supportive data that may assist clinicians in selecting appropriate strategies for FS prevention in children. Moreover, to better assess the role of LEV in managing FS in children under 60 months, additional randomized controlled trials with larger sample sizes and longer followup periods are needed.
Limitations
During the follow-up, some parents failed to cooperate or respond, which was a restriction for this study. To overcome the challenge, we made sure to communicate with families often and constantly reminded them of the treatment goals, which encouraged their ongoing participation and follow-up. Additional limitations include the single-blind design, lack of adherence monitoring, reliance on unvalidated checklists/diary, and reduced power due to low event rates; these factors may have influenced outcome assessment and generalizability.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Kashan University of Medical Sciences, Kashan, Iran (Code: IR.kAUMS.MEDNT.REC.1399.213). In addition, this study was registered with the Iranian Registry of Clinical Trials (IRCT), Tehran, Iran (Code: IRCT20210911052441N1).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors equally contributed to preparing this article.
Conflicts of interest
The authors declared no conflict of interest.
References
Seizures are among the most common neurological emergencies in children, and febrile seizures (FS) are the most frequent seizure type in this population [1]. FS are defined as seizures occurring in the presence of a fever of at least 38 °C, and absence of central nervous system infection, and they typically affect children between 6 months and 6 years of age [2]. The male to female ratio is about 1.6:1 and most cases occur between 12 and 18 months [1, 3].
In 2010, the International League Against Epilepsy suggested that FS could be grouped based on the age of onset, either in infancy or later in childhood. FS are typically classified as simple or complex. Simple FS are isolated, generalized seizures lasting less than 15 minutes [4]. On the other hand, complex FS are focal, prolonged (>15 minutes), or recurrent within 24 hours, and may be associated with transient neurological deficits [5]. About 20–35% of FS are considered complex, and and this proportion may reach up to 45% in children <12 months [6, 7]. Another variant, known as biphasic FS, is reported to recur 20 hours after the initial seizure [8].
FS recur in approximately 25–50% of affected children. The primary factors for recurrence include seizures onset before one year of age, a positive family history of FS, low-grade fever at seizure onset, and a short duration of fever before the seizure [9]. For parents and caregivers, watching a seizure can be extremely distressing and can greatly impact their quality of life [6]. In many cases, parents perceive FS as a life-threatening event [2]. Even though FS are quite alarming, they are self-limiting with a benign course. Nevertheless, such events often prompt pediatric consultations, and the treatment approaches vary by clinical context [1, 10].
Multiple pharmacologic strategies have been evaluated to prevent FS recurrence [11]. Antipyretic medications such as acetaminophen and ibuprofen, may relieve feverrelated discomfort but do not prevent FS recurrence [12]. Intermittent oral benzodiazepines, such as clobazam (CLB), are sometimes used to prevent FS episodes in children at high risk. CLB may be administered orally, rectally, or sublingually [13]. Although effective, the use of benzodiazepines has declined due to concerns regarding sedation and other adverse effects [14, 15]. Levetiracetam (LEV) has been evaluated in various settings and is considered a promising option for FS prevention, and is commonly prescribed for infants and young children with epilepsy [16]. The common side effects of LEV include dizziness, drowsiness, irritability, a sore throat, fatigue, and weakness. On the more serious side, some children might experience hypersensitivity reactions, such as rashes, hives, itching, and even breathing problems, as well as unusual thoughts, dark-colored urine, excessive drowsiness, marked weakness, fever, and mood changes [17]. LEV is generally well tolerated [18]. Several factors, including quick action, few drug interactions, and the option for intermittent infusion (IV) delivery, make it proves to be an optimal choice for managing seizures [19]. Although, few studies directly compare LEV with other antiepileptics [14, 15], its favorable tolerability profile underscores the need for further comparative research across diverse populations. Direct head-to-head trials comparing LEV and CLB remain limited, particularly in diverse populations where genetic or environmental factors may modulate response. This gap hinders evidence-based selection, especially as systematic reviews highlight insufficient high-quality comparative data on intermittent prophylaxis [20, 21]. Therefore, this study aimed to compare the efficacy of LEV with CLB, a widely used and effective agent for FS prevention in children.
