
Mon, Jul 13, 2026


Volume 14, Issue 2 (April 2026)
J. Pediatr. Rev 2026, 14(2): 155-162 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Wandalsen G, Treglia M, Penha M, Dos Dos Reis S, Solé D. Nebulized Corticosteroids for Asthma Exacerbations in Children: The Role of Beclomethasone Dipropionate. J. Pediatr. Rev 2026; 14 (2) :155-162
URL: http://jpr.mazums.ac.ir/article-1-807-en.html
URL: http://jpr.mazums.ac.ir/article-1-807-en.html



1- Pensi Institute, Federal University of São Paulo, São Paulo, Brazil. , gfwandalsen@unifesp.br
2- Medical Department, Chiesi Pharmaceuticals of Brazil, São Paulo, Brazil.
3- Pensi Institute, Federal University of São Paulo, São Paulo, Brazil.
2- Medical Department, Chiesi Pharmaceuticals of Brazil, São Paulo, Brazil.
3- Pensi Institute, Federal University of São Paulo, São Paulo, Brazil.
Full-Text [PDF 490 kb]
(107 Downloads)
| Abstract (HTML) (233 Views)
Full-Text: (41 Views)
Introduction
Inhaled corticosteroids (ICS) are the most effective anti-inflammatory agents for long-term asthma management, and their beneficial therapeutic effects are directly related to the reduction of airway inflammation [1]. Regular use reduces symptoms, exacerbations and hospitalizations, improve quality of life and lung function, and reduce asthma-related deaths [2].
Asthma exacerbations are acute or subacute episodes of worsening symptoms and lung function. Asthma exacerbations are responsible for numerous emergency department visits, hospitalizations, and use of systemic corticosteroids (SCS) [2]. SCS remain the standard therapy for asthma exacerbations, although the benefit of highdose ICS in this setting is not well established. Administration of high-dose ICSs at the onset of acute exacerbation has been performed by some researchers, with mixed results [2]. A systematic review reported a reduction in hospitalizations among children treated with high-dose ICSs who were not receiving SCS within the first hour of an acute asthma exacerbation [3]. In adults, this approach has shown conflicting results [2, 4].
This narrative review aimed to evaluate the benefits of nebulized ICSs for treating or preventing wheezing and asthma exacerbations.
Materials and Methods
We searched for studies published in English, French, Spanish, and Portuguese over the past 25 years in the following databases: PubMed, SciELO, Google Scholar, and the Virtual Health Library. “Search terms included ‘acute asthma,’ ‘asthma exacerbation’, ‘beclomethasone’, ‘budesonide,’ ‘suspension,’ ‘nebulization,’ ‘children OR adolescents.’” The abstracts of the 150 studies found were read, and those deemed relevant were selected. Additional articles identified in the text of other publications were also included in the review.
Results
ICS
To date, eight compounds have been made available worldwide for asthma treatment: beclomethasone dipropionate (BDP), budesonide (BUD), fluticasone propionate (FP), fluticasone furoate, mometasone furoate, ciclesonide, flunisolide, and triamcinolone acetonide. They have distinct biological characteristics and pharmacokinetic and pharmacodynamics properties, and provide similar therapeutic benefits at equipotent doses [2]. However, therapeutic effects and systemic bioavailability vary with the efficiency of the delivery device [2, 5, 6].
Mechanism of action of ICS
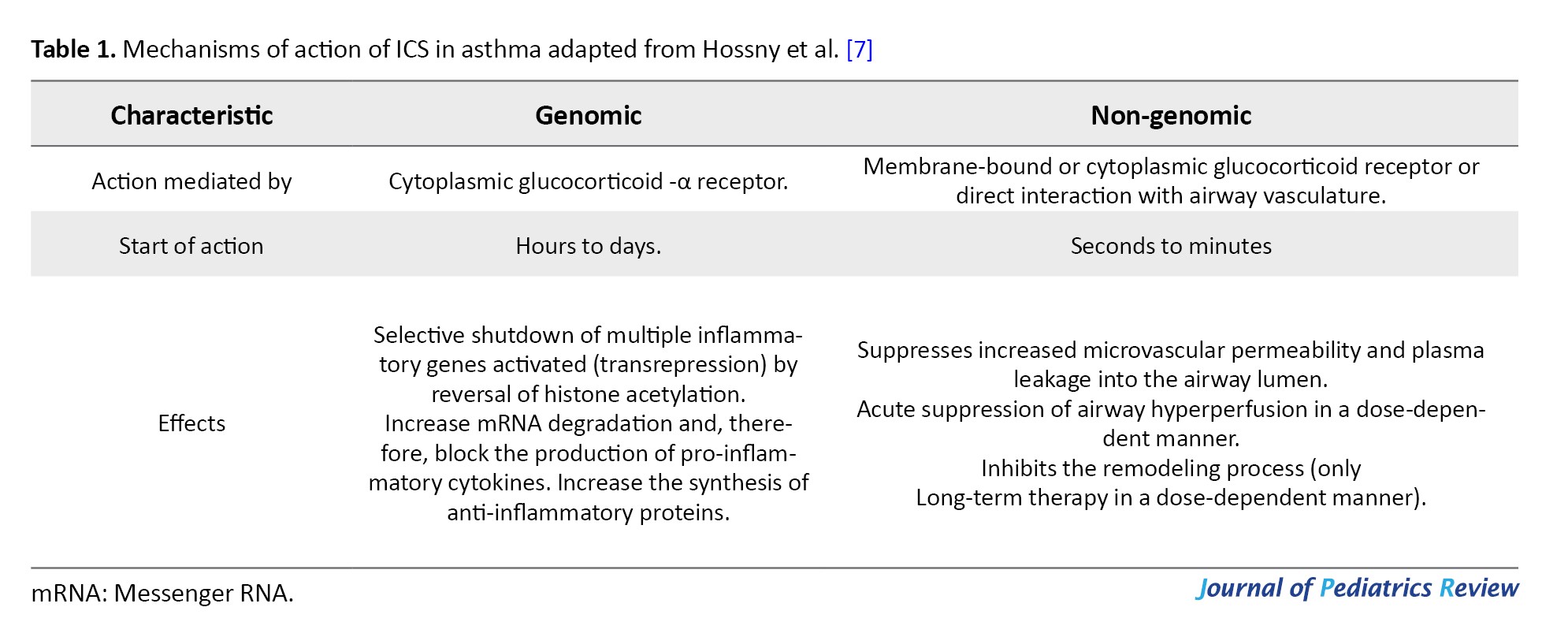
Despite the development of new drugs, ICS remain the main anti-inflammatory agent used in asthma treatment. They reduce inflammation and decrease airway eosinophils, T lymphocytes, and macrophages. Their effects include genomic actions, which develop slowly, and non-genomic actions, which occur rapidly and are exclusive to inhaled formulations. The genomic action occurs after the ICS binds to the glucocorticoid receptor in the cell cytoplasm, penetrates the cell nucleus, and alters gene transcription, inhibiting the synthesis of pro-inflammatory proteins and stimulating the synthesis of anti-inflammatory proteins (Table 1) [7].
