
Mon, Jul 13, 2026


Volume 14, Issue 2 (April 2026)
J. Pediatr. Rev 2026, 14(2): 163-176 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghazaiean M, Najafi B, Zamanfar D. Shifting Seasonal Pattern of Type 1 Diabetes Diagnosis and Diabetic Ketoacidosis at Diagnosis Towards Warm Seasons in Children and Adolescents During 2011-2020: A Single Center Experience in Iran. J. Pediatr. Rev 2026; 14 (2) :163-176
URL: http://jpr.mazums.ac.ir/article-1-830-en.html
URL: http://jpr.mazums.ac.ir/article-1-830-en.html



1- Student Research Committee, Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
2- Diabetes Research Center of Mazandaran, Mazandaran University of Medical Sciences, Sari, Iran. ,danielzamanfar@yahoo.com, daniel.zamanfar2024@gmail.com
2- Diabetes Research Center of Mazandaran, Mazandaran University of Medical Sciences, Sari, Iran. ,
Full-Text [PDF 2488 kb]
(107 Downloads)
| Abstract (HTML) (346 Views)
Full-Text: (47 Views)
Introduction
Type 1 diabetes mellitus (T1DM) is a chronic autoimmune condition resulting from the immune-mediated destruction of pancreatic beta cells [1]. The incidence of T1DM is steadily increasing, with an estimated annual increase of 3%. Projections indicate that by 2025, the number of individuals with T1DM is projected to reach 285 million [2]. Numerous studies have shown a seasonal trend in the occurrence of T1DM, while others have not. Moreover, specific subgroups have been found to exhibit seasonal variations, as indicated by several studies [3, 4]. It has been suggested that seasonality may be more pronounced in regions with higher T1DM rates, but a definitive conclusion has not been reached [5]. Therefore, this variability has made it difficult to compare studies, resulting in conflicting results. Understanding the frequency and distribution of T1DM and other diseases is crucial for guiding epidemiological, etiological, and clinical research, as well as designing, implementing, and assessing public health initiatives [6]. The incidence and temporal patterns of T1DM have been extensively documented, particularly in high- and middle-income nations [7]. Prevalence estimates, on the other hand, are sparse and often derived by applying incidence rates to age- and sex-specific estimates of population size, assuming childhood mortality is very low [8]. The current study aimed to investigate the seasonal variability of T1DM onset and initial presentation with diabetic ketoacidosis (DKA) in a 10-year period comparing two 5-year intervals.
Materials and Methods
Ethics
The researchers prioritized the confidentiality of all information obtained from study participants and obtained written informed consent from patients or their guardians who participated in the study. The study proposal underwent thorough review and received approval from the Ethics Committee of Mazandaran University of Medical Sciences, ensuring its alignment with the ethical standards outlined in the Declaration of Helsinki (1964) and subsequent amendments or similar ethical standards and Ethics Committee approval date was on 2021.
Study design and population
This retrospective study investigated the seasonal variation in demographic characteristics and initial presentation of children and adolescents with T1DM referred to the pediatric diabetes clinic from 2011 to 2020. Our center’s pediatric diabetes clinic serves as the primary referral center for T1DM patients in Mazandaran Province, attracting the majority of its patients from both urban and rural areas in the region. This study utilized a census sampling approach to include all children and adolescents diagnosed with T1DM over the decade. The selection criteria included the inclusion of children and adolescents aged 18 or younger diagnosed with T1DM, while those with other types of diabetes (such as maturity-onset diabetes of the young [MODY]), those without consent from their guardians, or those with incomplete medical records were excluded.
The study population consisted of patients diagnosed with T1DM before the onset of the COVID-19 pandemic, divided into two groups. Group 1 comprised children and adolescents aged ≤18 years and under who received a T1DM diagnosis between 2011 and 2015. Group 2 included children and adolescents ≤18 years diagnosed between 2016 and 2020, prior to the COVID-19 pandemic. In our study, 90% of the patients presented with severe DKA based on the International Society for Pediatric and Adolescent Diabetes (ISPAD) categorization [9], while the remaining cases were classified as mild or moderate DKA. The severity of DKA at diagnosis was determined by assessing pH levels in capillary blood samples collected at presentation.
Despite the common practice of categorizing months and seasons as cold or warm, it is essential to recognize that seasonality can vary significantly based on geographical location. To accurately define the cold and warm months and seasons of each region, it is crucial to consider mean temperature data. Our study utilized existing data to establish the temperature thresholds for categorizing months and seasons in our province from 2011-2020. We gathered average monthly and seasonal temperature data from 15 regions in our province, obtained from the Statistics and Research Department of Mazandaran Meteorological Center. This data was then correlated with the residential locations of most patients included in our study over the same time period. In our study, the majority of participants were from 14 cities in Mazandaran Province. It is important to note that the ten-year average temperature data were available for only 9 of these cities. Consequently, we initially gathered average temperature information for cities, such as Sari, Qaem Shahr, Amol, Babolsar, Alasht, Nowshahr, Galugah, Dasht-e Naz, and Amirabad For the remaining regions without available average temperature data, we strategically selected areas in close proximity to the cities with available data to ensure the accuracy of their average temperatures. These areas included Syahbisheh, Polsefid, Kojor, Kiasar, and Baladeh. To assess the temperature patterns in our province, we performed a comprehensive analysis. This involved calculating the annual mean temperature by averaging monthly data from the 14 regions. Furthermore, we derived the seasonal mean temperature by averaging monthly data for each season. Subsequently, we determined the cut-off temperature for months and seasons for each 5-year period by averaging the temperatures of the 15 regions. These cut-offs were then utilized to identify the cold and warm months and seasons for each 5-year period. Finally, we compared the mean temperature of each month and season over a 10-year period to the calculated cut-off values. This rigorous comparison allowed us to identify the cold and warm months as well as seasons, enabling a more accurate evaluation of T1DM patients based on the month and season of diagnosis.
Data collection
During face-to-face interviews and medical record reviews, a comprehensive checklist of patient information was compiled. This encompassed demographic data, including the year of T1DM diagnosis, age at disease onset, sex, birth weight, birth height, month and season of birth, order of birth, number of children, body mass index (BMI, kg/m2), month and season of T1DM onset, blood group (A, B, AB, O), location (city or village), parental relationship (consanguineous or non-consanguineous), type of delivery (natural vaginal delivery [NVD] or caesarean), type of birth (term or preterm), duration of breastfeeding, age of starting supplementary feeding, history of underlying disease (celiac, Hashimoto disease, hypothyroidism, Down syndrome, allergy, favism, dyslipidemia, asthma, lymphoma, dystrophy, seizures and Graves disease), family history of diabetes, family history of dyslipidemia, family history of autoimmune diseases (hypothyroidism, graves, multiple sclerosis, and rheumatism), and the initial patient presentation with hyperglycemic symptoms including polyuria, polydipsia, polyphagia, nocturia, and weight loss or DKA were collected by two physicians.