Materials and Methods
This clinical trial involved 69 children diagnosed with FS who were referred to the Shahid Beheshti Specialized Hospital at Kashan University of Medical Sciences in Iran. A parallel-group, randomized clinical trial was used; patients received either CLB or LEV for treatment. Sample size was calculated assuming an 18% recurrence rate with CLB and 24% with LEV, using 95% confidence and 80% power, yielding 34 per group [15, 22, 23]. Observed rates (~6%) were lower, reducing power to detect small differences; this underpowering for subtle effects is a limitation.
Initially, all patients were thoroughly evaluated to rule out significant febrile diseases, such as meningitis and encephalitis. The inclusion criteria for the study were as follows:
1. Children aged between 6 months and 6 years who presented to the hospital with FS.
2. There was no previous history of seizures occurring without fever.
The exclusion criteria were
1. Patients exhibiting non-generalized seizures, seizures lasting more than 15 minutes, or seizures recurring several times within 24 hours.
2. Neurological impairment was defined as abnormal results on neurological examination, developmental delay, or progressive neurological disease.
3. Presence of metabolic disorders.
4. Seizures attributable to central nervous system infections, or secondary to other causes such as epilepsy, electrolyte disturbances, physical trauma, etc.
5. Abnormal electroencephalogram (EEG) findings.
6. Failure of parents to provide consent for the child’s continued participation in the study.
This detailed set of criteria ensured a well-defined study population and maintained the scientific validity of trial.
Randomization
Group allocation was performed using a random number table. Preprepared opaque sealed envelopes, created by an independent person, were used to assign patients to the two treatment groups (CLB and LEV), and the pediatric neurologist did the patient assignment.
Treatment with CLB
The CLB medication was given in a dose of 1 mg/kg per dose, administered twice daily for the first 48 hours of fever. The tablet was dissolved in the recommended amount of water, and this solution was administered orally to the child.
Treatment with LEV
LEV syrup medication was administered at a dose of 30 mg/kg per dose, twice daily for 48 hours following the onset of fever. The appropriate dose was measured using a dosing syringe and administered orally to the child.
Parents of the enrolled children were educated that, at the onset of any febrile illness, in addition to the specific treatment for the febrile condition and the administration of acetaminophen as prescribed by the physician, they should administer the prescribed doses of CLB and LEV exclusively during the first 48 hours of the febrile episode. After 48 hours, even if the fever persists, the administration of CLB and LEV should be discontinued.
Blinding
A single-blinded design was used for the study. While both the patients and the treating physicians were aware of the treatment allocations due to formulation differences (tablet vs syrup), the statistical analysis and interpretation of the results were performed in a blinded manner, without knowing which drug each participant received. This open-label approach risks performance/detection bias (e.g. differential side effect reporting).
Evaluation of treatment outcomes and drug side effects
A pre-treatment checklist was completed for every patient at the beginning of the study. The checklist recorded the number of fever episodes, drugrelated side effects, and recurrence of FS. Every three months, patients visited the hospital outpatient clinic, where they were examined by a specialist, and both the treatment outcomes and any drug-related side effects were evaluated. No external confirmation (e.g. ED records) or adherence monitoring was incorporated (no pill counts/syringe checks/biochemical assays). This is a limitation prone to recall and reporting bias, particularly in an unblinded study.
Study duration data and recording
The total study period was 9 months. Patients were scheduled for outpatient visits every 3 months, during which a specialist evaluated fever episodes, FS recurrence, and any drug-related side effects. Parents were provided with a checklist, along with detailed instructions on how to observe and record any instances of FS for their child or negative side effects from medicines. Parents were to keep a record of any such events in the checklist. At each follow-up visit, the specialist and resident, together with the parents, reviewed the completed checklists, (e.g. study-specific parental diary for fever episodes, seizures and side effects) after which the data were systematically recorded.
Statistical analysis
The study data were analyzed using SPSS software, version 22. For comparing FS recurrence and the occurrence of drug side effects between the two groups, the independent sample t-test and chi-square tests were utilized. In addition, logistic regression was performed to assess the effect of possible confounders. No significant confounders were identified (all P>0.05).