Nongenomic actions are less well understood. This mechanism of action initiates by the binding of ICS to cell membrane receptors or by nonspecific interactions with airway cells. The main non-genomic action described is a transient reduction in airway blood flow (Qaw), particularly increased in asthmatics due to local vasodilation and vascular neoformation [7]. The vasoconstrictor action of ICS is secondary to the increased action of norepinephrine on smooth muscle, beginning minutes after drug administration. This mechanism peaks at 30–60 minutes and lasts 90–120 minutes. This action is dose-dependent and observed primarily with high ICS doses. A study with bronchopulmonary dysplasia observed a greater reduction in Qaw (21%) in asthmatics at a dose of 1680 µg [8].
Other non-genomic ICS mechanisms of action have been described. In animal models of allergic asthma, ICS rapidly inhibited mast cell degranulation (in approximately 10 minutes) during histamine-induced bronchoprovocation by reducing intracellular calcium elevation [9]. An ex vivo study documented a rapid relaxation of histamine-precontracted airway muscle cells after exposure to BDP, with greater maximal relaxation in passively sensitized bronchioles (31.9% vs 63.9%), independent of vasoconstriction [10].
Inhalation devices
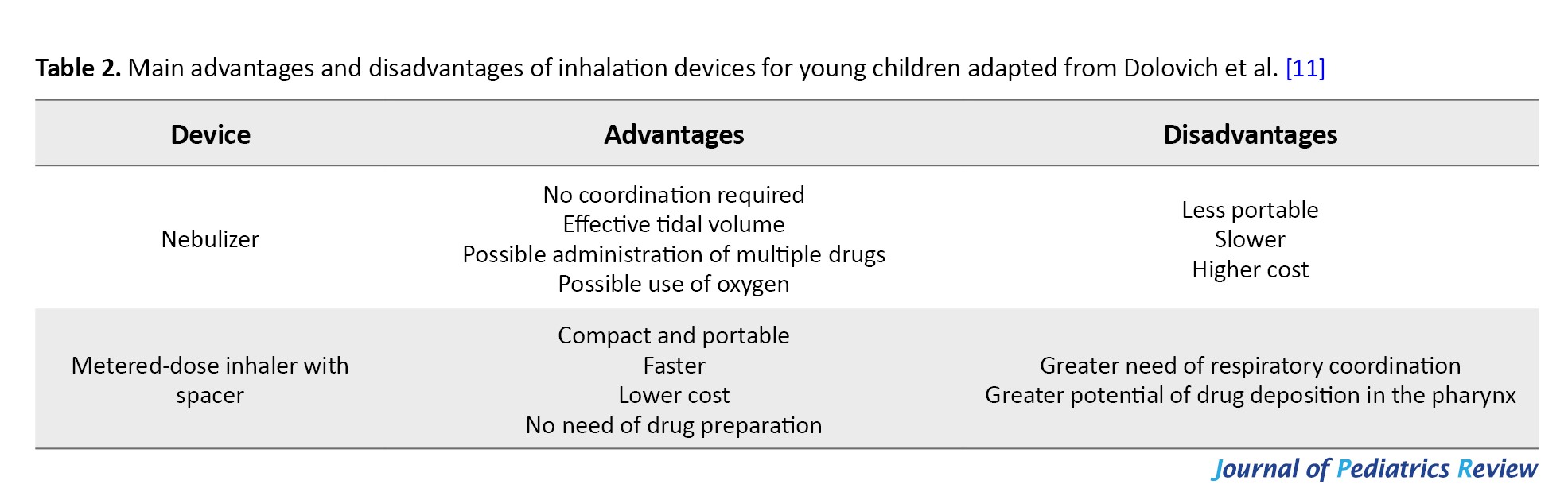
In clinical practice, the choice of inhalation device is a key determinant of treatment success in respiratory diseases, such as asthma. Each type of inhalation device has advantages and disadvantages, and no single device is ideal for all patients. Young children under six years of age cannot adequately use dry powder inhalers. Therefore, pressurized metered-dose inhalers (pMDIs) with a spacer and face mask, and nebulizers are the recommended options [2]. Table 2 presents the main advantages and disadvantages of these devices [11].
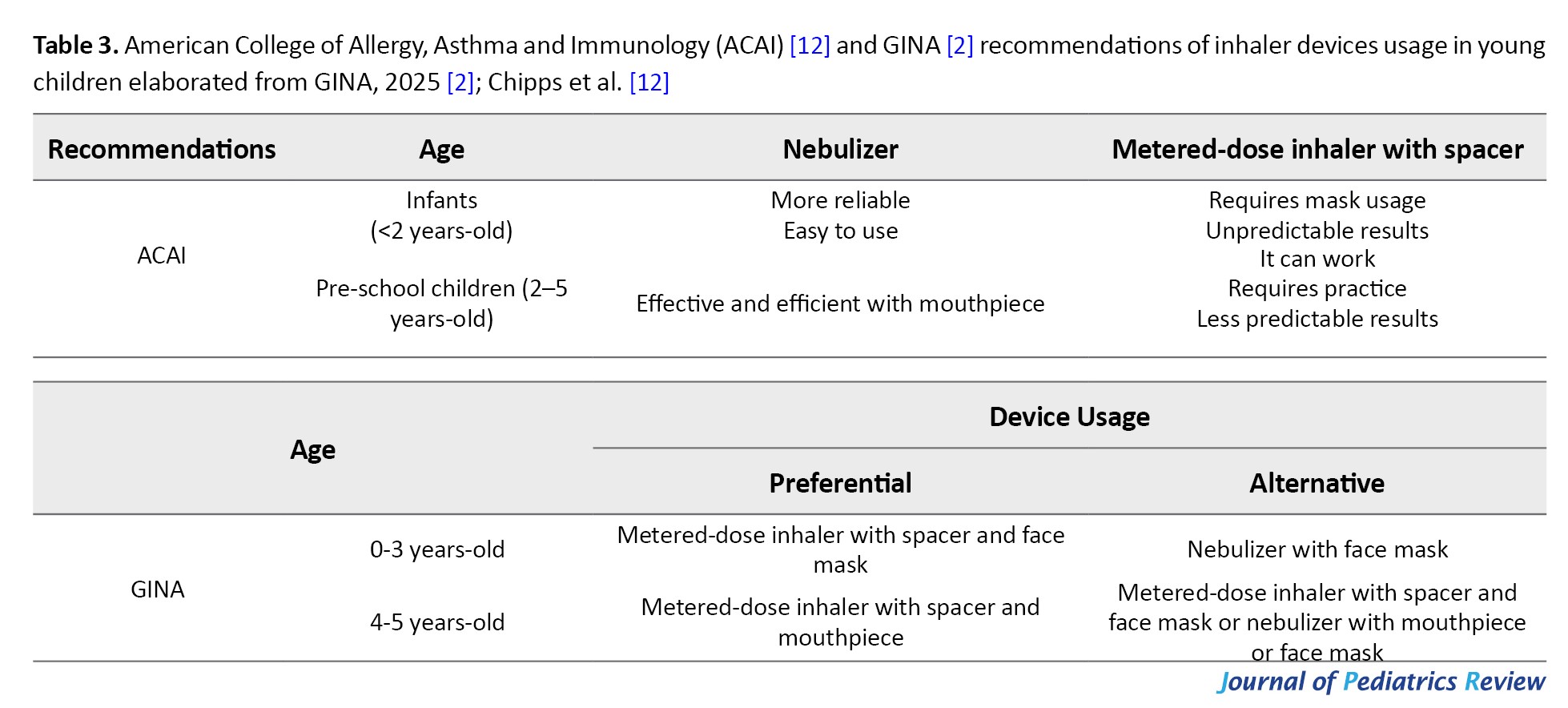
Global initiative for asthma (GINA) recommends pMDI as the preferred device for young children with asthma, and nebulizer as an alternative. Other organizations have different recommendations (Table 3).
