
Tue, Jun 9, 2026


Volume 14, Issue 1 (1-2026)
J. Pediatr. Rev 2026, 14(1): 29-36 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Yadolahi B, Sadri L, Taghian M. Efficacy of Mucoadhesive Patch Systems for Topical Anesthesia in Pediatric Dentistry: A Systematic Review. J. Pediatr. Rev 2026; 14 (1) :29-36
URL: http://jpr.mazums.ac.ir/article-1-809-en.html
URL: http://jpr.mazums.ac.ir/article-1-809-en.html



1- Student Research Committee, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran.
2- Department of Pediatric Dentistry, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran.
3- Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran. ,behrad.ydl79@gmail.com
2- Department of Pediatric Dentistry, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran.
3- Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran. ,
Full-Text [PDF 575 kb]
(194 Downloads)
| Abstract (HTML) (478 Views)
Full-Text: (231 Views)
Introduction
Despite continuous progress in dental care and pain control techniques, dental anxiety remains a major challenge for clinicians and patients alike [1]. Local anesthetics are the most commonly used method for managing pain during dental procedures; however, needle phobia persists as a significant concern among both children and adults [1-3]. This fear frequently leads to poor cooperation, complicating both anesthetic administration and the overall treatment process [2-5]. To reduce the discomfort associated with injections, topical anesthetics are commonly applied before needle insertion [4, 6].
Delivering medications through the oral mucosa offers a convenient and non-invasive route of administration. However, this method is challenged by factors such as the constant presence of saliva, which can dilute the drug, and the inherent barrier function of mucosal tissue, which limits drug absorption and permeability. Mucoadhesive formulations that adhere to the mucosal surface can enhance absorption by maintaining higher local drug concentrations at the application site [7]. The use of biopolymers as delivery matrices provides a controlled-release mechanism for therapeutic agents and can be formulated into hydrogels, mucoadhesive films, or patches [8]. These mucoadhesive polymers attach firmly to oral tissues. As the polymer matrix gradually degrades, it enables sustained, controlled drug release over time [9].
In 1996, the U.S. Food and Drug Administration (FDA) approved DentiPatch™, the first transoral lidocaine delivery system designed to provide topical anesthesia and minimize discomfort during dental injections and soft-tissue procedures. Each patch contains 41.6 mg of lidocaine within a 2 cm² adhesive matrix, coated with a polyester backing, and provides effective anesthesia in approximately 2.5 minutes, according to the manufacturer. Clinical trials have verified its safety and efficacy in both adult and pediatric populations, although some studies have reported issues related to inadequate adhesion to the mucosal surface [8].
Accordingly, this systematic review aims to assess the effectiveness and safety of mucoadhesive anesthetic systems compared with conventional local anesthetics in pediatric dentistry.
Materials and Methods
Protocol and registration
This study followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. The literature search strategy was developed according to the problem, intervention or exposure, comparison or control (PICO) framework, defining: Population (P), children undergoing dental procedures; intervention (I), application of topical mucoadhesive anesthetic agents; comparison (C), conventional topical anesthetic agents; and outcome (O), effectiveness of anesthesia.
Children requiring local anesthetic injections were included in the selected studies. In the intervention groups, mucoadhesive topical anesthetics were applied to the mucosal area before the injection. In contrast, control groups received traditional topical agents such as EMLA, benzocaine, or lidocaine before anesthetic administration.
To identify and compare relevant studies on mucoadhesive topical anesthesia, two independent reviewers conducted a comprehensive search of English-language articles published between January 1, 2015, and September 15, 2025, across major databases, including PubMed, Scopus, Web of Science, and the Cochrane Library. Search terms were initially refined using the Medical Subject Headings (MeSH) database, and final keywords included pediatric dentistry, dental patch, topical patch, oral patch, and children. Additionally, a manual search was conducted on Google Scholar using the same keywords to ensure comprehensive coverage of the literature. Last search date: (August 1, September 15, 2025).
Search strategy
The search strategy used the following keywords and operators: (“Pediatric dentistry” [Title/Abstract] Or “pediatric dentistry” [MeSH Terms]) AND (“dental patch” [Title/Abstract] OR “topical patch” [Title/Abstract] OR “oral patch” [Title/Abstract]) AND (“children” [Title/Abstract]) AND (“2015/01/01” [PDAT]: “2025/09/15” [PDAT]) AND English [language].
Eligibility criteria
Randomized controlled trials (RCTs) published in English that involved the application of mucoadhesive topical anesthesia before local anesthetic injection were included in this review. To maintain strict adherence to the PICO framework, only pediatric dentistry studies were prioritized.
The exclusion criteria comprised non-randomized or non-controlled clinical studies, comparative studies without randomization, technical reports, case studies, narrative and systematic reviews, in vitro research, non-English publications, and studies lacking full-text availability.