Results
In this study, 69 children with FS who had no history of neurological or metabolic disorders were included. Of these, 34 children received CLB and 35 received LEV. All participants were in the age range of 6 to 60 months. The Mean±SD was 23.77±13.31 months. Additionally, 40 children were female, while the remaining 29 were male.
As illustrated in Table 1, among the children treated with CLB, 4(11.8%) were 12 months old or younger, while 10(28.6%) in the LEV group were younger than 12 months; the remaining children in both groups were older than 12 months.
Regarding gender distribution, 7 children (64.7%) in the CLB group were male compared with 4 children (51.4%) in the LEV group, with the rest being female. On average, participants in the CLB group were 23.5 months old, whereas those in the LEV group were 23.9 months old. No significant differences were observed between the groups in terms of age or gender (P>0.05).
As illustrated in Table 2, the results showed that regarding initial fever, 11.8% of children in the CLB group had a fever above 38 °C, whereas none of the children in the LEV group had a fever above this level.
Additionally, 14.7% of children in the CLB group versus 9.22% in the LEV group had a family history of FS, and a family history of epilepsy was reported in 17.6% of children in the CLB group compared with 14.3% in the LEV group. Furthermore, seizures occurring 24 hours after the onset of fever were observed in 41.2% of cases in the CLB group and 94.3% in the LEV group. No statistically significant relationship were observed between the groups receiving different treatments and initial fever, family history of FS, family history of epilepsy, or the occurrence of seizures within the first 24 hours (P>0.05).
As illustrated in Table 3, our study findings indicate that in the CLB treatment group, 5.9% of the children experienced FS recurrence, compared to 5.7% in the LEV group.
The mean number of recurrences was 0.54±0.12 in the CLB group and 0.37±0.09 in the LEV group. No statistically significant relationship was observed between FS recurrence status and the treatment groups (P>0.05).
Based on Table 4, the percentage of children experiencing side effects was 58.5% in the CLB group and 60% in the LEV group.
The frequency of dizziness was 14.7% in the CLB group and 25.7% in the LEV group. Similarly, irritability was reported in 26.5% of children in the CLB group and 28.6% of children in the LEV group, while insomnia was observed in 20.6% of CLB children and 17.1% of LEV children. Moreover, the percentage of high fever episodes during the treatment period was 10.1% in the CLB group and 10.6% in the LEV group. Nevertheless, no significant differences were observed in the frequency of side effects between the two treatment groups (P>0.05).
Discussion
In our study, the mean age of the children was 23.77±13.31 months in both the CLB and LEV treatment groups, with 64.7% and 51.4% of the patients being male, respectively. A family history of febrile seizure was noted in 14.7% of CLB-treated children and 22.9% in the children who received LEV, while 17.6% and 14.3% had a history of epilepsy, respectively. No significant variations between the treatment groups were observed for age, gender or a family history of FS and epilepsy (P>0.05). The recurrence rate of FS was 5.9% in the CLB group and 5.7% in the LEV group, and the mean number of recurrences was 0.54±0.12 for the CLB group compared to 0.37±0.09 for the LEV group. This difference was not statistically significant (P>0.05).
With regard to safety, side effects were observed in 58.8% of children in the CLB group, while 60% of children in the LEV group experienced side effects. Moreover, the mean number of high fever episodes during the treatment period was 10.1 in the CLB group and 10.6 in the LEV group. However, no statistically significant difference was observed between the groups in terms of possible harmful effects (P>0.05).