Statistical analysis
The normality of the data was assessed using Q-Q plots, histograms, and formal tests (Shapiro-Wilk or Kolmogorov-Smirnov, depending on sample size). Categorical variables were presented as both counts and percentages, while quantitative variables were expressed as Mean±SD. Group comparisons for categorical variables were conducted using the chi-squared test or Fisher’s exact test. For numerical variables, two-group comparisons were performed using either the independent t-test or the Mann–Whitney U test, based on the normality of the corresponding variables. To assess trends over time, we conducted the Mann-Kendall test for monotonic trend. Additionally, bivariate correlation analysis was performed to explore potential relationships between variables. Statistical analysis was conducted using STATA software (version 17) (StataCorp, College Station, TX). Statistical significance was set at P<0.05, using two-tailed P values for all statistical analyses.
Results
Study selection
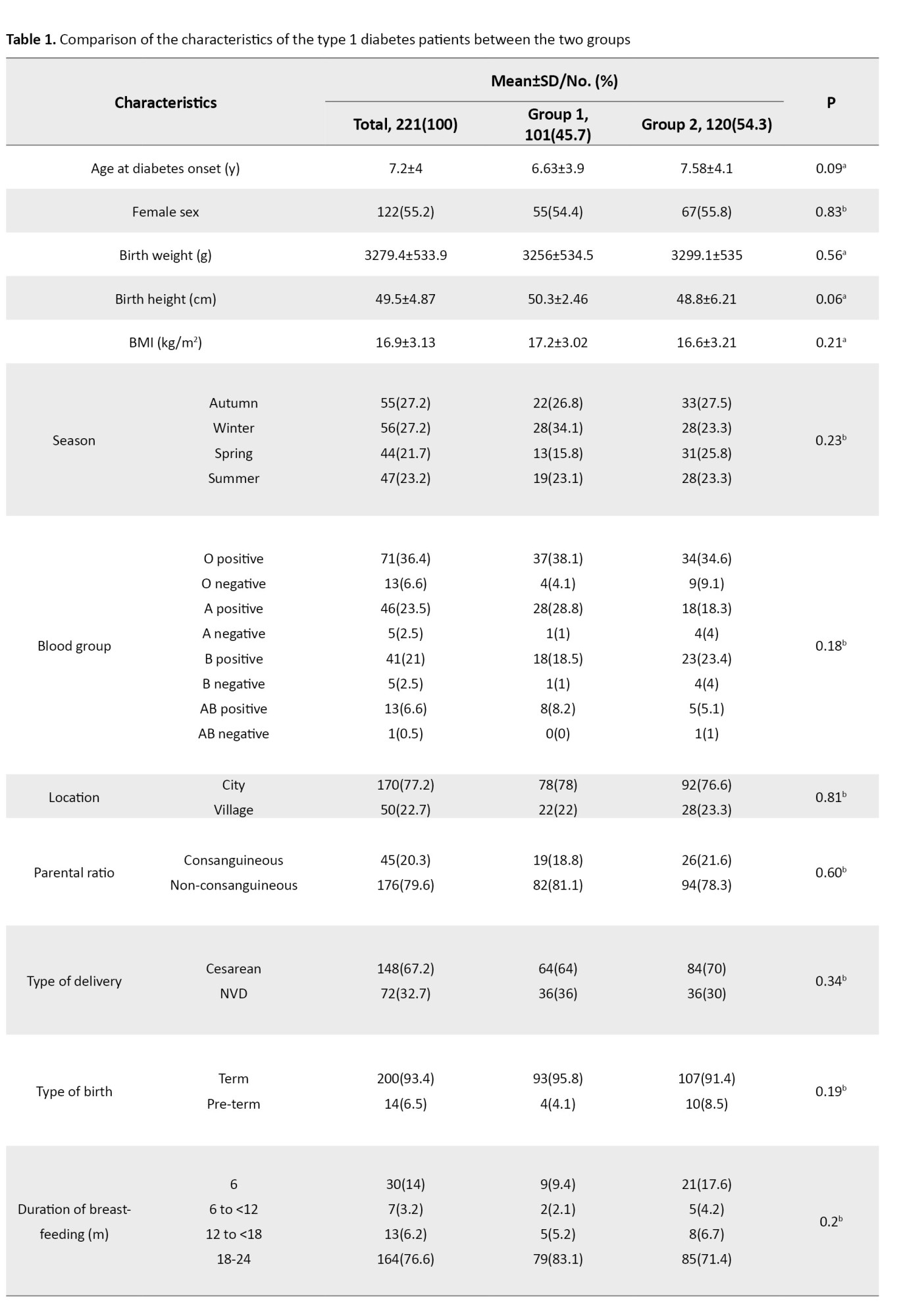
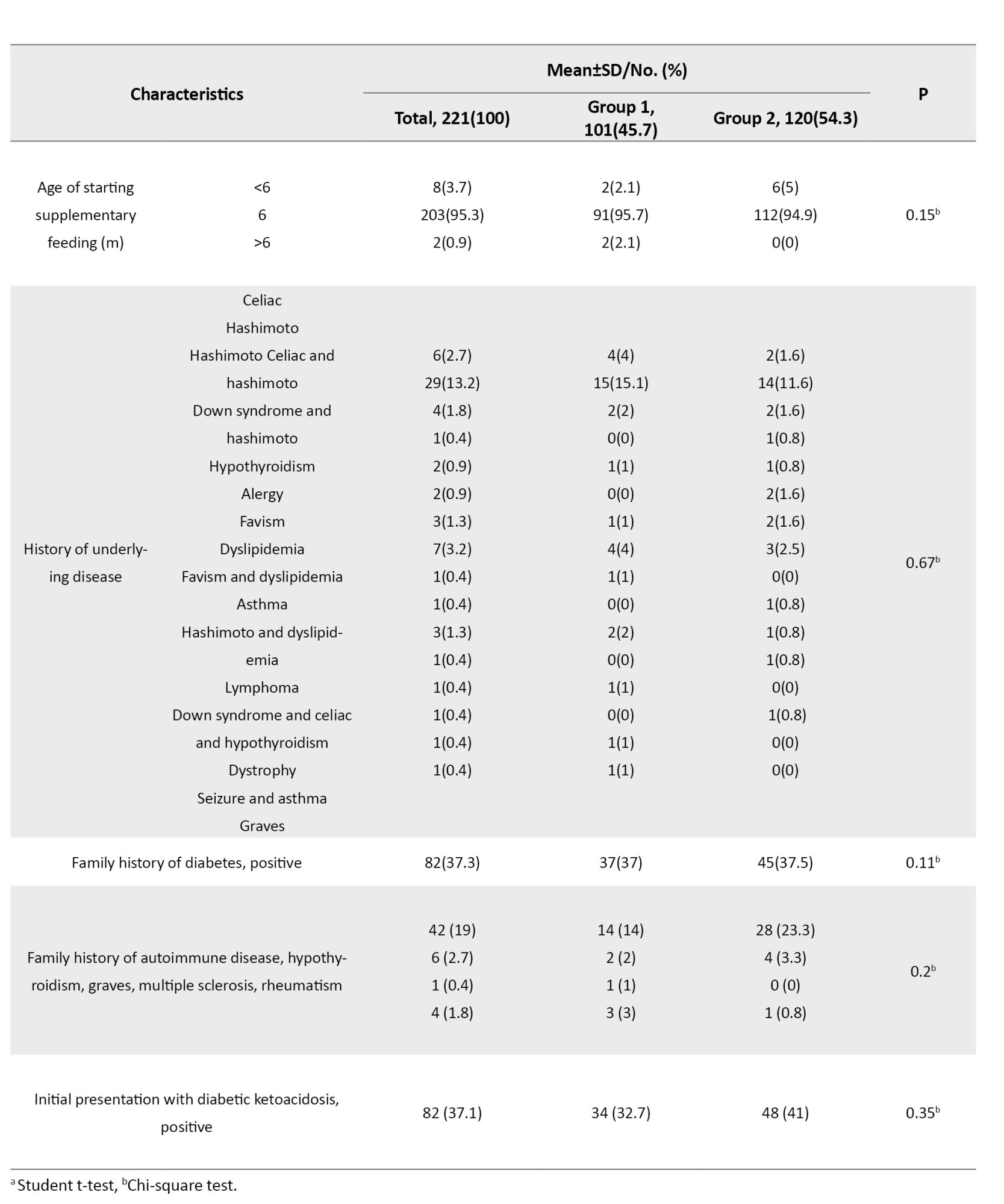
In a cohort of 250 subjects, 29 patients were excluded from the study. Sixteen were excluded due to a MODY diagnosis (one MODY 1, six MODY 2, one MODY 4, one MODY 8, one MODY 9, four MODY 11, one MODY 12, and one MODY 13), and thirteen were excluded due to incomplete medical records. Table 1 presents the characteristics of the study sample.