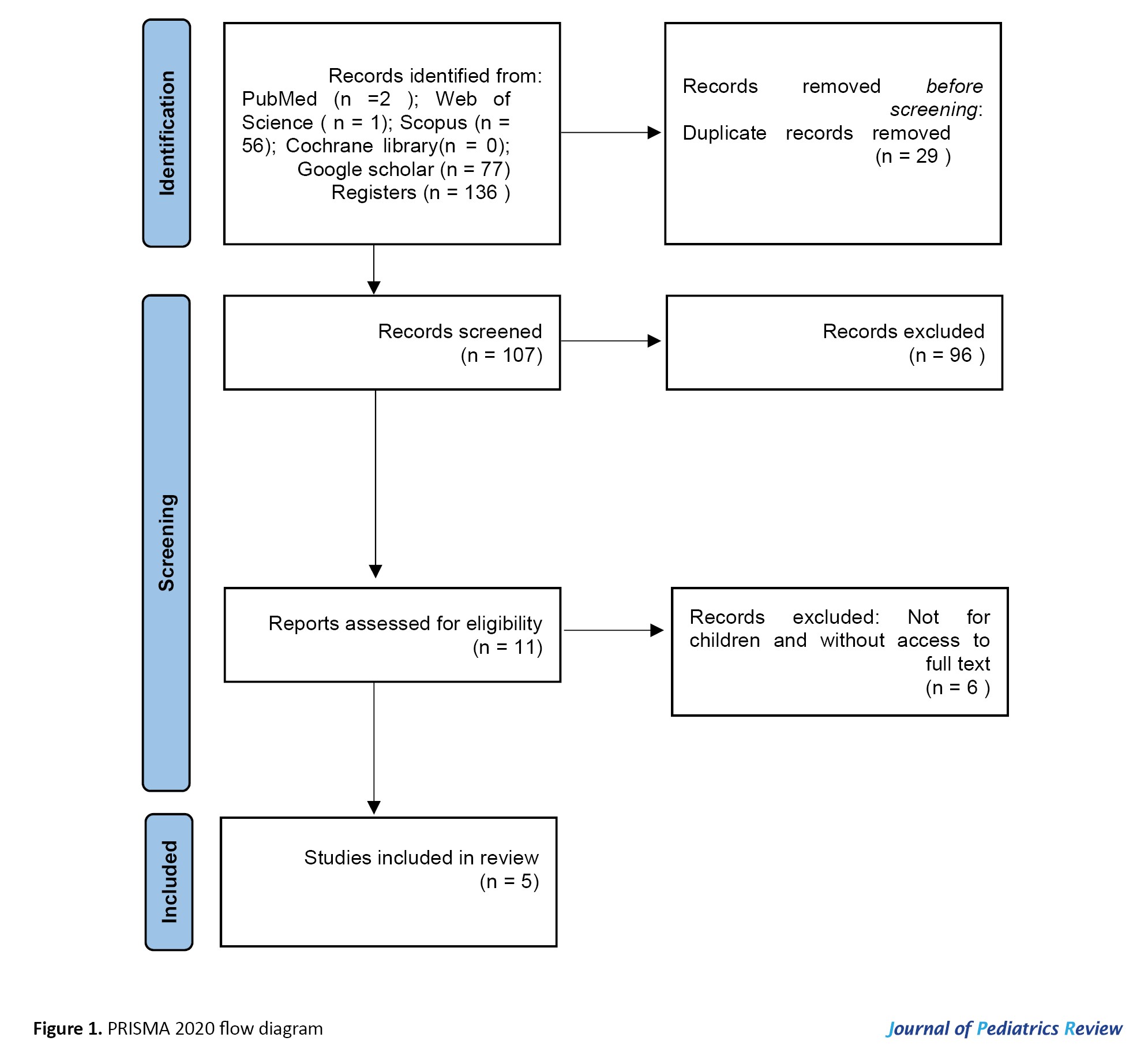
Initially, all retrieved articles were imported into Mendeley Desktop software, version 1.19.8 to identify and remove duplicates. Following deduplication, the remaining studies were independently screened by at least 2 reviewers. Based on the inclusion and exclusion criteria, irrelevant studies were excluded. Subsequently, data evaluation and extraction were performed for the eligible studies, and the information was systematically recorded in Microsoft Excel (Figure 1).
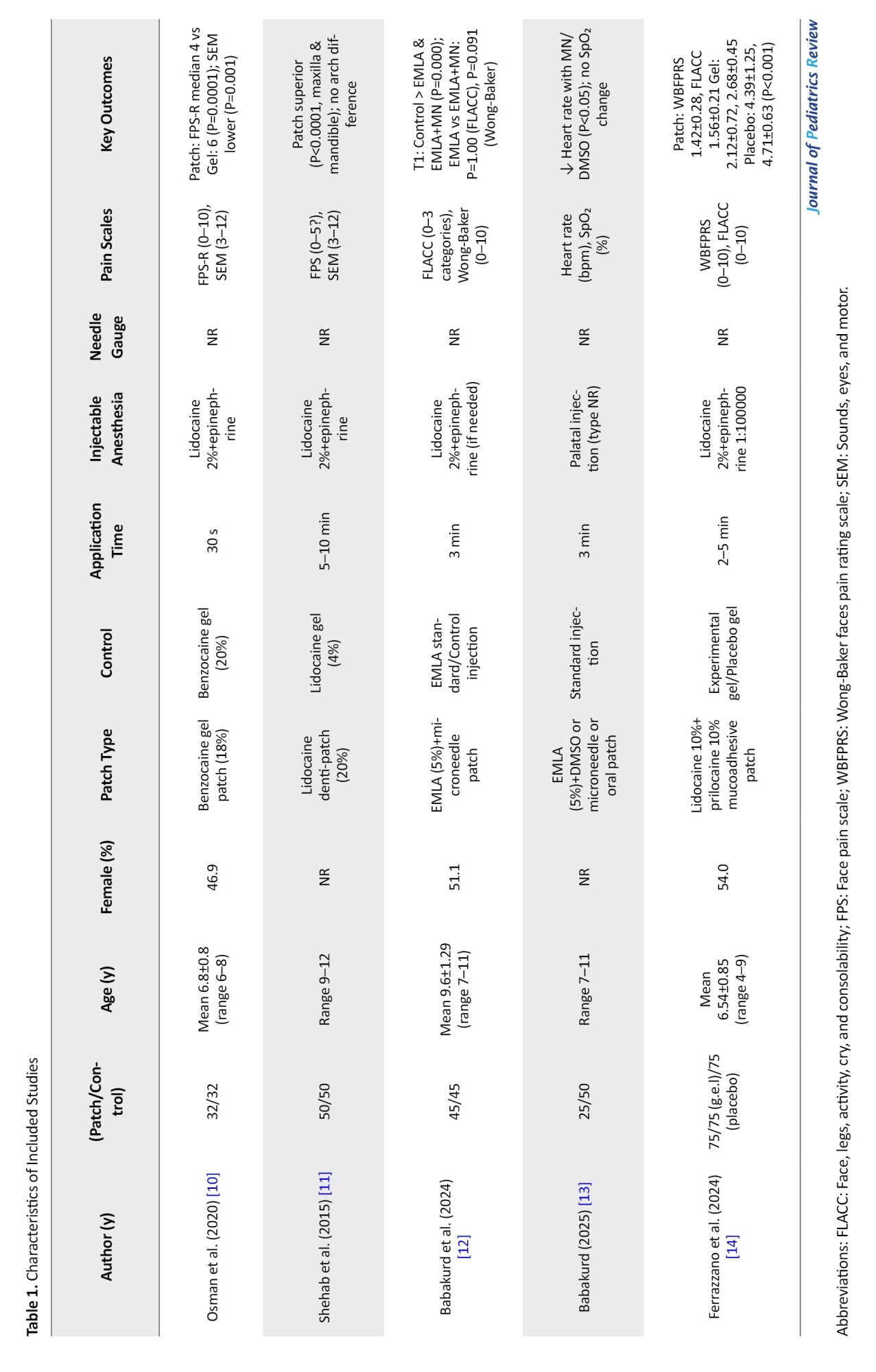
 The extracted data included the author name, year of publication, sample characteristics, type of topical anesthetic used, intervention details, duration of anesthetic application, type of injectable anesthetic, needle gauge, assessment scales, and reported outcomes (Table 1).