Following our study findings, the research by Shabani et al. (2024) indicated that the mean time to the first seizure recurrence after intervention was significantly longer in the LEV group than in the control group. In addition, the mean number of FS recurrences in the LEV group was significantly lower compared to the control group [24]. Similarly, the clinical trial by Hu et al. (2018), which evaluated the efficacy of intermittent oral LEV in preventing FS, showed that LEV can effectively prevent febrile seizure recurrences [25]. Hu et al. (2014) showed that patients receiving LEV significantly reduced the risk of FS recurrences, which suggests this oral treatment is effective in preventing FS [18]. In the study by Xu et al. (2016), the results showed no significant difference between LEV and phenytoin in terms of FS prevention [26]. In addition, Farzaneh Bajestani et al. (2021) studied oral LEV solution and oral diazepam tablets for children from 6 to 60 months when they had FS. No significant differences were observed between groups in the total seizure time, the frequency of seizures, or the average span in between them [27]. Offringa et al. (2017) found that after 50 weeks of treatment with LEV, the recurrence rate and seizure frequency in children were 15.5% and 12.4%, respectively, leading to the conclusion that LEV may be effective in preventing seizure recurrences and reducing their frequency [21]. In contrast to our study, Chaudhary et al. (2016) compared the effect of LEV with that of CLB in reducing febrile seizure recurrences in children. While LEV and CLB were both effective in preventing FS, the CLB group had fewer relapses than the LEV group [28]. In support of these results, Offringa et al. (2021) observed that CLB reduced the rate of febrile seizure recurrences more than placebo during a six-month period [20].
The equivalence observed in our trial (recurrence rates of 5.9% for CLB and 5.7% for LEV) may be attributed to comparable pharmacodynamic profiles: LEV modulates synaptic vesicle protein 2A (SV2A) to inhibit excessive neuronal firing, whereas CLB enhances gammaaminobutyric acid (GABAA) receptor activity [29]. The unexpectedly low recurrence rate in both arms (~6% versus anticipated 18–24%) likely reflects several factors, including the enrollment of simple FS cases, potential underreporting via parental checklists, and the limited 9-month follow-up duration. These elements, while enhancing internal validity within a low-risk cohort, constrain detection of subtle inter-group differences and limit external applicability to children with complex FS or neurodevelopmental comorbidities.
Critical comparison with prior literature reveals methodological heterogeneity as a key driver of divergent outcomes. For instance, Chaudhary et al. (2016) reported CLB superiority, possibly due to variations in dosing regimens, population demographics, or blinding status [28]. Ethnic and genetic factors influencing drug metabolism or seizure susceptibility may further contribute to inconsistencies across studies; such variables merit targeted investigation in future multi-ethnic trials.
In the present study, 14.7% of children in the CLB treatment group and 22.9% in the LEV group had a family history of FS. Similar studies have pointed out that LEV is effective in treating focal, myoclonic, and tonic-colonic epilepsies [26]. Besides, LEV prevents repetitive neuronal firing by inhibiting the generation of consecutive action potentials [29]. LEV is not extensively metabolized in the body and is mostly removed through the urine. When administered orally, the medicine is quickly and almost fully absorbed by children. Because this drug lacks significant hepatic metabolism and has low protein binding, the risk of side effects is very low, and monitoring in routine blood tests is unnecessary [30]. Another study indicated that the risk of recurrent FS is approximately 30–40%, which may be attributed to both genetic and environmental factors. Furthermore, the risk of FS recurrence is higher when seizures occur at an early age and when the child has a family history of FS [31]. According to Li et al., administering 1000–2500 mg of LEV every day provided effective control of myoclonic seizures in adolescents, with no patients experiencing any side effects [32].
Our study showed that the LEV therapy was highly effective, and no major negative effects occurred. LEV has been found not to be associated with serious systemic side effects [27]. Furthermore, allergic eruptions due to LEV are extremely rare, showing a significant difference when compared with other antiepileptic drugs [33]. A systematic review by Chen et al. (2018) confirmed that the side effects of LEV are acceptable [34]. In addition, Xu et al. (2016) found that, in the prevention of FS, LEV is associated with fewer drug-related side effects than phenytoin [26]. The results from Hu et al. (2014) indicated that only one patient out of the group had drowsiness after being given LEV. To clarify, it is difficult to say if the symptom was due to the drug or is simply due to the fever, as this patient had no past history of side effects. Moreover, no other side effects were observed in the remaining patients. Overall, intermittent LEV treatment has proven to be safe for patients with FS [18].