Nebulizers
Nebulizers convert solutions or suspensions into aerosols composed of small particles capable of reaching the lower airways [13]. The three main nebulizers are jet, ultrasonic, and vibrating mesh nebulizers. Air-jet nebulizers are the most traditional nebulizers. In jet nebulizers, compressed gas (air or oxygen) creates negative pressure that overcomes liquid surface tension and produces droplets carried by the gas stream [13]. Ultrasonic nebulizers use a vibrating quartz crystal to generate high frequency sound waves that aerosolize the solution [14]. Vibrating mesh nebulizers use an oscillating membrane with uniform conical apertures to generate aerosol [13, 14].
Nebulized medications are typically diluted in saline. For devices with residual volumes greater than 1 mL, a total fill volume of 3–4 mL is recommended; for devices with residual volumes less than 1 mL, 2.0–2.5 mL is preferred [15]. Large fill volumes prolong nebulization time and may cause discomfort in children. Conversely, small volumes increase the proportion of drug retained within the device [13]. In air-jet nebulizers, the airflow provided by the compressor is essential for generating particles suitable for inhalation, with a flow rate typically between 6 and 8 L/min recommended. Air-jet nebulizers are capable of nebulizing solutions and suspensions. Ultrasonic nebulizers should not be used to nebulize suspensions, such as corticosteroids [16].
Nebulizers can be used with a face mask or mouthpiece. Although mouthpiece provide greater lung deposition, they are unsuitable for infants and uncooperative children. Proper mask fit is essential to ensure adequate lung deposition [13].
ICS in asthma exacerbations
The standard treatment of asthma exacerbations in the emergency department is based on the administration of repeated doses of short-acting bronchodilators, supplemental oxygen when it is needed, and SCS [2]. Multiple studies and several meta-analyses have evaluated the effectiveness of high-dose ICS in asthma exacerbations, usually with the goal of preventing hospitalizations. In 2019, Kearns et al. conducted a comprehensive meta-analyses of randomized clinical trials comparing ICS, alone or with SCS, to SCS alone. The analysis included 25 studies (2,733 patients). ICS reduced hospitalization rates by 38% versus SCS and by 27% when added to SCS. Eighteen of the 25 studies evaluated were in children, 13 of which used nebulized ICS. In the evaluation of pediatric studies, a significant reduction was observed in hospitalizations when comparing the combination of ICS and SCS versus SCS (odds ratio [OR], 95% confidence interval [CI]: 0.75 [0.57%, 0.99%]; 4 studies), but no significant difference was found for ICS versus SCS (OR [95% CI]: 0.69 [0.42%, 1.12%]; 6 studies) [17].
A previous metaanalysis of pediatric trials (8 studies, 797 patients) reported no significant differences in hospitalization rates or need for additional therapy between ICS and SCS [18]. A more recent meta analysis evaluating the addition of ICS (nebulized or pMDI) to SCS (oral or parenteral) in children showed no effect on hospitalization rates but demonstrated reduced length of stay (>1 day) and improved severity scores [19].
According to GINA, the use of ICS in high-doses within the first hour of treatment in the emergency department, with or without concomitant SCS, reduces the risk of hospitalization and the need for SCS in children. The addition of ICS is well tolerated, but it is associated with higher treatment costs. However, dose standardization and treatment-duration protocols remain undefined [2]. A systematic review of nebulized ICS for exacerbations included 10 studies using four different ICS regimens, with daily doses ranging from 1000–2400 µg of BUD, 800 µg of BDP, and 2000 µg of FP [20].
ICS for the prevention of asthma exacerbations
Asthma exacerbations are the most morbid event of the disease, responsible for emergency department visits and hospitalizations, and are often treated with SCS, which have potential adverse events [21]. One method already studied to prevent asthma exacerbations in young children without persistent symptoms and, consequently, without regular ICS use, is the intermittent high-dose ICS use. In this treatment modality, high-dose ICS (doses similar to those described in the previous section) are initiated at the onset of respiratory symptoms, usually triggered by viral infections, and continued for 7-10 days. In children younger than six years of age with intermittent or viral asthma, this treatment strategy was able to reduce the progression to asthma exacerbation with SCS use by 35% (95% CI, 19%, 49%), representing the most evidence-supported treatment for children with this symptom profile [22]. Based on the available evidence, GINA has recommended intermittent ICS treatment as an alternative treatment option for steps 1 and 2 in children younger than six years of age for several years [2]. Due to potential adverse effects, such as reduced growth velocity reported with high-dose FP [23], this strategy is recommended only when the family understands the benefit-risk profile [2].
Nebulized BDP
BDP was the first ICS molecule to be tested in the early 1970s. Since then, it has been shown to be effective in reducing the frequency and severity of asthma symptoms, whether administered by nebulizer or pMDI [24]. BDP is mainly available in two administration forms: pMDI and vials for nebulization.
The efficacy and safety of nebulized BDP have been studied and documented in several pediatric studies across different age groups. In infants (6-24 months) with recurrent wheezing, Carlsen et al. compared nebulized BDP 100 μg four times daily with placebo for eight weeks. Infants treated with BDP had significantly fewer respiratory complaints and wheezing episodes during the one-year follow-up [25].
A randomized, double-blind, placebo-controlled study evaluated children (mean age, 10 years of age) with intermittent allergic asthma and associated rhinitis who received nebulized BDP 800 μg daily (with face mask) for four weeks. The BDP group showed significant reduction in exhaled nitric oxide levels and lung function (forced expiratory volume in 1 second [FEV1] and forced vital capacity [FVC]) compared to baseline, as well as significant improvements in cough, respiratory distress, wheezing, and sleep disturbances compared to placebo [26]. Another study evaluated the effects of 800 μg/day of nebulized BDP for 12 weeks in school-aged children with persistent asthma (mean age, 8 years of age) divided into once- or twice-daily treatment. At the end of the study, both treatment groups showed sustained improvement in lung function, in addition to an increase in the number of symptom-free days and nights, as well as in the percentage of children who achieved complete asthma symptom control. There were no significant changes in the urinary cortisol/creatinine ratio during the study period within or between groups [27].