The extracted data included the author name, year of publication, sample characteristics, type of topical anesthetic used, intervention details, duration of anesthetic application, type of injectable anesthetic, needle gauge, assessment scales, and reported outcomes (Table 1).
Data synthesis
Due to heterogeneity in patch types, application durations, and assessment scales, a qualitative synthesis was performed, as meta-analysis was not feasible. This systematic review integrates findings from 5 RCTs published between 2015 and 2025 that assess the effectiveness of mucoadhesive patch systems compared with conventional gel or injection-based methods for topical anesthesia in pediatric dentistry, with an emphasis on pain reduction during dental procedures. The included studies involved children aged 4–12 years, with sample sizes ranging from 32 to 150 participants.
The interventions comprised benzocaine gel patches [10], lidocaine denti-patches [11], EMLA cream with different delivery systems [12, 13], and a novel lidocaine-prilocaine patch [14]. Pain outcomes were evaluated using various subjective scales (e.g. face pain scale-revised [FPS-R], Wong-Baker, Wong-Baker faces pain rating scale [WBFPRS]) and objective measures (e.g. sounds, eyes, and motor [SEM], face, legs, activity, cry, and consolability], heart rate changes [FLACC]). Application times ranged from 30 seconds to 10 minutes, depending on the formulation.
Across all included studies, patch-based interventions consistently demonstrated superior pain reduction compared to controls. Osman et al. reported significantly lower median FPS-R scores with benzocaine patches (4 vs 6, P=0.0001) and reduced SEM scores (P=0.001). Shehab et al. [11] observed a marked decrease in pain intensity with lidocaine Denti-Patches compared with gel (P<0.0001 at both maxillary and mandibular sites). Babakurd and Azzawi [13] noted significant reductions in heart rate during anesthetic application and probing when using EMLA combined with microneedles or DMSO (P<0.05), while Babakurd et al. [12] reported lower FLACC and Wong-Baker scores for both EMLA and EMLA-microneedle systems (P=0.000), with no statistically significant difference between the two (P=1.00 for FLACC; P=0.091 for Wong-Baker). Ferrazzano et al. found that the experimental lidocaine-prilocaine patch achieved the lowest mean WBFPRS (1.42±0.28) and FLACC (1.56±0.21) scores, outperforming both gel and placebo groups (P<0.001).
While results consistently favored mucoadhesive patches, heterogeneity across formulation types, application durations, and pain assessment scales limited the feasibility of direct comparisons. Importantly, no systemic adverse events (e.g. local anesthetic systemic toxicity [LAST], methemoglobinemia) were reported across trials; however, local issues such as poor patch adhesion were noted in some studies [10, 11].
The collective findings indicate that mucoadhesive patch systems—particularly microneedle-enhanced variants—significantly improve anesthetic efficacy, especially for palatal injections in children. Given the variability in outcome reporting (e.g. median values without standard deviations) and methodological diversity, a quantitative meta-analysis using standardized mean differences (SMD) could be feasible with imputed SDs (e.g. via the Hozo method). Nonetheless, possible heterogeneity (likely I2>50%) and potential risk of bias necessitate sensitivity analyses to ensure the robustness and reliability of the conclusions. However, a meta-analysis was not performed due to heterogeneity among studies. Individual study results were reported using the original summary measures.
Risk of bias assessment
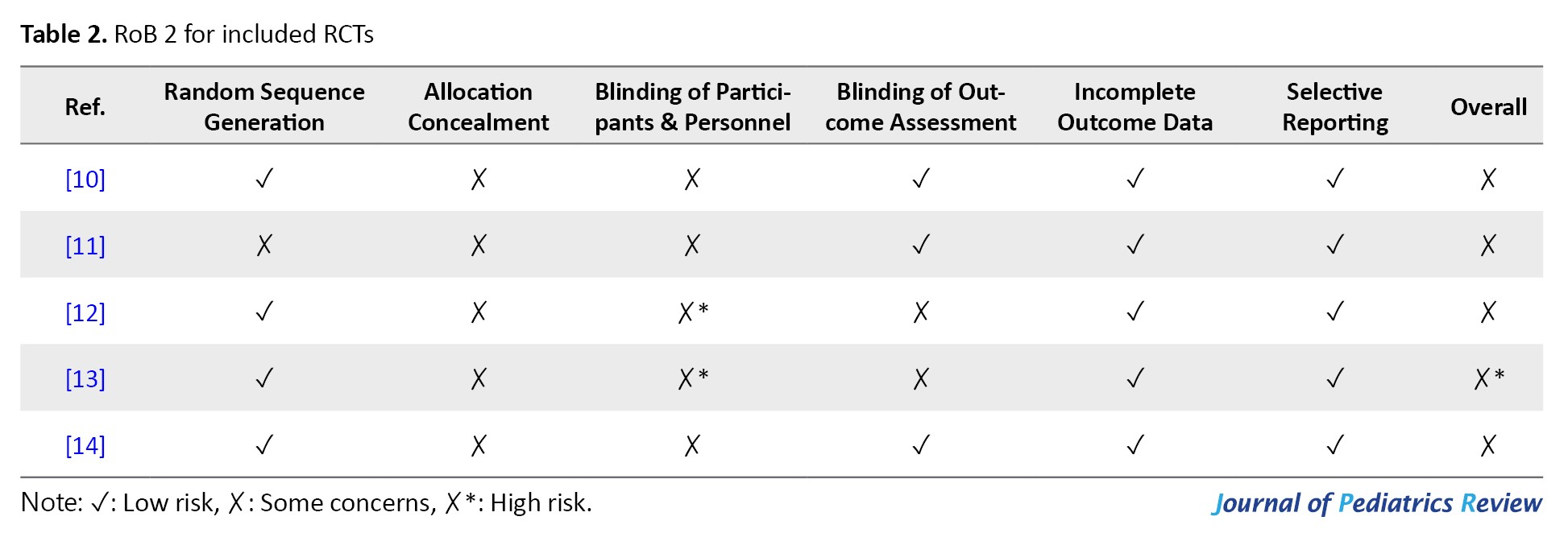
Risk of bias was assessed independently by two reviewers using the Cochrane risk-of-bias 2 (RoB 2) tool [15]. The evaluation was conducted at the outcome level for the primary outcome (pain reduction) and the secondary outcomes (heart rate, adverse events). The six domains of RoB 2 were evaluated as follows:
1) Random sequence generation, 2) allocation concealment, 3) blinding of participants and personnel, 4) blinding of outcome assessment, 5) incomplete outcome data, and 6) selective reporting.