Strengths of the current investigation include its randomized design, a priori sample size calculation grounded in established recurrence estimates, predefined inclusion/exclusion criteria that ensured cohort homogeneity, and regular specialist oversight during follow-up visits. Weaknesses encompass the single-blind approach (introducing risks of performance and detection bias), reliance on an unvalidated parental checklist without objective verification (e.g. emergency department records or video confirmation), absence of formal adherence monitoring (pill counts, syringe returns, or biochemical assays), and reduced statistical power owing to lower-than-expected event rates.
This investigation provides supportive evidence that intermittent oral LEV and CLB yield comparable efficacy and tolerability in preventing FS recurrence among children with predominantly simple seizures. Larger, multi-center, double-blind randomized controlled trials incorporating validated seizure diaries, objective adherence measures, extended follow-up periods, and inclusion of complex FS cases are recommended to confirm these findings and enhance generalizability.
Conclusion
The present study indicated that LEV and CLB have similar effects in preventing FS in children, as no statistically significant differences were observed between the groups in recurrence rates or sideeffect incidence. This study provides supportive data that may assist clinicians in selecting appropriate strategies for FS prevention in children. Moreover, to better assess the role of LEV in managing FS in children under 60 months, additional randomized controlled trials with larger sample sizes and longer followup periods are needed.
Limitations
During the follow-up, some parents failed to cooperate or respond, which was a restriction for this study. To overcome the challenge, we made sure to communicate with families often and constantly reminded them of the treatment goals, which encouraged their ongoing participation and follow-up. Additional limitations include the single-blind design, lack of adherence monitoring, reliance on unvalidated checklists/diary, and reduced power due to low event rates; these factors may have influenced outcome assessment and generalizability.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Kashan University of Medical Sciences, Kashan, Iran (Code: IR.kAUMS.MEDNT.REC.1399.213). In addition, this study was registered with the Iranian Registry of Clinical Trials (IRCT), Tehran, Iran (Code: IRCT20210911052441N1).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors equally contributed to preparing this article.
Conflicts of interest
The authors declared no conflict of interest.
References
- Sawires R, Buttery J, Fahey M. A review of febrile seizures: Recent advances in understanding of febrile seizure pathophysiology and commonly implicated viral triggers. Front Pediatr. 2022; 9:801321. [DOI:10.3389/fped.2021.801321] [PMID]
- Eilbert W, Chan C. Febrile seizures: A review. J Am Coll Emerg Physicians Open. 2022; 3(4):e12769. [DOI:10.1002/emp2.12769] [PMID]
- Leung AK, Hon KL, Leung TN. Febrile seizures: An overview. Drugs Context. 2018; 7:212536. [DOI:10.7573/dic.212536] [PMID]
- Sharafi R, Hassanzadeh Rad A, Aminzadeh V. Circadian Rhythm and the Seasonal Variation in Childhood Febrile Seizure. Iran J Child Neurol. 2017; 11(3):27-30. [PMID]
- Whelan H, Harmelink M, Chou E, Sallowm D, Khan N, Patil R, et al. Complex febrile seizures-A systematic review. Dis Mon. 2017; 63(1):5-23. [DOI:10.1016/j.disamonth.2016.12.001] [PMID]