Few studies have directly compared different nebulized ICSs. Delacourt et al. evaluated 130 children (6 months to 6 years) with severe persistent asthma treated with BDP 800 μg/day or BUD 750 μg/day, both administered by nebulization. At the end of the study (14 weeks), there were no differences in the percentage of children who did not experience exacerbations (BDP: 40.4% versus BUD: 51.7%; P=0.28), the number of nights with wheezing, or the consumption of oral steroids. Similarly, both treatments were well tolerated, with no serious adverse events [28]. In older children and adolescents, Terzano et al. evaluated two treatment regimens for mild to moderate persistent asthma for four weeks: BDP 800 μg/day and BUD 1000 μg/day, both nebulized. There were no differences between the treatment regimens regarding improvement in lung function (peak expiratory flow [PEF] and FEV1 or the need for salbutamol as a reliever. Mild adverse events occurred similarly in both groups and did not require treatment discontinuation [29].
The comparison of nebulized BDP with BDP pMDI was evaluated in 151 schoolchildren and adolescents (6–16 years) with asthma. Patients were randomized to receive nebulized BDP (1600 μg/day) or pMDI (800 μg/day) for four weeks. Both groups showed improvement compared to the pretreatment period, and there were no differences between the nebulized or pMDI groups in PEF, symptom scores, or salbutamol use as a reliever [30].
Nebulized BDP in asthma exacerbation
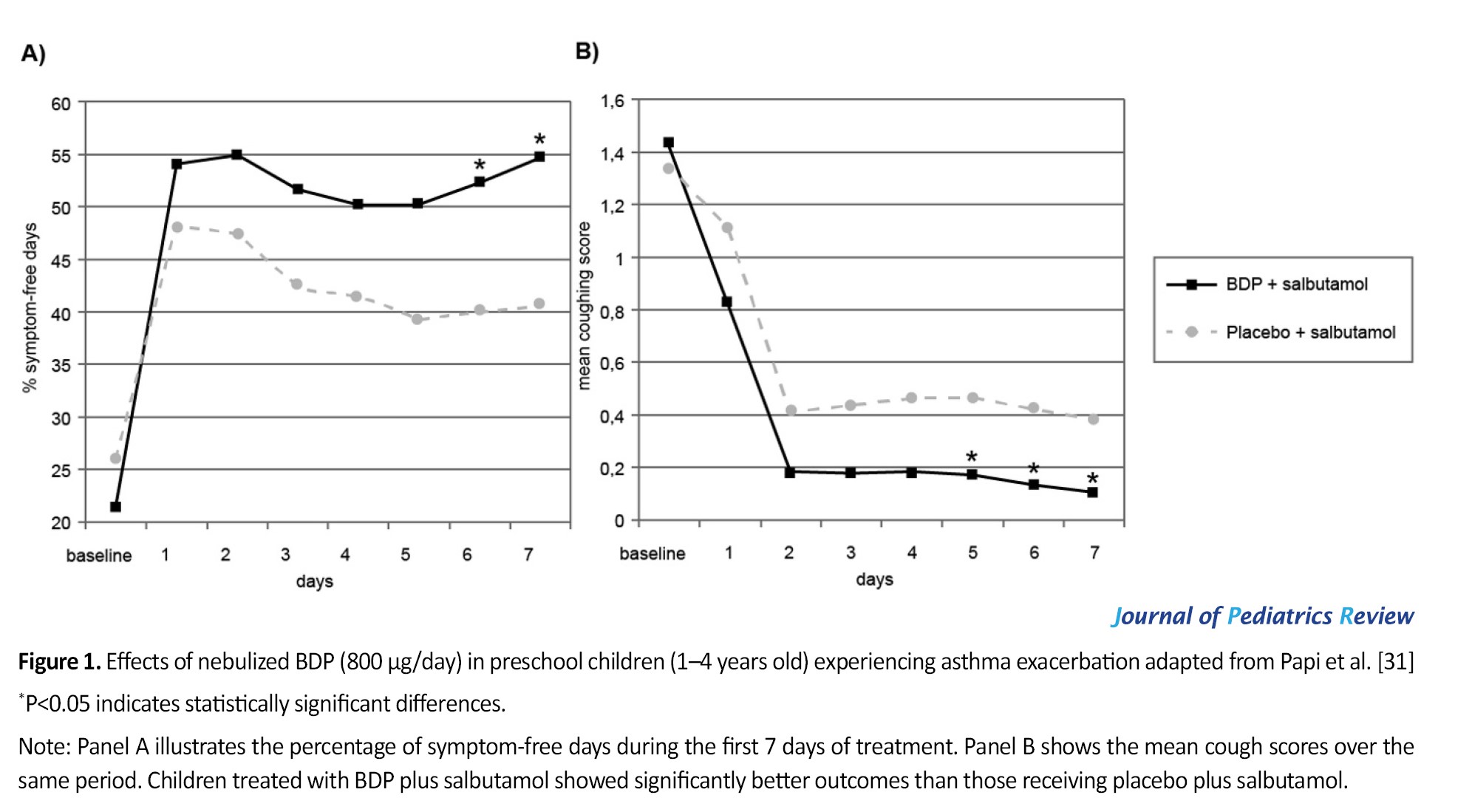
In preschool children, the effect of nebulized BDP in asthma exacerbations was described in a post hoc analysis of a clinical trial. This analysis evaluated the first week of treatment of 166 pre-school children (1-4 years of age) with recurrent wheezing who received nebulized BDP (800 μg/day) or placebo, initiated during a mild to moderate episode of acute wheezing. Those treated with BDP had more symptom-free days (54.7% versus 40.5%; P=0.01) and lower cough scores. For both outcomes, clinical improvement was observed within the first few days of treatment (Figure 1) [31].
 A strategy to prevent asthma exacerbations/wheezing with highdose BDP was evaluated in 26 infants (7-12 months of age) with recurrent wheezing. The infants were divided into two groups: one initiating nebulized BDP 400 μg, three times daily, at the onset of respiratory infection symptoms, and the other group received no preventive treatment. BDP treatment was continued for five days, or stopped earlier, if symptoms subsided for 24 hours. Compared to the control group (placebo), those actively treated experienced fewer wheezing episodes and fewer activity limitations. Emergency department visits were required on five occasions (four in the placebo group), and SCS was initiated in six episodes (four in the placebo group). No adverse effects were reported in children treated with BDP [32]. Evaluating preschool children with persistent wheezing, Papi et al. reported that daily treatment with nebulized BDP (400 μg twice daily) for three months was superior to placebo (only salbutamol if needed) in increasing symptom-free days and preventing wheezing exacerbations. A third group of children treated with the combination of BDP (800 μg) and salbutamol only when needed had a similar primary outcome and several secondary outcomes to those treated daily with BDP [33].
A strategy to prevent asthma exacerbations/wheezing with highdose BDP was evaluated in 26 infants (7-12 months of age) with recurrent wheezing. The infants were divided into two groups: one initiating nebulized BDP 400 μg, three times daily, at the onset of respiratory infection symptoms, and the other group received no preventive treatment. BDP treatment was continued for five days, or stopped earlier, if symptoms subsided for 24 hours. Compared to the control group (placebo), those actively treated experienced fewer wheezing episodes and fewer activity limitations. Emergency department visits were required on five occasions (four in the placebo group), and SCS was initiated in six episodes (four in the placebo group). No adverse effects were reported in children treated with BDP [32]. Evaluating preschool children with persistent wheezing, Papi et al. reported that daily treatment with nebulized BDP (400 μg twice daily) for three months was superior to placebo (only salbutamol if needed) in increasing symptom-free days and preventing wheezing exacerbations. A third group of children treated with the combination of BDP (800 μg) and salbutamol only when needed had a similar primary outcome and several secondary outcomes to those treated daily with BDP [33].