Trends of T1DM and DKA onset during the 10-year period
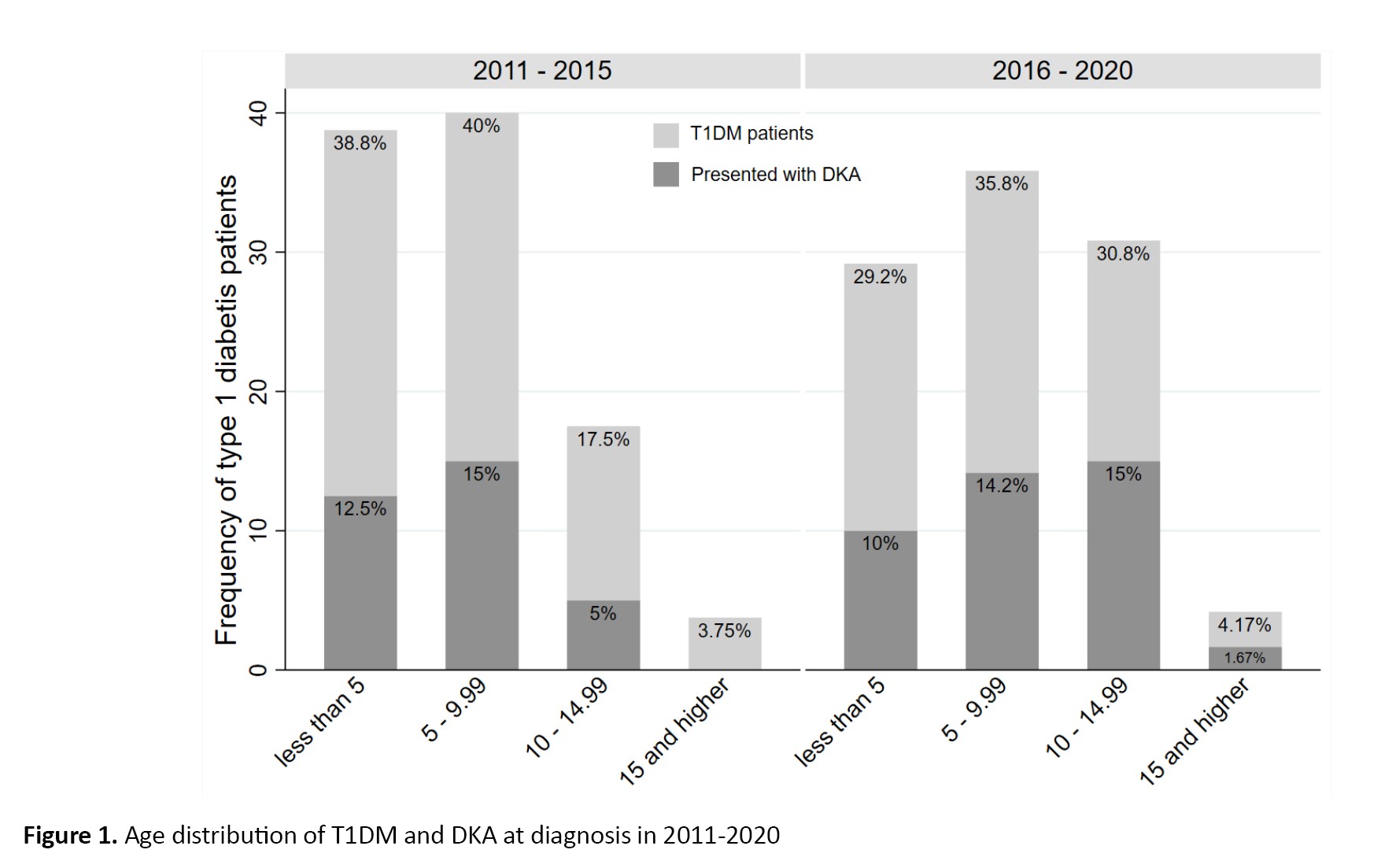
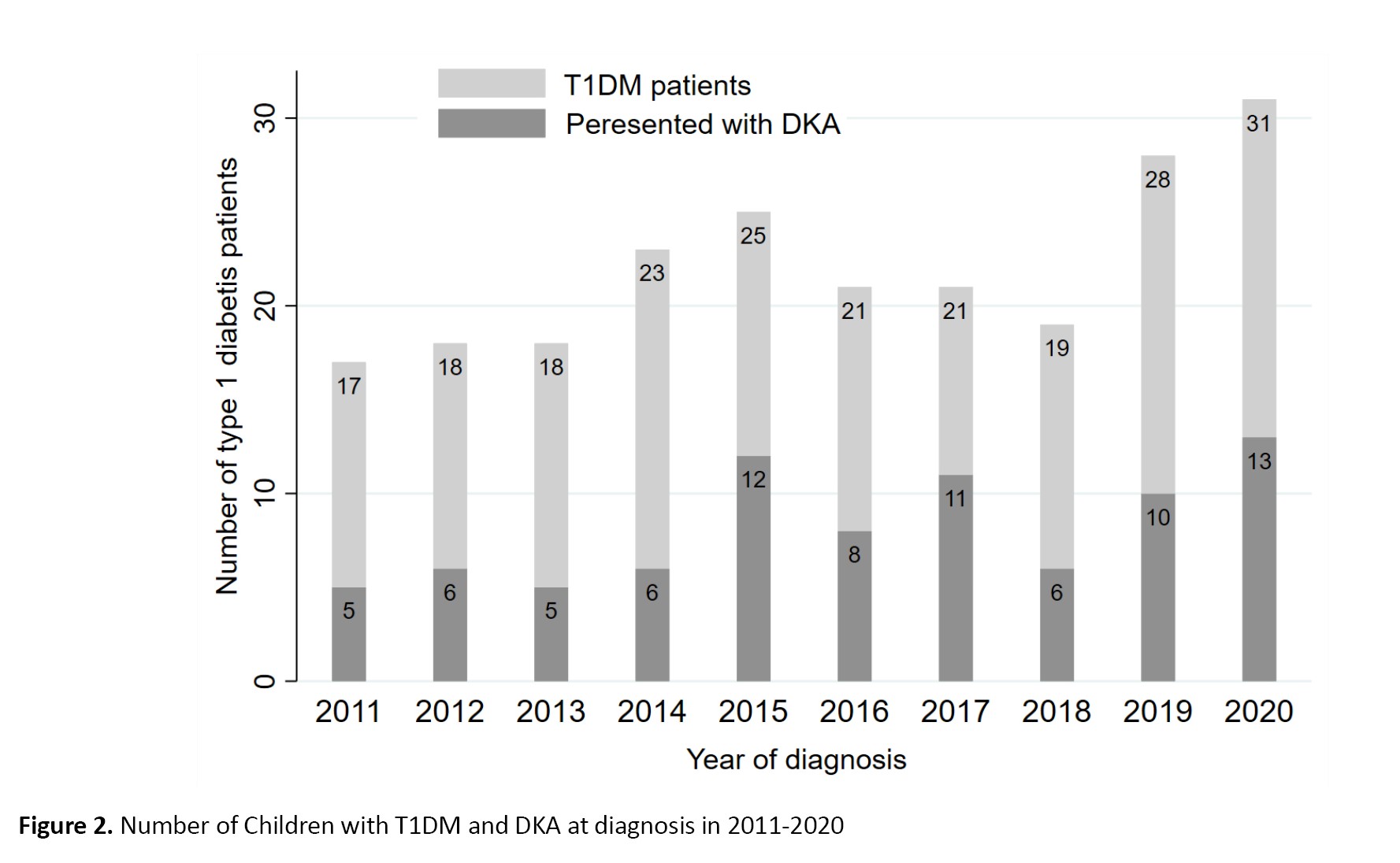
During the observed period, 221 pediatric patients with T1DM were included in the study, all of whom were from the Clinical Hospital Centre in Mazandaran Province. Out of the participants, 82 presented with DKA as the initial symptom (Figure 1).
 Over the 10-year investigation period, the highest number of T1DM diagnoses in children occurred in 2020 (n=31), with the same year also seeing the highest number of 13 out of 82 DKA cases (15.9%). The Mann–Kendall trend test revealed a significant change in T1DM from 2011 to 2020 (tau=0.6138, P=0.0191). A similar result was observed for DKA onset (tau=0.582, P=0.0287).
Over the 10-year investigation period, the highest number of T1DM diagnoses in children occurred in 2020 (n=31), with the same year also seeing the highest number of 13 out of 82 DKA cases (15.9%). The Mann–Kendall trend test revealed a significant change in T1DM from 2011 to 2020 (tau=0.6138, P=0.0191). A similar result was observed for DKA onset (tau=0.582, P=0.0287).
Age and sex distribution of the study findings
Of 221 participants, 101(45.7%) were in group 1 and 120(54.3%) in group 2. Among these participants, 55.2% (n=122) were female. In group 1 and group 2, 54.4% and 55.8% of the patients were female, respectively. The mean age at diagnosis was 7.2±4 years; group 1 (6.63 years, 95% CI, 5.75%, 7.51%) was younger than group 2 (7.58 years, 95% CI, 6.83%, 8.33%). However, the difference was not statistically significant (P=0.09). Male patients in group 2 were older than those in group 1 (7.34±4.1 years vs 5.32±3.3 years). The mean age of female patients in group 2 was nearly the same as that of group 1 (7.68±4.2 years vs 7.76±4.1 years). A marginally significant increase was observed among female patients under 5 years diagnosed during the second period compared to the first period (P=0.051). The frequency of preschool-age children increased during the second 5-year period compared to the first 5-year period, but the increase was not statistically significant (53% vs 47%, P=0.16). The proportion of adolescent patients was significantly higher in group 2 than group 1 (71.2% vs 28.8%, P=0.04). The age distribution of T1DM across the 5-year periods is presented in supplementary file (Figure 2).
 Group 1 comprised 47 firstborn children with an average age of 7.57±4.4 years, 31 second-born children with an average age of 5.22±2.7 years, one thirdborn child aged 6 years, and one fourth-born child aged 7 years. In comparison, group 2 consisted of 68 firstborn children with an average age of 8.75±4.2 years, 41 secondborn children with an average age of 5.95±3.4 years, one thirdborn child aged 6 years, and one fourthborn child aged 8 years.