Each domain was rated as low risk, some concerns, or high risk, with an overall judgment derived using the RoB 2 algorithm. Disagreements were resolved by consensus or a third reviewer.
Osman et al. [10] and Ferrazzano et al. [14] were both rated as having “some concerns” due to incomplete operator blinding, despite adequate blinding of children and assessors in Osman et al. [10] and of children, assessors, and caregivers in Ferrazzano et al. [14] This partial blinding may have introduced performance or detection bias. Shehab et al. [11] were also categorized as having “some concerns,” primarily because of insufficient detail regarding randomization concealment and limited blinding (assessor only), potentially leading to allocation bias.
In contrast, Babakurd and Azzawi [13] rated “high risk” due to the lack of blinding for both clinicians and participants, which increases the likelihood of performance bias, despite the study’s use of appropriate statistical analyses. Similarly, Babakurd et al. [12] judged to have “some concerns” since only the data analyst was blinded, with no blinding of operators or children, thereby increasing the potential for biased outcome assessment.
All studies demonstrated a low risk of bias in the domains of missing outcome data and selective reporting, indicating complete data collection and adherence to predefined study protocols. While randomization procedures were generally appropriate, insufficient reporting of allocation concealment in three trials contributed to a moderate overall risk.
Given these findings, the overall risk of bias for the included studies is moderate, with one study [13] at high risk. Consequently, the results should be interpreted with caution, and it is recommended to perform sensitivity analyses excluding the high-risk study to assess the robustness of the pooled outcomes. Future investigations should aim to implement double-blind designs and provide comprehensive descriptions of randomization and allocation procedures to enhance methodological rigor and minimize bias (Table 2).
Results
This systematic descriptive review integrates findings from 5 RCTs conducted between 2015 and 2025 that assessed the efficacy of mucoadhesive patch systems compared with traditional gel or injection methods for topical anesthesia in pediatric dentistry, with a primary focus on pain reduction during dental procedures. The included studies encompassed 447 children aged 4–12 years, with sample sizes ranging from 32 to 150 participants, and were conducted in diverse geographical settings, including Egypt, Saudi Arabia, Syria, and Italy.
The evaluated interventions included benzocaine gel patches [10], lidocaine Denti-patches [11], EMLA cream with delivery systems [12, 13], and a novel lidocaine-prilocaine patch [14]. Application times ranged from 30 seconds to 10 minutes, while pain assessment was conducted using both subjective scales (FPS-R, Wong-Baker, WBFPRS) and objective indicators (SEM, FLACC, heart rate changes in beats per minute).
Across all studies, mucoadhesive patch interventions significantly reduced pain compared to controls. Osman et al. [10] reported a median FPS-R score of 4 for the benzocaine patch versus 6 for the gel (P=0.0001), along with lower SEM scores (P=0.001). Shehab et al. [11] demonstrated that lidocaine Denti-patches were markedly more effective than 4% lidocaine gel, with P<0.0001 for both maxillary and mandibular injections. Babakurd and Azzawi (2025) observed significant reductions in heart rate with EMLA combined with microneedles or DMSO during both the application and probing stages (P<0.05), though oxygen saturation remained unchanged [13]. Similarly, Babakurd et al. (2024) found lower FLACC and Wong-Baker scores with both EMLA and EMLA-microneedle systems (P=0.000), with no significant differences between the two (P=1.00 for FLACC; P=0.091 for Wong-Baker) [12]. Ferrazzano et al. [14] recorded the lowest mean WBFPRS (1.42±0.28) and FLACC (1.56±0.21) scores with the experimental patch, outperforming both gel (2.12±0.72; 2.68±0.45) and placebo (4.39±1.25; 4.71±0.63) (P<0.001) [10-14].
No systemic adverse events (e.g. LAST or methemoglobinemia) were reported across any of the studies. However, local issues such as poor patch adhesion were observed in the studies by Osman et al. and Shehab et al. [10, 11] The analgesic efficacy of mucoadhesive patches was particularly notable in palatal injections, where microneedle-enhanced systems further improved EMLA’s penetration and performance.
Mucoadhesive patches consistently provided superior pain control compared to traditional gels or placebo. Palatal injections benefited most from microneedle-enhanced systems, improving penetration and analgesic efficacy. Nevertheless, heterogeneity in formulation types, application durations, and pain assessment scales hindered direct comparison across studies. Moreover, inconsistencies in data reporting, such as median scores reported without standard deviations, limit the precision of effect estimation. While evidence consistently supports the superior pain control of mucoadhesive patches compared with traditional methods, the magnitude of benefit varies across studies, underscoring the need for standardized protocols and outcome measures in future research to validate and strengthen these findings.