- Ferretti A, Riva A, Fabrizio A, Bruni O, Capovilla G, Foiadelli T, et al. Best practices for the management of febrile seizures in children. Ital J Pediatr. 2024; 50(1):95. [DOI:10.1186/s13052-024-01666-1] [PMID]
- Francis JR, Richmond P, Robins C, Lindsay K, Levy A, Effler PV, et al. An observational study of febrile seizures: The importance of viral infection and immunization. BMC Pediatr. 2016; 16(1):202. [DOI:10.1186/s12887-016-0740-5] [PMID]
- Kumar N, Midha T, Rao YK. Risk Factors of recurrence of febrile seizures in children in a tertiary care hospital in Kanpur: A one year follow up study. Ann Indian Acad Neurol. 2019; 22(1):31-6. [DOI:10.4103/aian.AIAN_472_17] [PMID]
- Canpolat M, Per H, Gumus H, Elmali F, Kumandas S. Investigating the prevalence of febrile convulsion in Kayseri, Turkey: An assessment of the risk factors for recurrence of febrile convulsion and for development of epilepsy. Seizure. 2018; 55:36-47. [DOI:10.1016/j.seizure.2018.01.007] [PMID]
- Minardi C, Minacapelli R, Valastro P, Vasile F, Pitino S, Pavone P, et al. Epilepsy in children: From diagnosis to treatment with focus on emergency. J Clin Med. 2019; 8(1):39. [DOI:10.3390/jcm8010039] [PMID]
- Smith DK, Sadler KP, Benedum M. Febrile seizures: Risks, evaluation, and prognosis. Am Fam Physician. 2019; 99(7):445-50. [PMID]
- Gontko-Romanowska K, Żaba Z, Panieński P, Steinborn B, Szemień M, Łukasik-Głębocka M, et al. The assessment of laboratory parameters in children with fever and febrile seizures. Brain Behav. 2017; 7(7):e00720. [DOI:10.1002/brb3.720] [PMID]
- Pavlidou E, Tzitiridou M, Panteliadis C. Effectiveness of intermittent diazepam prophylaxis in febrile seizures: long-term prospective controlled study. J Child Neurol. 2006; 21(12):1036-40. [DOI:10.1177/7010.2006.00221] [PMID]
- Faraji Gavgani L, Laghousi D, Sarbakhsh P, Jahangiri L, Vahed N, Hajebrahimi S. Comparing the effect of intermittent diazepam and continuous phenobarbital in preventing recurrent febrile seizures among children under 6 years old: A systematic review and meta-analysis. J Res Med Sci. 2023; 28:38. [DOI:10.4103/jrms.jrms_1114_21] [PMID]
- Khosroshahi N, Faramarzi F, Salamati P, Haghighi SM, Kamrani K. Diazepam versus clobazam for intermittent prophylaxis of febrile seizures. Indian J Pediatr. 2011; 78(1):38-40. [DOI:10.1007/s12098-010-0220-0] [PMID]
- Grinspan ZM, Shellhaas RA, Coryell J, Sullivan JE, Wirrell EC, Mytinger JR, et al. Comparative effectiveness of levetiracetam vs phenobarbital for infantile epilepsy. JAMA Pediatr. 2018; 172(4):352-60. [DOI:10.1001/jamapediatrics.2017.5211] [PMID]
- Pizza V, Busillo V, Agresta A, Bisogno A, Capasso A. Elderly patients with migraine: An open-label study on prophylaxis therapy with levetiracetam. Cent Nerv Syst Agents Med Chem. 2011; 11(1):31-4. [DOI:10.2174/187152411794961086] [PMID]
- Hu LY, Zou LP, Zhong JM, Gao L, Zhao JB, Xiao N, et al. Febrile seizure recurrence reduced by intermittent oral levetiracetam. Ann Clin Transl Neurol. 2014; 1(3):171-9. [DOI:10.1002/acn3.34] [PMID]
- Mruk AL, Garlitz KL, Leung NR. Levetiracetam in neonatal seizures: A review. J Pediatr Pharmacol Ther. 2015; 20(2):76-89. [DOI:10.5863/1551-6776-20.2.76] [PMID]
- Offringa M, Newton R, Nevitt SJ, Vraka K. Prophylactic drug management for febrile seizures in children. Cochrane Database Syst Rev. 2021; 6(6):Cd003031. [DOI:10.1002/14651858.CD003031.pub4] [PMID]
- Offringa M, Newton R, Cozijnsen MA, Nevitt SJ. Prophylactic drug management for febrile seizures in children. Cochrane Database Syst Rev. 2017; 2(2):Cd003031. [DOI:10.1002/14651858.CD003031.pub3]