Safety of BDP
In general, the possible adverse effects of ICS are related to the dose, the duration of treatment, and the device used. The most commonly described systemic adverse event in children is reduced growth velocity and adrenal suppression. Reduced bone mineralization and ocular changes, such as cataracts and glaucoma, are associated with the use of SCS or very high doses of ICS [34].
In commercial use for almost 40 years, BDP has demonstrated a good safety profile [24]. It is a prodrug with good local tolerability, rarely associated with local adverse effects such as oropharyngeal candidiasis, dysphonia, or pharyngeal pain [15]. An earlier meta-analysis evaluating 21 studies (810 pediatric patients with asthma) found no evidence of an association between BDP treatment (nebulized or via metered-dose inhaler) and growth deceleration, even at high doses or for long periods [35].
Over the years, clinical studies conducted in the pediatric population have revealed that the nebulized formulation of BDP is not only effective but also well tolerated [26, 28, 30, 31, 33, 36, 37]. Adverse effects induced by nebulized BDP were rare and mild, and few patients required treatment discontinuation. There was no evidence of significant changes in growth, urinary cortisol concentration, or bone metabolism [15].
In a comparative study, the tolerability profile of nebulized BDP (800 µg/day) was similar to that observed with nebulized BUD (750 µg/day) in infants and pre-school children, with no differences in the rate of adverse events or growth. Neither treatment altered bone metabolism or urinary cortisol levels [28]. In another study with pre-school children, both daily and as-needed use of nebulized BDP did not show higher rates of adverse events, treatment-related adverse events, or changes in salivary cortisol compared to the group treated with only as-needed salbutamol [33].
Conclusion
Despite the development of new agents, ICS remain the main anti-inflammatory drugs used in the treatment of asthma. Due to their non-genomic actions, primarily in controlling airway blood flow, they have a rapid onset of action and may contribute to the treatment and prevention of asthma exacerbations. The use of high-dose ICS within the first hour at the emergency department, with or without concomitant SCS, reduces the risk of hospitalization and the need for SCS in children. Nebulization is an effective form of administration of inhaled medications, particularly useful in young children with less training required. The efficacy and safety of nebulized BDP have been studied and documented in several pediatric studies across different age groups.
Ethical Considerations
Compliance with ethical guidelines
This article is a narrative review with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization: Gustavo Wandalsen; Writing the original draft: Gustavo Wandalsen and Dirceu Solé; Review, editing and final approval: All authors.
Conflicts of interest
The authors declared no conflict of interest.
References
Inhaled corticosteroids (ICS) are the most effective anti-inflammatory agents for long-term asthma management, and their beneficial therapeutic effects are directly related to the reduction of airway inflammation [1]. Regular use reduces symptoms, exacerbations and hospitalizations, improve quality of life and lung function, and reduce asthma-related deaths [2].
Asthma exacerbations are acute or subacute episodes of worsening symptoms and lung function. Asthma exacerbations are responsible for numerous emergency department visits, hospitalizations, and use of systemic corticosteroids (SCS) [2]. SCS remain the standard therapy for asthma exacerbations, although the benefit of highdose ICS in this setting is not well established. Administration of high-dose ICSs at the onset of acute exacerbation has been performed by some researchers, with mixed results [2]. A systematic review reported a reduction in hospitalizations among children treated with high-dose ICSs who were not receiving SCS within the first hour of an acute asthma exacerbation [3]. In adults, this approach has shown conflicting results [2, 4].
This narrative review aimed to evaluate the benefits of nebulized ICSs for treating or preventing wheezing and asthma exacerbations.
Materials and Methods
We searched for studies published in English, French, Spanish, and Portuguese over the past 25 years in the following databases: PubMed, SciELO, Google Scholar, and the Virtual Health Library. “Search terms included ‘acute asthma,’ ‘asthma exacerbation’, ‘beclomethasone’, ‘budesonide,’ ‘suspension,’ ‘nebulization,’ ‘children OR adolescents.’” The abstracts of the 150 studies found were read, and those deemed relevant were selected. Additional articles identified in the text of other publications were also included in the review.
Results
ICS
To date, eight compounds have been made available worldwide for asthma treatment: beclomethasone dipropionate (BDP), budesonide (BUD), fluticasone propionate (FP), fluticasone furoate, mometasone furoate, ciclesonide, flunisolide, and triamcinolone acetonide. They have distinct biological characteristics and pharmacokinetic and pharmacodynamics properties, and provide similar therapeutic benefits at equipotent doses [2]. However, therapeutic effects and systemic bioavailability vary with the efficiency of the delivery device [2, 5, 6].
Mechanism of action of ICS
Despite the development of new drugs, ICS remain the main anti-inflammatory agent used in asthma treatment. They reduce inflammation and decrease airway eosinophils, T lymphocytes, and macrophages. Their effects include genomic actions, which develop slowly, and non-genomic actions, which occur rapidly and are exclusive to inhaled formulations. The genomic action occurs after the ICS binds to the glucocorticoid receptor in the cell cytoplasm, penetrates the cell nucleus, and alters gene transcription, inhibiting the synthesis of pro-inflammatory proteins and stimulating the synthesis of anti-inflammatory proteins (Table 1) [7].
Nongenomic actions are less well understood. This mechanism of action initiates by the binding of ICS to cell membrane receptors or by nonspecific interactions with airway cells. The main non-genomic action described is a transient reduction in airway blood flow (Qaw), particularly increased in asthmatics due to local vasodilation and vascular neoformation [7]. The vasoconstrictor action of ICS is secondary to the increased action of norepinephrine on smooth muscle, beginning minutes after drug administration. This mechanism peaks at 30–60 minutes and lasts 90–120 minutes. This action is dose-dependent and observed primarily with high ICS doses. A study with bronchopulmonary dysplasia observed a greater reduction in Qaw (21%) in asthmatics at a dose of 1680 µg [8].
Other non-genomic ICS mechanisms of action have been described. In animal models of allergic asthma, ICS rapidly inhibited mast cell degranulation (in approximately 10 minutes) during histamine-induced bronchoprovocation by reducing intracellular calcium elevation [9]. An ex vivo study documented a rapid relaxation of histamine-precontracted airway muscle cells after exposure to BDP, with greater maximal relaxation in passively sensitized bronchioles (31.9% vs 63.9%), independent of vasoconstriction [10].
Inhalation devices
In clinical practice, the choice of inhalation device is a key determinant of treatment success in respiratory diseases, such as asthma. Each type of inhalation device has advantages and disadvantages, and no single device is ideal for all patients. Young children under six years of age cannot adequately use dry powder inhalers. Therefore, pressurized metered-dose inhalers (pMDIs) with a spacer and face mask, and nebulizers are the recommended options [2]. Table 2 presents the main advantages and disadvantages of these devices [11].