Group 1 comprised 47 firstborn children with an average age of 7.57±4.4 years, 31 second-born children with an average age of 5.22±2.7 years, one thirdborn child aged 6 years, and one fourth-born child aged 7 years. In comparison, group 2 consisted of 68 firstborn children with an average age of 8.75±4.2 years, 41 secondborn children with an average age of 5.95±3.4 years, one thirdborn child aged 6 years, and one fourthborn child aged 8 years.
An analysis of the gender of the patients and the type of delivery revealed that the number of patients born by caesarean section was approximately double that of those born by NVD, for both males and females. The mean age of patients born via NVD and cesarean section in group 1 was 7.21±4.2 and 6.17±3.64 years, respectively. In contrast, the mean age of patients delivered by NVD or cesarean section in group 2 was 7.75±3.9 and 7.51±4.2 years.
Upon analyzing the initial presentation of the patients, it was found that polydipsia and polyuria were the most prevalent clinical manifestations in children at the time of diagnosis, with 51.8% (74 out of 143 participants) and 50.4% (72 out of 143), respectively. This was followed by weight loss (12.9%, 18 out of 140), nocturia (9.3%, 13 out of 140), and polyphagia (5.7%, 8 out of 140). The frequency of DKA at presentation was 37.1% (95% CI, 30.9%, 43.7%) over a ten-year period, with 32.7% (95% CI, 24.2%, 42.4%) in group 1 and 41% (95% CI, 32.4%, 50%) in group 2 (P=0.35). It is noteworthy that the greatest increase in DKA at presentation occurred in the adolescent age group. Notably, 90% of the patients with DKA at diagnosis were presented with severe DKA (pH <7.1), necessitating intensive care unit hospitalization.
An analysis of the gender distribution of patients referred with DKA revealed that 32(39%) were male and 50(61%) were female, with no statistically significant difference (P=0.17). Among female patients with DKA, 40% were in the 5-9 age range, while nearly 30% of male patients aged 10-14 presented with DKA. Over a 10-year period, 33.3% of children under 5 years old presented with DKA, with frequencies of 32.3% and 34.3% in the first and second 5-year periods, respectively. The frequency of DKA in preschool-age children did not show a significant increase between the first and second periods (46.2% vs 53.9%, P=0.55). During the second period, a significant increase was observed in adolescent patients presenting with DKA compared to the first period (83.3% vs 16.7%, P=0.03). However, the correlation between adolescent age and DKA at presentation was not significant in the second period (chi-squared=0.049, P=0.09). Age distribution of DKA at diagnosis across the 5-year periods is presented in supplementary file (Figure 2).