Discussion
The consistent superiority of mucoadhesive patch systems over conventional gel or injection methods for topical anesthesia in pediatric dentistry, as demonstrated by 5 RCTs from 2015 to 2025, underscores their promising potential to improve pain management during dental procedures. These findings are highly relevant to pediatric dentists (enabling calmer procedures), parents (no systemic adverse events, only rare adhesion issues), and policy makers (justifying inclusion in standard pediatric dental kits), supporting immediate clinical adoption while emphasizing the need for future double-blind trials.
A major observation is that mucoadhesive patches provided significant pain reduction across diverse formulations and varying application durations (30 seconds to 10 minutes). Osman et al. [10] and Shehab et al. [11] demonstrated superior analgesic effects with benzocaine and lidocaine patches compared to gels (P=0.001, P<0.0001, respectively). Similarly, Ferrazzano et al. [14] reported lower WBFPRS and FLACC scores with an experimental patch compared with gel and placebo (P<0.001). Two studies by Babakurd et al. (2024, 2025) confirmed the analgesic potential of EMLA-based systems, either alone or combined with microneedles, showing significant reductions in pain and physiological parameters such as heart rate (P<0.05) [12, 13]. Interestingly, Babakurd et al. observed no significant difference between EMLA alone and EMLA-microneedle systems (P=1.00 for FLACC; P=0.091 for Wong-Baker), whereas Babakurd et al. found microneedle application to provide additional benefits [12, 13].
The enhanced performance of patch systems may be attributed to their ability to bypass the anatomical resistance of keratinized palatal mucosa, which typically limits anesthetic absorption. EMLA’s lipophilic nature and higher pH improve diffusion and tissue penetration [12]. However, the diversity in active ingredients (benzocaine, lidocaine, prilocaine), delivery methods (microneedles, DMSO), and outcome measures (FPS-R, SEM, FLACC, Wong-Baker, heart rate) complicates direct comparisons. Importantly, no systemic adverse events were reported, though local adhesion issues [10, 11] indicate areas for technical refinement.
These results position mucoadhesive patch systems as a promising standard for pediatric palatal anesthesia, with potential to improve cooperation and long-term dental experiences. Nevertheless, methodological variability and inconsistent data reporting (e.g. means without standard deviations) limit precise effect-size estimation. Future research should aim to standardize formulations, application protocols, and outcome measures, while exploring the broader adoption of microneedle technology as it becomes more commercially available.
This systematic review has several limitations. Heterogeneity exists in study designs, interventions, and outcome measures, including differences in active ingredients, application durations (30 seconds to 10 minutes), and subjective versus objective pain assessment tools. Risk of bias varies: Babakurd and Azzawi (2025) is rated high due to lack of clinician and child blinding, potentially inflating performance bias [13], while Osman et al. [10] Shehab et al. [11] Ferrazzano et al. [14] and Babakurd et al. studies had some concerns due to incomplete operator blinding or insufficient details on randomization concealment [12]. The focus on cooperative children aged 4–12 with specific dental needs (e.g. extractions) limits generalizability to broader pediatric populations, including those with behavioral or systemic challenges. Additionally, a lack of reported needle gauge and inconsistent reporting on injectable anesthetic characteristics (e.g. epinephrine concentration) complicates comparisons of procedural pain. Implementing sensitivity analyses that exclude high-bias studies, along with standardized protocols in future trials, could help mitigate these limitations and strengthen evidence for clinical practice.
Conclusion
This systematic review of 5 RCTs conducted between 2015 and 2025 demonstrates that mucoadhesive patch systems, including benzocaine, lidocaine, and EMLA with microneedles, effectively reduce pain during pediatric dental procedures.
Ethical Considerations
Compliance with ethical guidelines
The systematic review protocol was registered in PROSPERO (International Prospective Register of Systematic Reviews), maintained by the Centre for Reviews and Dissemination, University of York.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflicts of interest
The authors declared no conflict of interest.
References
Despite continuous progress in dental care and pain control techniques, dental anxiety remains a major challenge for clinicians and patients alike [1]. Local anesthetics are the most commonly used method for managing pain during dental procedures; however, needle phobia persists as a significant concern among both children and adults [1-3]. This fear frequently leads to poor cooperation, complicating both anesthetic administration and the overall treatment process [2-5]. To reduce the discomfort associated with injections, topical anesthetics are commonly applied before needle insertion [4, 6].
Delivering medications through the oral mucosa offers a convenient and non-invasive route of administration. However, this method is challenged by factors such as the constant presence of saliva, which can dilute the drug, and the inherent barrier function of mucosal tissue, which limits drug absorption and permeability. Mucoadhesive formulations that adhere to the mucosal surface can enhance absorption by maintaining higher local drug concentrations at the application site [7]. The use of biopolymers as delivery matrices provides a controlled-release mechanism for therapeutic agents and can be formulated into hydrogels, mucoadhesive films, or patches [8]. These mucoadhesive polymers attach firmly to oral tissues. As the polymer matrix gradually degrades, it enables sustained, controlled drug release over time [9].
In 1996, the U.S. Food and Drug Administration (FDA) approved DentiPatch™, the first transoral lidocaine delivery system designed to provide topical anesthesia and minimize discomfort during dental injections and soft-tissue procedures. Each patch contains 41.6 mg of lidocaine within a 2 cm² adhesive matrix, coated with a polyester backing, and provides effective anesthesia in approximately 2.5 minutes, according to the manufacturer. Clinical trials have verified its safety and efficacy in both adult and pediatric populations, although some studies have reported issues related to inadequate adhesion to the mucosal surface [8].
Accordingly, this systematic review aims to assess the effectiveness and safety of mucoadhesive anesthetic systems compared with conventional local anesthetics in pediatric dentistry.
Materials and Methods
Protocol and registration
This study followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. The literature search strategy was developed according to the problem, intervention or exposure, comparison or control (PICO) framework, defining: Population (P), children undergoing dental procedures; intervention (I), application of topical mucoadhesive anesthetic agents; comparison (C), conventional topical anesthetic agents; and outcome (O), effectiveness of anesthesia.