Global initiative for asthma (GINA) recommends pMDI as the preferred device for young children with asthma, and nebulizer as an alternative. Other organizations have different recommendations (Table 3).
Nebulizers
Nebulizers convert solutions or suspensions into aerosols composed of small particles capable of reaching the lower airways [13]. The three main nebulizers are jet, ultrasonic, and vibrating mesh nebulizers. Air-jet nebulizers are the most traditional nebulizers. In jet nebulizers, compressed gas (air or oxygen) creates negative pressure that overcomes liquid surface tension and produces droplets carried by the gas stream [13]. Ultrasonic nebulizers use a vibrating quartz crystal to generate high frequency sound waves that aerosolize the solution [14]. Vibrating mesh nebulizers use an oscillating membrane with uniform conical apertures to generate aerosol [13, 14].
Nebulized medications are typically diluted in saline. For devices with residual volumes greater than 1 mL, a total fill volume of 3–4 mL is recommended; for devices with residual volumes less than 1 mL, 2.0–2.5 mL is preferred [15]. Large fill volumes prolong nebulization time and may cause discomfort in children. Conversely, small volumes increase the proportion of drug retained within the device [13]. In air-jet nebulizers, the airflow provided by the compressor is essential for generating particles suitable for inhalation, with a flow rate typically between 6 and 8 L/min recommended. Air-jet nebulizers are capable of nebulizing solutions and suspensions. Ultrasonic nebulizers should not be used to nebulize suspensions, such as corticosteroids [16].
Nebulizers can be used with a face mask or mouthpiece. Although mouthpiece provide greater lung deposition, they are unsuitable for infants and uncooperative children. Proper mask fit is essential to ensure adequate lung deposition [13].
ICS in asthma exacerbations
The standard treatment of asthma exacerbations in the emergency department is based on the administration of repeated doses of short-acting bronchodilators, supplemental oxygen when it is needed, and SCS [2]. Multiple studies and several meta-analyses have evaluated the effectiveness of high-dose ICS in asthma exacerbations, usually with the goal of preventing hospitalizations. In 2019, Kearns et al. conducted a comprehensive meta-analyses of randomized clinical trials comparing ICS, alone or with SCS, to SCS alone. The analysis included 25 studies (2,733 patients). ICS reduced hospitalization rates by 38% versus SCS and by 27% when added to SCS. Eighteen of the 25 studies evaluated were in children, 13 of which used nebulized ICS. In the evaluation of pediatric studies, a significant reduction was observed in hospitalizations when comparing the combination of ICS and SCS versus SCS (odds ratio [OR], 95% confidence interval [CI]: 0.75 [0.57%, 0.99%]; 4 studies), but no significant difference was found for ICS versus SCS (OR [95% CI]: 0.69 [0.42%, 1.12%]; 6 studies) [17].
A previous metaanalysis of pediatric trials (8 studies, 797 patients) reported no significant differences in hospitalization rates or need for additional therapy between ICS and SCS [18]. A more recent meta analysis evaluating the addition of ICS (nebulized or pMDI) to SCS (oral or parenteral) in children showed no effect on hospitalization rates but demonstrated reduced length of stay (>1 day) and improved severity scores [19].
According to GINA, the use of ICS in high-doses within the first hour of treatment in the emergency department, with or without concomitant SCS, reduces the risk of hospitalization and the need for SCS in children. The addition of ICS is well tolerated, but it is associated with higher treatment costs. However, dose standardization and treatment-duration protocols remain undefined [2]. A systematic review of nebulized ICS for exacerbations included 10 studies using four different ICS regimens, with daily doses ranging from 1000–2400 µg of BUD, 800 µg of BDP, and 2000 µg of FP [20].
ICS for the prevention of asthma exacerbations
Asthma exacerbations are the most morbid event of the disease, responsible for emergency department visits and hospitalizations, and are often treated with SCS, which have potential adverse events [21]. One method already studied to prevent asthma exacerbations in young children without persistent symptoms and, consequently, without regular ICS use, is the intermittent high-dose ICS use. In this treatment modality, high-dose ICS (doses similar to those described in the previous section) are initiated at the onset of respiratory symptoms, usually triggered by viral infections, and continued for 7-10 days. In children younger than six years of age with intermittent or viral asthma, this treatment strategy was able to reduce the progression to asthma exacerbation with SCS use by 35% (95% CI, 19%, 49%), representing the most evidence-supported treatment for children with this symptom profile [22]. Based on the available evidence, GINA has recommended intermittent ICS treatment as an alternative treatment option for steps 1 and 2 in children younger than six years of age for several years [2]. Due to potential adverse effects, such as reduced growth velocity reported with high-dose FP [23], this strategy is recommended only when the family understands the benefit-risk profile [2].
Nebulized BDP
BDP was the first ICS molecule to be tested in the early 1970s. Since then, it has been shown to be effective in reducing the frequency and severity of asthma symptoms, whether administered by nebulizer or pMDI [24]. BDP is mainly available in two administration forms: pMDI and vials for nebulization.
The efficacy and safety of nebulized BDP have been studied and documented in several pediatric studies across different age groups. In infants (6-24 months) with recurrent wheezing, Carlsen et al. compared nebulized BDP 100 μg four times daily with placebo for eight weeks. Infants treated with BDP had significantly fewer respiratory complaints and wheezing episodes during the one-year follow-up [25].
A randomized, double-blind, placebo-controlled study evaluated children (mean age, 10 years of age) with intermittent allergic asthma and associated rhinitis who received nebulized BDP 800 μg daily (with face mask) for four weeks. The BDP group showed significant reduction in exhaled nitric oxide levels and lung function (forced expiratory volume in 1 second [FEV1] and forced vital capacity [FVC]) compared to baseline, as well as significant improvements in cough, respiratory distress, wheezing, and sleep disturbances compared to placebo [26]. Another study evaluated the effects of 800 μg/day of nebulized BDP for 12 weeks in school-aged children with persistent asthma (mean age, 8 years of age) divided into once- or twice-daily treatment. At the end of the study, both treatment groups showed sustained improvement in lung function, in addition to an increase in the number of symptom-free days and nights, as well as in the percentage of children who achieved complete asthma symptom control. There were no significant changes in the urinary cortisol/creatinine ratio during the study period within or between groups [27].
Few studies have directly compared different nebulized ICSs. Delacourt et al. evaluated 130 children (6 months to 6 years) with severe persistent asthma treated with BDP 800 μg/day or BUD 750 μg/day, both administered by nebulization. At the end of the study (14 weeks), there were no differences in the percentage of children who did not experience exacerbations (BDP: 40.4% versus BUD: 51.7%; P=0.28), the number of nights with wheezing, or the consumption of oral steroids. Similarly, both treatments were well tolerated, with no serious adverse events [28]. In older children and adolescents, Terzano et al. evaluated two treatment regimens for mild to moderate persistent asthma for four weeks: BDP 800 μg/day and BUD 1000 μg/day, both nebulized. There were no differences between the treatment regimens regarding improvement in lung function (peak expiratory flow [PEF] and FEV1 or the need for salbutamol as a reliever. Mild adverse events occurred similarly in both groups and did not require treatment discontinuation [29].