The comparison of average age between patients presenting with and without DKA revealed significant findings. In group 1, patients referred with DKA were diagnosed at a younger age on average compared to those without DKA (6±3.5 vs 6.9±4.1). Conversely, in group 2, patients referred with DKA were older on average than those without DKA (8.06±4.2 vs 7.3±4.2). Notably, the mean age of patients presenting with DKA in group 2 was significantly higher than those in group 1 (8.06±4.18 vs 6±3.5, P=0.04). In group 2, the mean age of male patients with positive DKA was 7.2 years (95% CI, 5.26%, 9.14%), which was higher than group one’s mean age of 4.6 years (95% CI, 1.86%, 7.25%) (P=0.11). Similarly, the mean age of female patients with DKA in group 2 was 8.5 years (95% CI, 6.82%, 10.22%) compared to 6.8 (95% CI, 5.04%, 8.48%) in group 1 (P=0.16).
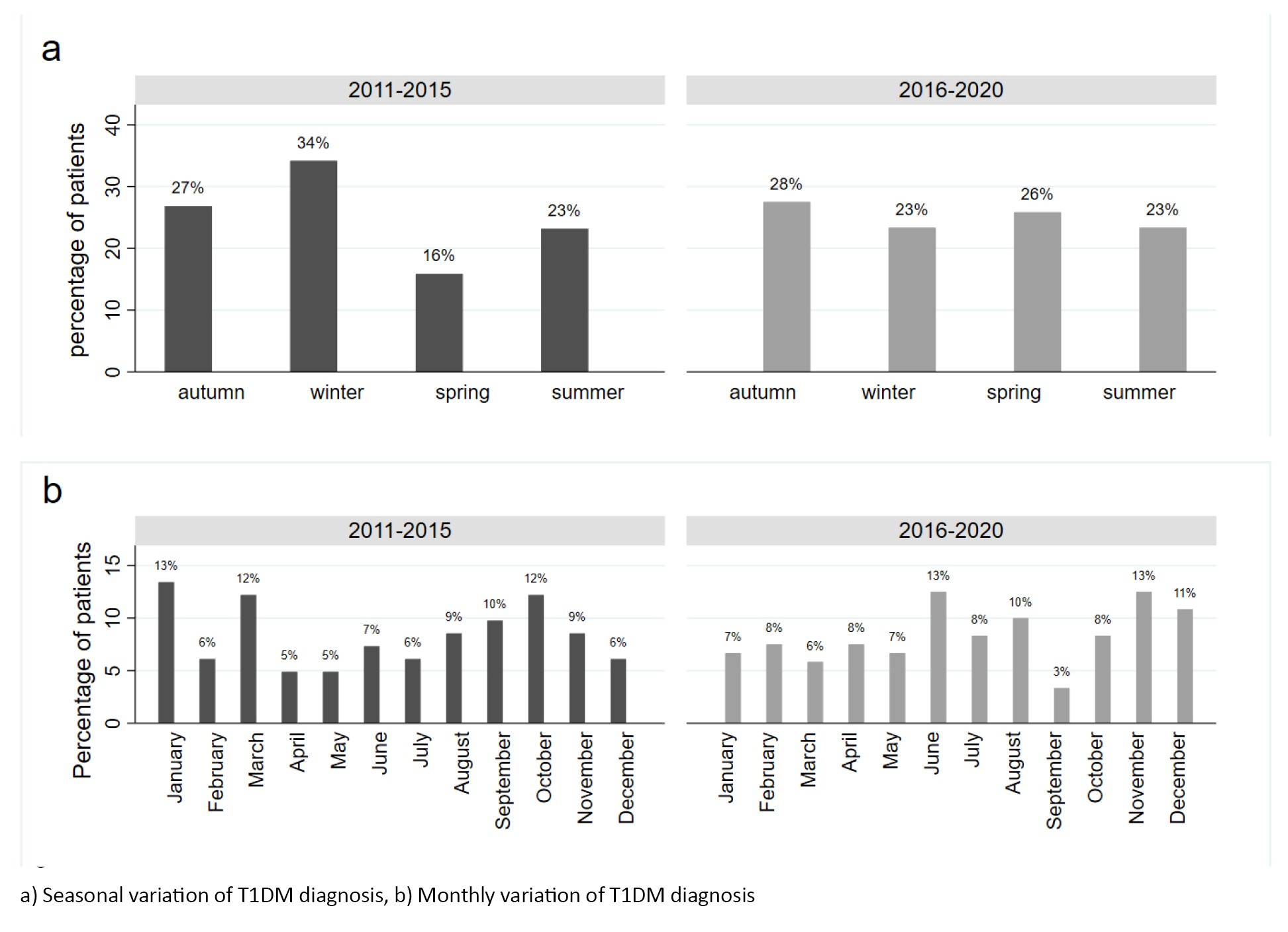
Monthly and seasonal variation of diagnosis
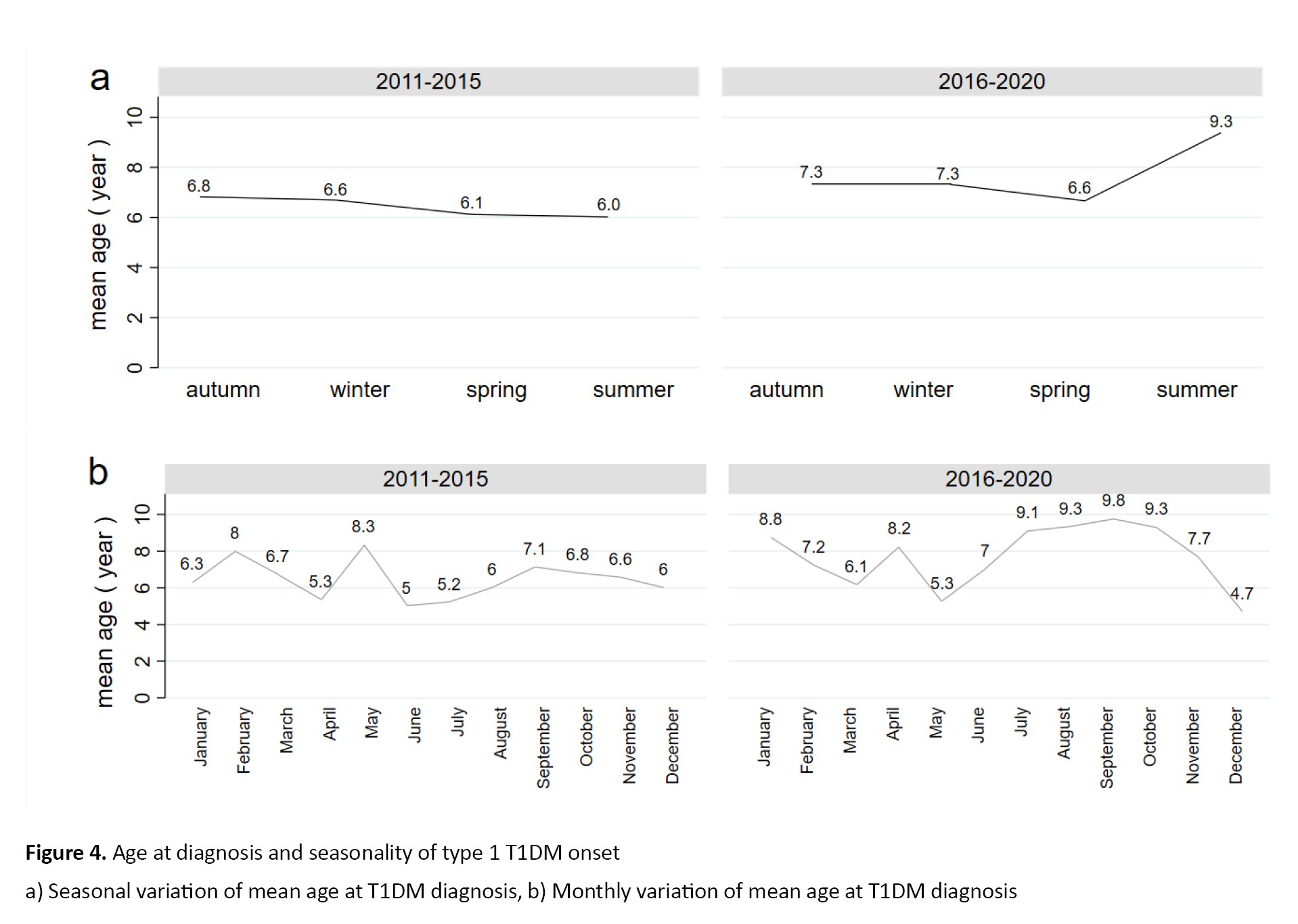
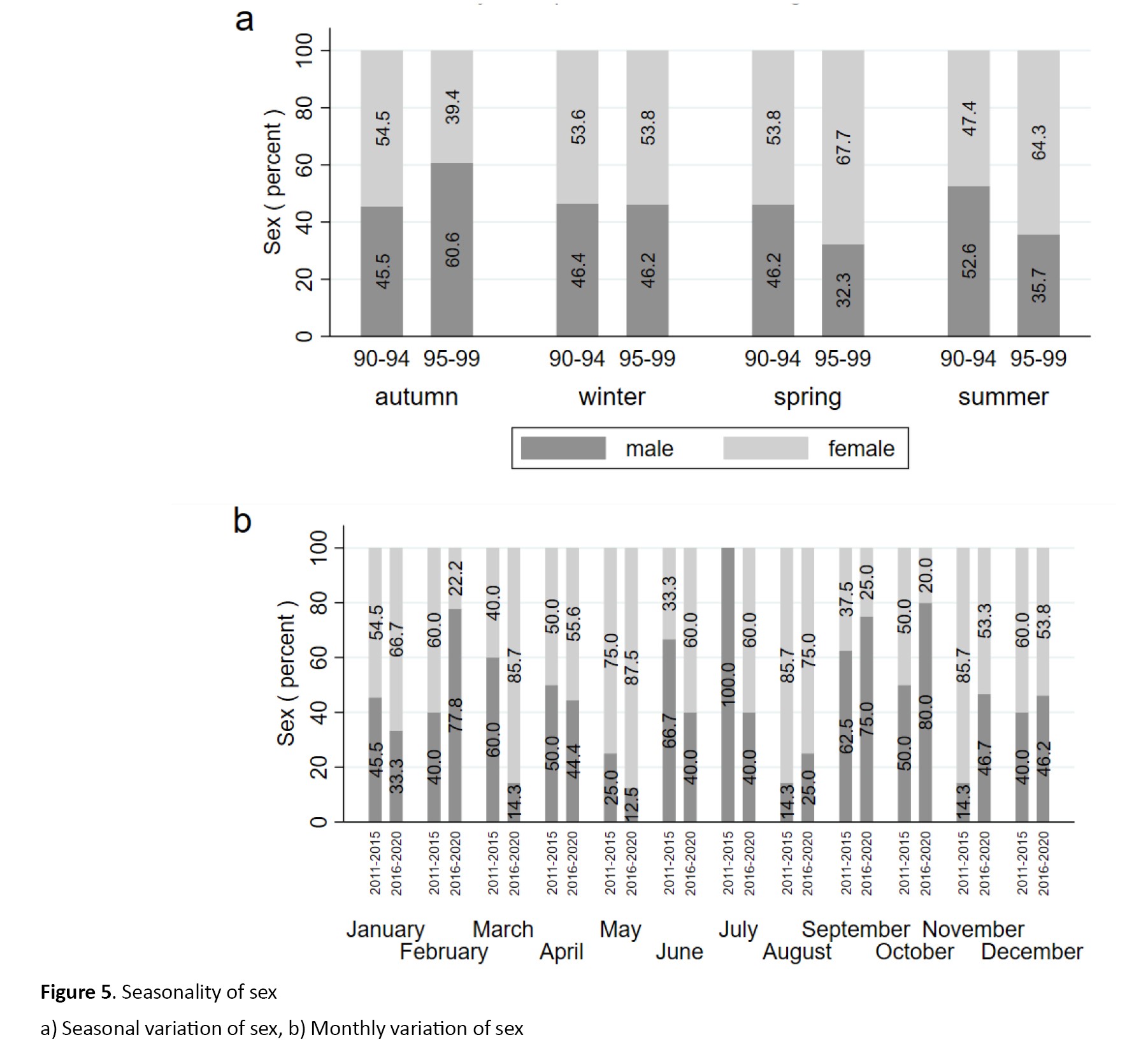
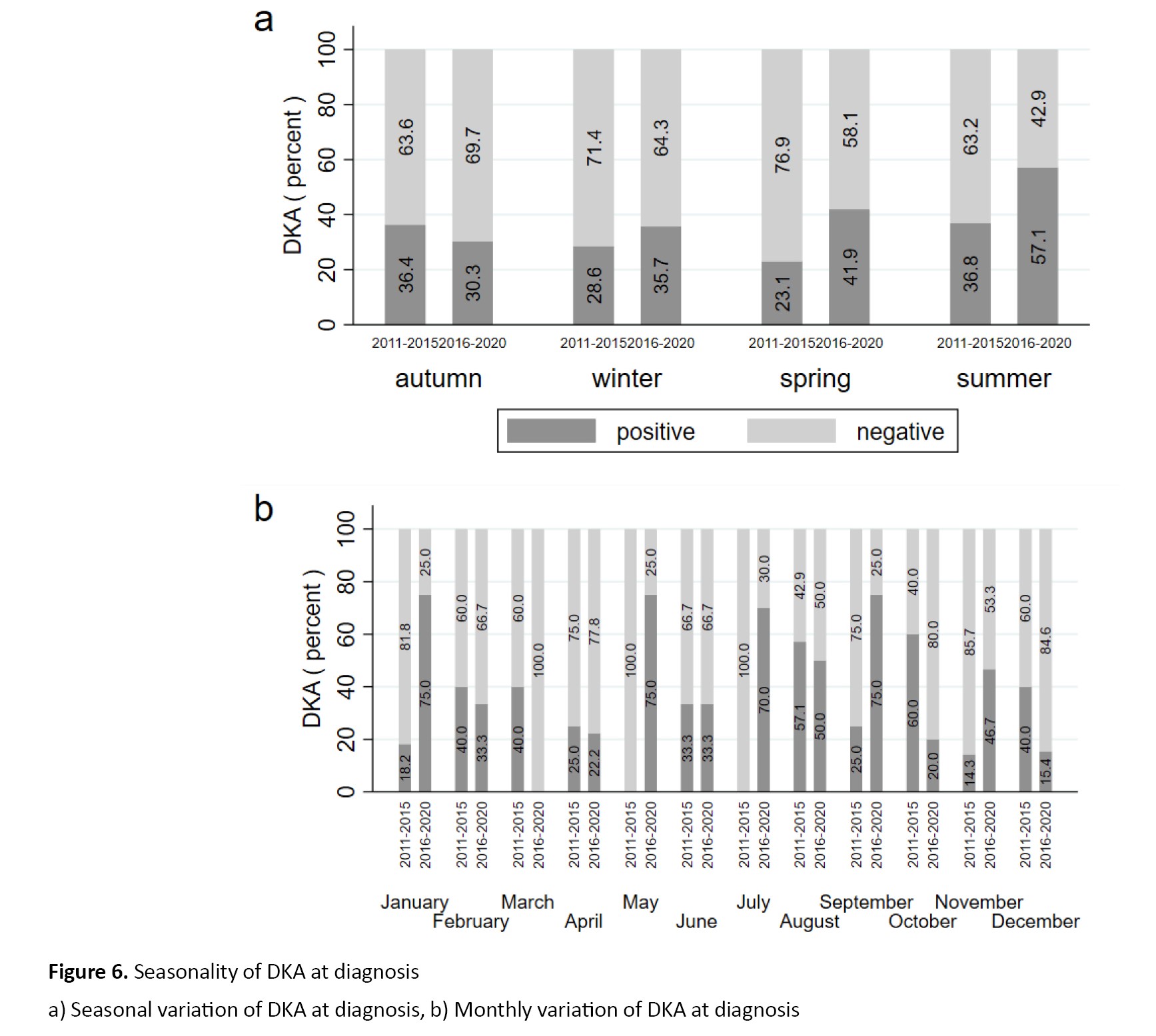
In the initial cohort, an analysis of birth seasons indicated that the highest proportion of patients with T1DM occurred during autumn (28.7%) and winter (25.7%). Conversely, in the second cohort, spring (29.2%) and summer (30%) exhibited the highest frequencies of T1DM cases. A comparison of birth months between the two cohorts revealed that December (10.9%) and July (10.9%) were the most common birth months in the group 1, whereas January (10.8%), March (10.8%), May (10.8%), and July (10.8%) were the most common birth months in group 2. Furthermore, the seasonality of T1DM diagnosis between the two cohorts (Figures 