Children requiring local anesthetic injections were included in the selected studies. In the intervention groups, mucoadhesive topical anesthetics were applied to the mucosal area before the injection. In contrast, control groups received traditional topical agents such as EMLA, benzocaine, or lidocaine before anesthetic administration.
To identify and compare relevant studies on mucoadhesive topical anesthesia, two independent reviewers conducted a comprehensive search of English-language articles published between January 1, 2015, and September 15, 2025, across major databases, including PubMed, Scopus, Web of Science, and the Cochrane Library. Search terms were initially refined using the Medical Subject Headings (MeSH) database, and final keywords included pediatric dentistry, dental patch, topical patch, oral patch, and children. Additionally, a manual search was conducted on Google Scholar using the same keywords to ensure comprehensive coverage of the literature. Last search date: (August 1, September 15, 2025).
Search strategy
The search strategy used the following keywords and operators: (“Pediatric dentistry” [Title/Abstract] Or “pediatric dentistry” [MeSH Terms]) AND (“dental patch” [Title/Abstract] OR “topical patch” [Title/Abstract] OR “oral patch” [Title/Abstract]) AND (“children” [Title/Abstract]) AND (“2015/01/01” [PDAT]: “2025/09/15” [PDAT]) AND English [language].
Eligibility criteria
Randomized controlled trials (RCTs) published in English that involved the application of mucoadhesive topical anesthesia before local anesthetic injection were included in this review. To maintain strict adherence to the PICO framework, only pediatric dentistry studies were prioritized.
The exclusion criteria comprised non-randomized or non-controlled clinical studies, comparative studies without randomization, technical reports, case studies, narrative and systematic reviews, in vitro research, non-English publications, and studies lacking full-text availability.
Initially, all retrieved articles were imported into Mendeley Desktop software, version 1.19.8 to identify and remove duplicates. Following deduplication, the remaining studies were independently screened by at least 2 reviewers. Based on the inclusion and exclusion criteria, irrelevant studies were excluded. Subsequently, data evaluation and extraction were performed for the eligible studies, and the information was systematically recorded in Microsoft Excel (Figure 1).
Data synthesis
Due to heterogeneity in patch types, application durations, and assessment scales, a qualitative synthesis was performed, as meta-analysis was not feasible. This systematic review integrates findings from 5 RCTs published between 2015 and 2025 that assess the effectiveness of mucoadhesive patch systems compared with conventional gel or injection-based methods for topical anesthesia in pediatric dentistry, with an emphasis on pain reduction during dental procedures. The included studies involved children aged 4–12 years, with sample sizes ranging from 32 to 150 participants.
The interventions comprised benzocaine gel patches [10], lidocaine denti-patches [11], EMLA cream with different delivery systems [12, 13], and a novel lidocaine-prilocaine patch [14]. Pain outcomes were evaluated using various subjective scales (e.g. face pain scale-revised [FPS-R], Wong-Baker, Wong-Baker faces pain rating scale [WBFPRS]) and objective measures (e.g. sounds, eyes, and motor [SEM], face, legs, activity, cry, and consolability], heart rate changes [FLACC]). Application times ranged from 30 seconds to 10 minutes, depending on the formulation.
Across all included studies, patch-based interventions consistently demonstrated superior pain reduction compared to controls. Osman et al. reported significantly lower median FPS-R scores with benzocaine patches (4 vs 6, P=0.0001) and reduced SEM scores (P=0.001). Shehab et al. [11] observed a marked decrease in pain intensity with lidocaine Denti-Patches compared with gel (P<0.0001 at both maxillary and mandibular sites). Babakurd and Azzawi [13] noted significant reductions in heart rate during anesthetic application and probing when using EMLA combined with microneedles or DMSO (P<0.05), while Babakurd et al. [12] reported lower FLACC and Wong-Baker scores for both EMLA and EMLA-microneedle systems (P=0.000), with no statistically significant difference between the two (P=1.00 for FLACC; P=0.091 for Wong-Baker). Ferrazzano et al. found that the experimental lidocaine-prilocaine patch achieved the lowest mean WBFPRS (1.42±0.28) and FLACC (1.56±0.21) scores, outperforming both gel and placebo groups (P<0.001).
While results consistently favored mucoadhesive patches, heterogeneity across formulation types, application durations, and pain assessment scales limited the feasibility of direct comparisons. Importantly, no systemic adverse events (e.g. local anesthetic systemic toxicity [LAST], methemoglobinemia) were reported across trials; however, local issues such as poor patch adhesion were noted in some studies [10, 11].
The collective findings indicate that mucoadhesive patch systems—particularly microneedle-enhanced variants—significantly improve anesthetic efficacy, especially for palatal injections in children. Given the variability in outcome reporting (e.g. median values without standard deviations) and methodological diversity, a quantitative meta-analysis using standardized mean differences (SMD) could be feasible with imputed SDs (e.g. via the Hozo method). Nonetheless, possible heterogeneity (likely I2>50%) and potential risk of bias necessitate sensitivity analyses to ensure the robustness and reliability of the conclusions. However, a meta-analysis was not performed due to heterogeneity among studies. Individual study results were reported using the original summary measures.
Risk of bias assessment
Risk of bias was assessed independently by two reviewers using the Cochrane risk-of-bias 2 (RoB 2) tool [15]. The evaluation was conducted at the outcome level for the primary outcome (pain reduction) and the secondary outcomes (heart rate, adverse events). The six domains of RoB 2 were evaluated as follows:
1) Random sequence generation, 2) allocation concealment, 3) blinding of participants and personnel, 4) blinding of outcome assessment, 5) incomplete outcome data, and 6) selective reporting.
Each domain was rated as low risk, some concerns, or high risk, with an overall judgment derived using the RoB 2 algorithm. Disagreements were resolved by consensus or a third reviewer.