The comparison of nebulized BDP with BDP pMDI was evaluated in 151 schoolchildren and adolescents (6–16 years) with asthma. Patients were randomized to receive nebulized BDP (1600 μg/day) or pMDI (800 μg/day) for four weeks. Both groups showed improvement compared to the pretreatment period, and there were no differences between the nebulized or pMDI groups in PEF, symptom scores, or salbutamol use as a reliever [30].
Nebulized BDP in asthma exacerbation
In preschool children, the effect of nebulized BDP in asthma exacerbations was described in a post hoc analysis of a clinical trial. This analysis evaluated the first week of treatment of 166 pre-school children (1-4 years of age) with recurrent wheezing who received nebulized BDP (800 μg/day) or placebo, initiated during a mild to moderate episode of acute wheezing. Those treated with BDP had more symptom-free days (54.7% versus 40.5%; P=0.01) and lower cough scores. For both outcomes, clinical improvement was observed within the first few days of treatment (Figure 1) [31].
Safety of BDP
In general, the possible adverse effects of ICS are related to the dose, the duration of treatment, and the device used. The most commonly described systemic adverse event in children is reduced growth velocity and adrenal suppression. Reduced bone mineralization and ocular changes, such as cataracts and glaucoma, are associated with the use of SCS or very high doses of ICS [34].
In commercial use for almost 40 years, BDP has demonstrated a good safety profile [24]. It is a prodrug with good local tolerability, rarely associated with local adverse effects such as oropharyngeal candidiasis, dysphonia, or pharyngeal pain [15]. An earlier meta-analysis evaluating 21 studies (810 pediatric patients with asthma) found no evidence of an association between BDP treatment (nebulized or via metered-dose inhaler) and growth deceleration, even at high doses or for long periods [35].
Over the years, clinical studies conducted in the pediatric population have revealed that the nebulized formulation of BDP is not only effective but also well tolerated [26, 28, 30, 31, 33, 36, 37]. Adverse effects induced by nebulized BDP were rare and mild, and few patients required treatment discontinuation. There was no evidence of significant changes in growth, urinary cortisol concentration, or bone metabolism [15].
In a comparative study, the tolerability profile of nebulized BDP (800 µg/day) was similar to that observed with nebulized BUD (750 µg/day) in infants and pre-school children, with no differences in the rate of adverse events or growth. Neither treatment altered bone metabolism or urinary cortisol levels [28]. In another study with pre-school children, both daily and as-needed use of nebulized BDP did not show higher rates of adverse events, treatment-related adverse events, or changes in salivary cortisol compared to the group treated with only as-needed salbutamol [33].
Conclusion
Despite the development of new agents, ICS remain the main anti-inflammatory drugs used in the treatment of asthma. Due to their non-genomic actions, primarily in controlling airway blood flow, they have a rapid onset of action and may contribute to the treatment and prevention of asthma exacerbations. The use of high-dose ICS within the first hour at the emergency department, with or without concomitant SCS, reduces the risk of hospitalization and the need for SCS in children. Nebulization is an effective form of administration of inhaled medications, particularly useful in young children with less training required. The efficacy and safety of nebulized BDP have been studied and documented in several pediatric studies across different age groups.
Ethical Considerations
Compliance with ethical guidelines
This article is a narrative review with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization: Gustavo Wandalsen; Writing the original draft: Gustavo Wandalsen and Dirceu Solé; Review, editing and final approval: All authors.
Conflicts of interest
The authors declared no conflict of interest.
References
- Axelsson I, Naumburg E, Prietsch SO, Zhang L. Inhaled corticosteroids in children with persistent asthma: Effects of different drugs and delivery devices on growth. Cochrane Database Syst Rev. 2019; 6(6):CD010126. [DOI:10.1002/14651858.CD010126.pub2] [PMID]
- Global Strategy for Asthma. Management and Prevention. Global Initiative for Asthma - GINA [Internet]. 2025 [Updated 2025 May 12]. Available from: [Link]
- Edmonds ML, Milan SJ, Camargo CA Jr, Pollack CV, Rowe BH. Early use of inhaled corticosteroids in the emergency department treatment of acute asthma. Cochrane Database Syst Rev. 2012; 12(12):CD002308. [DOI:10.1002/14651858.CD002308.pub2] [PMID]
- Ratto D, Alfaro C, Sipsey J, Glovsky MM, Sharma OP. Are intravenous corticosteroids required in status asthmaticus? JAMA. 1988; 260(4):527-9. [PMID]
- Borghardt JM, Kloft C, Sharma A. Inhaled therapy in respiratory disease: The complex interplay of pulmonary kinetic processes. Can Respir J. 2018; 2018:2732017.[DOI:10.1155/2018/2732017] [PMID]
- Rossi G, Cerasoli F, Cazzola M. Safety of inhaled corticosteroids: Room for improvement. Pulm Pharmacol Ther. 2007; 20(1):23-35. [DOI:10.1016/j.pupt.2005.10.008] [PMID]
- Hossny E, Rosario N, Lee BW, Singh M, El-Ghoneimy D, Soh JY, et al. The use of inhaled corticosteroids in pediatric asthma: update. World Allergy Organ J. 2016; 9:26.[DOI:10.1186/s40413-016-0117-0] [PMID]
- Mendes ES, Pereira A, Danta I, Duncan RC, Wanner A. Comparative bronchial vasoconstrictive efficacy of inhaled glucocorticosteroids. Eur Respir J. 2003; 21(6):989-93. [DOI:10.1183/09031936.03.00072402] [PMID]
- Zhou J, Liu DF, Liu C, Kang ZM, Shen XH, Chen YZ, et al. Glucocorticoids inhibit degranulation of mast cells in allergic asthma via nongenomic mechanism. Allergy. 2008; 63(9):1177-85. [DOI:10.1111/j.1398-9995.2008.01725.x] [PMID]
- Cazzola M, Calzetta L, Rogliani P, Puxeddu E, Facciolo F, Matera MG. Interaction between corticosteroids and muscarinic antagonists in human airways. Pulm Pharmacol Ther. 2016; 36:1-9. [DOI:10.1016/j.pupt.2015.11.004] [PMID]
- Dolovich MB, Ahrens RC, Hess DR, Anderson P, Dhand R, Rau JL, et al. Device selection and outcomes of aerosol therapy: Evidence-based guidelines: American College of Chest Physicians/American college of asthma, allergy, and immunology. Chest. 2005; 127(1):335-71. [DOI:10.1378/chest.127.1.335] [PMID]