3a and 3b), according to age at diagnosis (Figures 4a and 4b), sex (Figures 5a and 5b), and initial presentation with DKA (Figures 6a and 6b) is presented in detail in the mentioned figures.
 The mean monthly and seasonal temperatures of two groups over the 10-year period are presented in supplementary file (Figure 7).
The mean monthly and seasonal temperatures of two groups over the 10-year period are presented in supplementary file (Figure 7).
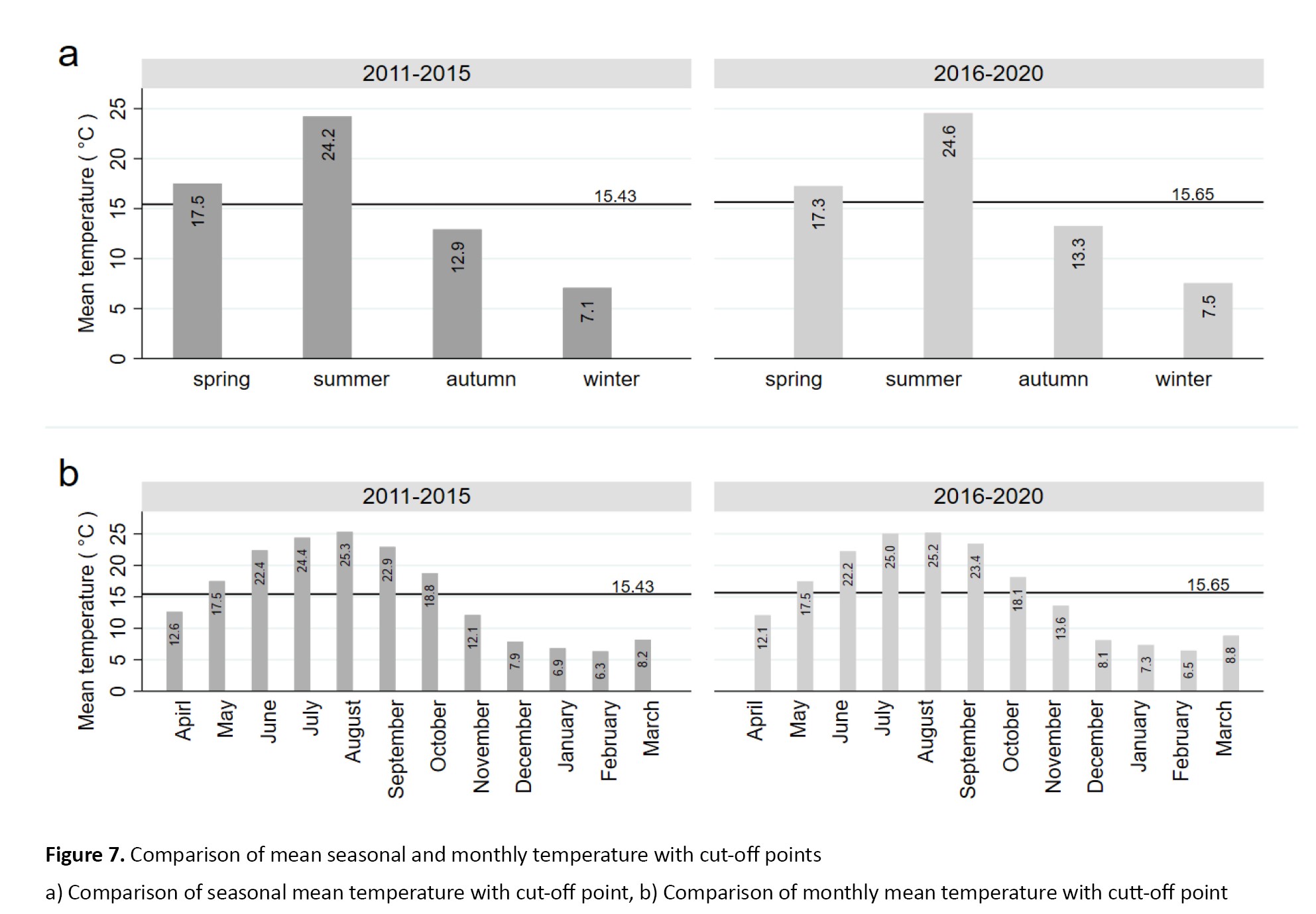 The average five-year cut-off temperature for group 1 (2011-2015) was 15.43 °C, while for group 2 (2016 to 2020), it was 15.65 °C. This analysis confirmed that the cold seasons for both groups were autumn and winter, as previously identified. Additionally, the cold months for both groups were April, November, December, January, February, and March.