Osman et al. [10] and Ferrazzano et al. [14] were both rated as having “some concerns” due to incomplete operator blinding, despite adequate blinding of children and assessors in Osman et al. [10] and of children, assessors, and caregivers in Ferrazzano et al. [14] This partial blinding may have introduced performance or detection bias. Shehab et al. [11] were also categorized as having “some concerns,” primarily because of insufficient detail regarding randomization concealment and limited blinding (assessor only), potentially leading to allocation bias.
In contrast, Babakurd and Azzawi [13] rated “high risk” due to the lack of blinding for both clinicians and participants, which increases the likelihood of performance bias, despite the study’s use of appropriate statistical analyses. Similarly, Babakurd et al. [12] judged to have “some concerns” since only the data analyst was blinded, with no blinding of operators or children, thereby increasing the potential for biased outcome assessment.
All studies demonstrated a low risk of bias in the domains of missing outcome data and selective reporting, indicating complete data collection and adherence to predefined study protocols. While randomization procedures were generally appropriate, insufficient reporting of allocation concealment in three trials contributed to a moderate overall risk.
Given these findings, the overall risk of bias for the included studies is moderate, with one study [13] at high risk. Consequently, the results should be interpreted with caution, and it is recommended to perform sensitivity analyses excluding the high-risk study to assess the robustness of the pooled outcomes. Future investigations should aim to implement double-blind designs and provide comprehensive descriptions of randomization and allocation procedures to enhance methodological rigor and minimize bias (Table 2).
Results
This systematic descriptive review integrates findings from 5 RCTs conducted between 2015 and 2025 that assessed the efficacy of mucoadhesive patch systems compared with traditional gel or injection methods for topical anesthesia in pediatric dentistry, with a primary focus on pain reduction during dental procedures. The included studies encompassed 447 children aged 4–12 years, with sample sizes ranging from 32 to 150 participants, and were conducted in diverse geographical settings, including Egypt, Saudi Arabia, Syria, and Italy.
The evaluated interventions included benzocaine gel patches [10], lidocaine Denti-patches [11], EMLA cream with delivery systems [12, 13], and a novel lidocaine-prilocaine patch [14]. Application times ranged from 30 seconds to 10 minutes, while pain assessment was conducted using both subjective scales (FPS-R, Wong-Baker, WBFPRS) and objective indicators (SEM, FLACC, heart rate changes in beats per minute).
Across all studies, mucoadhesive patch interventions significantly reduced pain compared to controls. Osman et al. [10] reported a median FPS-R score of 4 for the benzocaine patch versus 6 for the gel (P=0.0001), along with lower SEM scores (P=0.001). Shehab et al. [11] demonstrated that lidocaine Denti-patches were markedly more effective than 4% lidocaine gel, with P<0.0001 for both maxillary and mandibular injections. Babakurd and Azzawi (2025) observed significant reductions in heart rate with EMLA combined with microneedles or DMSO during both the application and probing stages (P<0.05), though oxygen saturation remained unchanged [13]. Similarly, Babakurd et al. (2024) found lower FLACC and Wong-Baker scores with both EMLA and EMLA-microneedle systems (P=0.000), with no significant differences between the two (P=1.00 for FLACC; P=0.091 for Wong-Baker) [12]. Ferrazzano et al. [14] recorded the lowest mean WBFPRS (1.42±0.28) and FLACC (1.56±0.21) scores with the experimental patch, outperforming both gel (2.12±0.72; 2.68±0.45) and placebo (4.39±1.25; 4.71±0.63) (P<0.001) [10-14].
No systemic adverse events (e.g. LAST or methemoglobinemia) were reported across any of the studies. However, local issues such as poor patch adhesion were observed in the studies by Osman et al. and Shehab et al. [10, 11] The analgesic efficacy of mucoadhesive patches was particularly notable in palatal injections, where microneedle-enhanced systems further improved EMLA’s penetration and performance.
Mucoadhesive patches consistently provided superior pain control compared to traditional gels or placebo. Palatal injections benefited most from microneedle-enhanced systems, improving penetration and analgesic efficacy. Nevertheless, heterogeneity in formulation types, application durations, and pain assessment scales hindered direct comparison across studies. Moreover, inconsistencies in data reporting, such as median scores reported without standard deviations, limit the precision of effect estimation. While evidence consistently supports the superior pain control of mucoadhesive patches compared with traditional methods, the magnitude of benefit varies across studies, underscoring the need for standardized protocols and outcome measures in future research to validate and strengthen these findings.
Discussion
The consistent superiority of mucoadhesive patch systems over conventional gel or injection methods for topical anesthesia in pediatric dentistry, as demonstrated by 5 RCTs from 2015 to 2025, underscores their promising potential to improve pain management during dental procedures. These findings are highly relevant to pediatric dentists (enabling calmer procedures), parents (no systemic adverse events, only rare adhesion issues), and policy makers (justifying inclusion in standard pediatric dental kits), supporting immediate clinical adoption while emphasizing the need for future double-blind trials.
A major observation is that mucoadhesive patches provided significant pain reduction across diverse formulations and varying application durations (30 seconds to 10 minutes). Osman et al. [10] and Shehab et al. [11] demonstrated superior analgesic effects with benzocaine and lidocaine patches compared to gels (P=0.001, P<0.0001, respectively). Similarly, Ferrazzano et al. [14] reported lower WBFPRS and FLACC scores with an experimental patch compared with gel and placebo (P<0.001). Two studies by Babakurd et al. (2024, 2025) confirmed the analgesic potential of EMLA-based systems, either alone or combined with microneedles, showing significant reductions in pain and physiological parameters such as heart rate (P<0.05) [12, 13]. Interestingly, Babakurd et al. observed no significant difference between EMLA alone and EMLA-microneedle systems (P=1.00 for FLACC; P=0.091 for Wong-Baker), whereas Babakurd et al. found microneedle application to provide additional benefits [12, 13].