- Manreza ML, Gherpelli JL, Machado-Haertel LR, Pedreira CC, Heise CO, Diament A. Treatment of febrile seizures with intermittent clobazam. Arq Neuropsiquiatr. 1997; 55(4):757-61. [DOI:10.1590/S0004-282X1997000500012] [PMID]
- Rose W, Kirubakaran C, Scott JX. Intermittent clobazam therapy in febrile seizures. Indian J Pediatr. 2005; 72(1):31-3. [DOI:10.1007/BF02760577] [PMID]
- Shabani J, Hemmati M, Sedighi M. The effect of intermittent oral anticonvulsant levetiracetam in prevention of recurrence of febrile seizure in children: A randomized clinical trial study. J Adv Med Biomed Res. 2024; 32(152):168-73. [DOI:10.61186/jambr.32.152.168]
- Hu LY, Shi XY, Li H, Zhang MN, Ma SF, Zou LP. Intermittent oral levetiracetam reduced recurrence of febrile seizure accompanied with epileptiform discharge: A pilot study. Ital J Pediatr. 2018; 44(1):70. [DOI:10.1186/s13052-018-0507-8] [PMID]
- Xu JC, Shen J, Shao WZ, Tang LJ, Sun YZ, Zhai XF, et al. The safety and efficacy of levetiracetam versus phenytoin for seizure prophylaxis after traumatic brain injury: A systematic review and meta-analysis. Brain Inj. 2016; 30(9):1054-61. [DOI:10.3109/02699052.2016.1170882] [PMID]
- GSPFBS, Pirzadeh Z, Farshadmoghadam H. Comparison of the effect of oral levetiracetam solution and intermittent oral diazepam tablets in reducing the recurrence of febrile seizures in children 6-60 months. Pakistan Journal of Medical & Health Sciences. 2021;15(4):1530-4. [Link]
- Chaudhary N, Narayana R, Chaudhary S. Reduction of febrile seizure recurrence comparative efficacy of intermittent oral levetiracetam vs clobazam (P3.239). Neurology. 2016; 86(16_supplement):P3.239. [DOI:10.1212/WNL.86.16_supplement.P3.239]
- Abou-Khalil B. Levetiracetam in the treatment of epilepsy. Neuropsychiatr Dis Treat. 2008; 4(3):507-23. [DOI:10.2147/NDT.S2937] [PMID]
- Kaminski RM, Matagne A, Leclercq K, Gillard M, Michel P, Kenda B, et al. SV2A protein is a broad-spectrum anticonvulsant target: functional correlation between protein binding and seizure protection in models of both partial and generalized epilepsy. Neuropharmacology. 2008; 54(4):715-20. [DOI:10.1016/j.neuropharm.2007.11.021] [PMID]
- Lynch BA, Lambeng N, Nocka K, Kensel-Hammes P, Bajjalieh SM, Matagne A, et al. The synaptic vesicle protein SV2A is the binding site for the antiepileptic drug levetiracetam. Proc Natl Acad Sci U S A. 2004; 101(26):9861-6. [DOI:10.1073/pnas.0308208101] [PMID]
- Li XC, Lu LL, Wang JZ, Wang M, Gao Y, Lin YX, et al. Clinical characteristics and electroencephalogram analysis of levetiracetam in the treatment of children with febrile seizure recurrence. Exp Ther Med. 2017; 14(3):2015-20. [DOI:10.3892/etm.2017.4738] [PMID]
- Arif H, Buchsbaum R, Weintraub D, Koyfman S, Salas-Humara C, Bazil CW, et al. Comparison and predictors of rash associated with 15 antiepileptic drugs. Neurology. 2007; 68(20):1701-9. [DOI:10.1212/01.wnl.0000261917.83337.db] [PMID]
- Chen YH, Kuo TT, Yi-Kung Huang E, Hoffer BJ, Chou YC, Chiang YH, et al. Profound deficits in hippocampal synaptic plasticity after traumatic brain injury and seizure is ameliorated by prophylactic levetiracetam. Oncotarget. 2018; 9(14):11515-27. [DOI:10.18632/oncotarget.23923] [PMID]
Type of Study: Original Article |
Subject:
Pediatrics
Received: 2025/09/17 | Accepted: 2026/04/3 | Published: 2026/04/3
Received: 2025/09/17 | Accepted: 2026/04/3 | Published: 2026/04/3
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