- Chipps BE, Bacharier LB, Farrar JR, Jackson DJ, Murphy KR, Phipatanakul W, et al. The pediatric asthma yardstick: Practical recommendations for a sustained step-up in asthma therapy for children with inadequately controlled asthma. Ann Allergy Asthma Immunol. 2018; 120(6):559-79.e11 [DOI:10.1016/j.anai.2018.04.002] [PMID]
- Hess DR. Aerosol delivery devices in the treatment of asthma. Respir Care. 2008; 53(6):699-723. [PMID]
- Aguiar R, Lopes A, Ornelas C, Ferreira R, Caiado J, Mendes A, et al. [Inhalation therapy: Inhalation techniques and inhalation devices (Portuguese)]. Rev Port Imunoalergologia. 2017; 25(1):9-26. [Link]
- Nicolini G, Cremonesi G, Melani AS. Inhaled corticosteroid therapy with nebulized beclometasone dipropionate. Pulm Pharmacol Ther. 2010; 23(3):145-55. [DOI:10.1016/j.pupt.2009.11.003] [PMID]
- Boe J, Dennis JH, O'Driscoll BR, Bauer TT, Carone M, Dautzenberg B, et al. European respiratory society guidelines on the use of nebulizers. Eur Respir J. 2001; 18(1):228-42. [DOI:10.1183/09031936.01.00220001] [PMID]
- Kearns N, Maijers I, Harper J, Beasley R, Weatherall M. Inhaled corticosteroids in acute asthma: A systemic review and meta-analysis. J Allergy Clin Immunol Pract. 2020; 8(2):605-17.e6. [DOI:10.1016/j.jaip.2019.08.051] [PMID]
- Beckhaus AA, Riutort MC, Castro-Rodriguez JA. Inhaled versus systemic corticosteroids for acute asthma in children. A systematic review. Pediatr Pulmonol. 2014; 49(4):326-34.[DOI:10.1002/ppul.22846] [PMID]
- Castro-Rodriguez JA, Pincheira MA, Escobar-Serna DP, Sossa-Briceño MP, Rodriguez-Martinez CE. Adding nebulized corticosteroids to systemic corticosteroids for acute asthma in children: A systematic review with meta-analysis. Pediatr Pulmonol. 2020; 55(10):2508-17. [DOI:10.1002/ppul.24956] [PMID]
- Murphy K, Hong J, Wandalsen G, Larenas-Linnemann D, El Beleidy A, Zaytseva O, et al. Nebulized inhaled corticosteroids in asthma treatment in children 5 years or younger: A systematic review and global expert analysis. J Allergy Clin Immunol Pract. 2020; 8(6):1815-27. [DOI:10.1016/j.jaip.2020.01.042] [PMID]
- Jackson DJ, Bacharier LB. Inhaled corticosteroids for the prevention of asthma exacerbations.Ann Allergy Asthma Immunol. 2021; 127(5):524-29. [DOI:10.1016/j.anai.2021.08.014] [PMID]
- Kaiser SV, Huynh T, Bacharier LB, Rosenthal JL, Bakel LA, Parkin PC, et al. Preventing exacerbations in preschoolers with recurrent wheeze: A meta-analysis. Pediatrics. 2016; 137(6):e20154496. [DOI:10.1542/peds.2015-4496] [PMID]
- Ducharme FM, Lemire C, Noya FJ, Davis GM, Alos N, Leblond H, et al. Preemptive use of high-dose fluticasone for virus-induced wheezing in young children. N Engl J Med. 2009; 360(4):339-53. [DOI:10.1056/NEJMoa0808907] [PMID]
- Tosca M, Rossi GA. [Beclomethasone dipropionate: efficacy and safety of the administration by nebulization (Italian)]. Recenti Prog Med. 2022; 113:1-12.[DOI:10.1701/3937.39206] [PMID]
- Carlsen KH, Leegaard J, Larsen S, Orstavik I. Nebulised beclomethasone dipropionate in recurrent obstructive episodes after acute bronchiolitis. Arch Dis Child. 1988; 63(12):1428-33. [DOI:10.1136/adc.63.12.1428] [PMID]
- Profita M, Riccobono L, Bonanno A, Chanez P, Gagliardo R, Montalbano AM, et al. Effect of nebulized beclomethasone on airway inflammation and clinical status of children with allergic asthma and rhinitis: A randomized, double-blind, placebo-controlled study. Int Arch Allergy Immunol. 2013; 161(1):53-64. [DOI:10.1159/000343137] [PMID]
- La Grutta S, Nicolini G, Capristo C, Bellodi SC, Rossi GA. Once daily nebulized beclomethasone is effective in maintaining pulmonary function and improving symptoms in asthmatic children. Monaldi Arch Chest Dis. 2007; 67(1):30-8.[DOI:10.4081/monaldi.2007.507] [PMID]
- Delacourt C, Dutau G, Lefrançois G, Clerson P; Beclospin Clinical Development Group. Comparison of the efficacy and safety of nebulized beclometasone dipropionate and budesonide in severe persistent childhood asthma. Respir Med. 2003; 97(Suppl B):S27-33. [DOI:10.1016/S0954-6111(03)90075-8]
- Terzano C, Allegra L, Barkai L, Cremonesi G. Beclomethasone dipropionate versus budesonide inhalation suspension in children with mild to moderate persistent asthma. Eur Rev Med Pharmacol Sci. 2001; 5(1):17-24. [PMID]
- Bisca N, Cernatescu I, Dragomir D, Iacomi A, Mirceau M, Orascanu D. Comparison of the efficacy and safety of beclometasone dipropionate suspension for nebulization and beclometasone dipropionate via a metered dose inhaler in paediatric patients with moderate to severe exacerbation of asthma. Respir Med. 2003; 97(Suppl. B):S15-20. [DOI:10.1016/S0954-6111(03)90073-4]
- Papi A, Nicolini G, Boner AL, Baraldi E, Cutrera R, Fabbri LM, et al. Short term efficacy of nebulized beclomethasone in mild-to-moderate wheezing episodes in pre-school children. Ital J Pediatr. 2011; 37:39. [DOI:10.1186/1824-7288-37-39] [PMID]
- Ghirga G, Ghirga P, Fagioli S, Colaiacomo M. Intermittent treatment with high dose nebulized beclomethasone for recurrent wheezing in infants due to upper respiratory tract infection. Minerva Pediatr. 2002; 54(3):217-20. [PMID]
- Papi A, Nicolini G, Baraldi E, Boner AL, Cutrera R, Rossi GA, et al. Regular vs prn nebulized treatment in wheeze preschool children. Allergy. 2009;64(10):1463-71. [DOI:10.1111/j.1398-9995.2009.02134.x] [PMID]
- Dahl R. Systemic side effects of inhaled corticosteroids in patients with asthma. Respir Med. 2006; 100(8):1307-17.[DOI:10.1016/j.rmed.2005.11.020] [PMID]
- Allen D, Mullen M, Mullen B. A meta-analysis of the effect of oral and inhaled corticosteroids on growth. J Allergy Clin Immunol. 1994; 93(6):967-76. [DOI:10.1016/S0091-6749(94)70043-5] [PMID]
- Freigang B, Ashford DR. Adrenal cortical function after long-term beclomethasone aerosol therapy in early childhood. Ann Allergy. 1990; 64(4):342-4. [PMID]
- Storr J, Lenney CA, Lenney W. Nebulised beclomethasone dipropionate in preschool asthma. Arch Dis Child. 1986; 61(3):270-3. [DOI:10.1136/adc.61.3.270] [PMID]
Type of Study: Narrative Review |
Subject:
Pediatric Pulmonology
Received: 2025/10/7 | Accepted: 2026/04/12 | Published: 2026/04/12
Received: 2025/10/7 | Accepted: 2026/04/12 | Published: 2026/04/12
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