The enhanced performance of patch systems may be attributed to their ability to bypass the anatomical resistance of keratinized palatal mucosa, which typically limits anesthetic absorption. EMLA’s lipophilic nature and higher pH improve diffusion and tissue penetration [12]. However, the diversity in active ingredients (benzocaine, lidocaine, prilocaine), delivery methods (microneedles, DMSO), and outcome measures (FPS-R, SEM, FLACC, Wong-Baker, heart rate) complicates direct comparisons. Importantly, no systemic adverse events were reported, though local adhesion issues [10, 11] indicate areas for technical refinement.
These results position mucoadhesive patch systems as a promising standard for pediatric palatal anesthesia, with potential to improve cooperation and long-term dental experiences. Nevertheless, methodological variability and inconsistent data reporting (e.g. means without standard deviations) limit precise effect-size estimation. Future research should aim to standardize formulations, application protocols, and outcome measures, while exploring the broader adoption of microneedle technology as it becomes more commercially available.
This systematic review has several limitations. Heterogeneity exists in study designs, interventions, and outcome measures, including differences in active ingredients, application durations (30 seconds to 10 minutes), and subjective versus objective pain assessment tools. Risk of bias varies: Babakurd and Azzawi (2025) is rated high due to lack of clinician and child blinding, potentially inflating performance bias [13], while Osman et al. [10] Shehab et al. [11] Ferrazzano et al. [14] and Babakurd et al. studies had some concerns due to incomplete operator blinding or insufficient details on randomization concealment [12]. The focus on cooperative children aged 4–12 with specific dental needs (e.g. extractions) limits generalizability to broader pediatric populations, including those with behavioral or systemic challenges. Additionally, a lack of reported needle gauge and inconsistent reporting on injectable anesthetic characteristics (e.g. epinephrine concentration) complicates comparisons of procedural pain. Implementing sensitivity analyses that exclude high-bias studies, along with standardized protocols in future trials, could help mitigate these limitations and strengthen evidence for clinical practice.
Conclusion
This systematic review of 5 RCTs conducted between 2015 and 2025 demonstrates that mucoadhesive patch systems, including benzocaine, lidocaine, and EMLA with microneedles, effectively reduce pain during pediatric dental procedures.
Ethical Considerations
Compliance with ethical guidelines
The systematic review protocol was registered in PROSPERO (International Prospective Register of Systematic Reviews), maintained by the Centre for Reviews and Dissemination, University of York.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflicts of interest
The authors declared no conflict of interest.
References
- Sanikop S, Agrawal P, Patil S. Relationship between dental anxiety and pain perception during scaling. J Oral Sci. 2011; 53(3):341-8. [DOI:10.2334/josnusd.53.341] [PMID]
- Kleinknecht RA, Klepac RK, Alexander LD. Origins and characteristics of fear of dentistry. J Am Dent Assoc. 1973; 86(4):842-8. [DOI:10.14219/jada.archive.1973.0165] [PMID]
- Lakshmanan L, Ravindran V. Efficacy of cryotherapy application on the pain perception during intraoral injection: A randomized controlled trial. Int J Clin Pediatr Dent. 2021; 14(5):616-20. [DOI:10.5005/jp-journals-10005-2032] [PMID]
- Dionne RA, Gordon SM, McCullagh LM, Phero JC. Assessing the need for anesthesia and sedation in the general population. J Am Dent Assoc. 1998; 129(2):167-73. [DOI:10.14219/jada.archive.1998.0173] [PMID]
- Malamed SF. Handbook of local anesthesia. Mosby: Elsevier Health Science; 2004. [Link]
- Holst A, Evers H. Experimental studies of new topical anaesthetics on the oral mucosa. Swed Dent J. 1985; 9(5):185-91. [PMID]
- Stie MB, Öblom H, Hansen ACN, Jacobsen J, Chronakis IS, Rantanen J, et al. Mucoadhesive chitosan-and cellulose derivative-based nanofiber-on-foam-on-film system for non-invasive peptide delivery. Carbohydr Polym. 2023; 303:120429. [DOI:10.1016/j.carbpol.2022.120429] [PMID]
- Franz-Montan M, Ribeiro LNM, Volpato MC, Cereda CMS, Groppo FC, Tofoli GR, et al. Recent advances and perspectives in topical oral anesthesia. Expert Opin Drug Deliv. 2017; 14(5):673-84. [DOI:10.1080/17425247.2016.1227784] [PMID]
- Jiménez-castellanos MR, Zia H, Rhodes CT. Mucoadhesive drug delivery systems. Drug Dev Ind Pharm. 1993; 19(1-2):143-94. [DOI:10.3109/03639049309038765]
- Osman Ha. Effectiveness of benzocaine gelpatch in reducing palatal injection pain in pediatric dental patients: A split-mouth randomized clinical trial. Alexandria Den J. 2021; 20(10):1-16. [Link]
- Shehab LA, Basheer B, Baroudi K. Effectiveness of lidocaine Denti patch® system versus lidocaine gel as topical anesthetic agent in children. J Indian Soc Pedod Prev Dent. 2015; 33(4):285-90. [DOI:10.4103/0970-4388.165664] [PMID]
- Babakurd FM, Azzawi SK, Alkhouli M, Al-Nerabieah Z. Evaluation of EMLA cream with microneedle patches in palatal anesthesia in children: A randomized controlled clinical trial. Sci Rep. 2024; 14(1):15295. [DOI:10.1038/s41598-024-66212-9] [PMID]
- Babakurd FM, Azzawi SK. Investigating the impact of drug delivery systems on the efficacy of EMLA cream for palatine anesthesia in children aged 7 to 11 years. Arab J Ped Denti. 2025; 2(1):5. [Link]
- Ferrazzano GF, Di Fabio G, Caruso S, Gatto R, Goyal V, Caruso S. Clinical efficacy and tolerability of a new experimental mucoadhesive patch for topical anesthesia of oral mucosa in pediatric dentistry. J Clin Med. 2024; 13(6):1558. [DOI:10.3390/jcm13061558] [PMID]
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ. 2019; 366. [DOI: 10.1136/bmj.l4898] [PMID]
Type of Study: Review Article |
Subject:
Dentistry
Received: 2025/02/12 | Accepted: 2025/05/23 | Published: 2026/01/1
Received: 2025/02/12 | Accepted: 2025/05/23 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