The average five-year cut-off temperature for group 1 (2011-2015) was 15.43 °C, while for group 2 (2016 to 2020), it was 15.65 °C. This analysis confirmed that the cold seasons for both groups were autumn and winter, as previously identified. Additionally, the cold months for both groups were April, November, December, January, February, and March.
Discussion
The seasonal pattern of T1DM onset and DKA presentation appears to be shifting toward a higher number of cases during the warmer seasons. The trend of T1DM has shown significant changes from 2011 to 2020. Although the trend in DKA presentation changed significantly, this cannot be attributed solely to the increased number of T1DM patients presenting with DKA during this period. During 2016–2020, the increase in T1DM cases was observed across all age groups, particularly during the warmer seasons. The presentation of DKA shifted towards warmer seasons in group 2. Although the mean monthly and seasonal temperatures of the two 5-periods did not differ significantly, using regionspecific temperature cutoffs may provide a more accurate assessment of T1DM onset and DKA presentation.
In the first 5-year period, the peak of T1DM diagnosis occurred in January and March, while June and November showed the highest number of diagnoses in the second 5-year period. Previous studies have produced conflicting results regarding the seasonal variation of T1DM diagnoses. The SWEET database, encompassing 23,603 patients, reported that the highest rate of T1DM onset was in January and the lowest in June [10]. A meta-analysis by Moltchanova et al. encompassing 53 countries found that the seasonal variation of type 1 diabetes diagnosis is a global phenomenon, likely linked to geographical position. A study of 105 World Health Organization Diabetes Mondiale (WHODiaMond) centers revealed that 42 of them observed seasonality in T1DM onset. Among these, 33 centers reported a peak in T1DM onset during the summer months (June-August), while 28 centers showed troughs in the winter months (October-January) [11]. This study found a significant 10% increase in the rate of T1DM diagnosis during the springtime in the second 5-year period compared to the first. The rate of T1DM diagnosis remained relatively constant in autumn between the two periods, highlighting a noteworthy trend among young individuals. The heightened risk of T1DM during autumn has been associated with higher rates of infections, which can spread more easily due to heightened interaction among children. This trend is likely influenced by a combination of factors, such as higher humidity, lower temperatures, and variations in sunshine hours, all of which can potentially trigger autoimmune processes [12]. As the season transitions from winter to spring, the frequency of T1DM increases, likely due to the lingering effects of winter-borne infections. Specifically, a connection between specific enteroviruses and the advancement to clinical type 1 diabetes has been suggested [13]. Evidence suggests that enteroviruses might act as a catalyst for beta-cell autoimmunity and could also be the final trigger for clinical type 1 diabetes. Enteroviruses primarily impact younger children, and in Finland, over 80% of enterovirus cases are identified from August to December [14]. Hanberger et al. noted comparable results for HbA1c [11], with the levels reaching their highest in late spring and summer when the count of children diagnosed with type 1 diabetes was at its lowest. The outcomes could be attributed to the elevated risk of dehydration or the concealment of heightened thirst in warmer seasons, resulting in more severe metabolic decompensation, or due to delays in diagnosis during summer breaks and reduced access to healthcare services. These findings suggest that the effects of such infections may extend into the following season. While there is a potential link between viral infections and the etiopathogenesis of T1DM, epidemiological studies have indicated that hygiene conditions, geographical locations, vitamin D, nutrition, and sunlight exposure may influence the seasonality of T1DM onset. Environmental factors, including local climate patterns, may influence earlylife risk of T1DM; however, the evidence remains inconclusive.
Both the SWEET database [10] and EURODIAB study [15] have highlighted a clear sinusoidal trend in the seasonality of T1DM diagnosis, with the highest incidence occurring in winter and the lowest in summer. This pattern has been consistently observed across genders and age groups. Furthermore, a comprehensive study by Patterson et al. (1998-2008) involving over 50,000 children under 15 years from 23 European countries also demonstrated a significant sinusoidal pattern, with only two minor exceptions [16]. Our study conducted from 2011 to 2015 revealed a consistent sinusoidal pattern in T1DM diagnosis seasonality. However, this pattern was not observed during 2016-2020. The current study found that T1DM onset seasonality was nearly identical for both sexes in the initial 5-year period, aligning with previous research [10, 11]. However, in the subsequent 5-year period, the seasonality of T1DM diagnosis differed between sexes, consistent with findings from the European Community Concerted Action Program in Diabetes (EURODIAB) registry [16] and data from Finland [17]. Our study revealed that patients diagnosed with T1DM during colder seasons and months tended to be younger on average than those diagnosed during warmer seasons and months. The current study identified a rise in T1DM cases during warmer seasons (spring and summer) across all age groups in the second period, particularly among children aged 5 years and above. These findings align with previous studies and underscore the seasonal variation in T1DM diagnoses [16, 18]. Green et al. [18], similarly found that the onset of T1DM showed marked seasonality in the 10-14 age group. Additionally, Turtinen et al. observed that seasonality was particularly evident in older children aged 5-14 years [19]. Consistent with our study, Moltchanova et al. also noted seasonality in older children, but not in those younger than 5 years [11]. Studies with small sample sizes did not provide evidence supporting seasonality in younger children [17, 20].
In our study, the classical symptoms of polydipsia and polyuria were the prevailing clinical indicators of T1DM. Notably, approximately 37% of the children in the study exhibited DKA, with nearly 90% experiencing severe DKA. It is worth noting that most children with DKA demonstrated severe metabolic acidosis upon admission, aligning with findings from other studies [21, 22]. In contrast to the findings from centers in China and Turkey, where the percentages of children with severe metabolic acidosis on admission were 33.9% and 15.9%, respectively, our results revealed a higher rate of this condition [23, 24]. Nearly two-thirds of patients with the onset of T1DM require treatment in a pediatric intensive care unit (PICU) due to the severe clinical manifestations of DKA. There are limited studies on PICU hospitalization rates at the onset of T1DM; however, our findings suggest that the prevalence of PICU admissions for severe DKA is higher than previously reported by Passanisi et al. [25] and Lah Tomulić et al. [22]. These findings suggest that in our region, if symptoms of T1DM are not recognized early by caregivers, particularly when only polyuria and polydipsia are present, they are identified much later when severe metabolic acidosis has developed, leading to a heightened risk of severe DKA complications. This delay in diagnosis is further exacerbated by mismanagement, limited access to experienced physicians, and a lack of adequately equipped centers. Our study uncovered a distinct pattern in the presentation of DKA, with a higher frequency during the warmer months. This finding contrasts with the observations by Babar et al. [26] and previous studies, which reported the highest frequency of DKA cases during winter [27, 28]. Apart from genetic heterogeneity and racial differences [29], environmental factors specific to the Asian population and other populations could account for the differences in DKA occurrence across geographical areas [30]. Another potential explanation for this variation could be the longer and hotter summers experienced in certain regions, particularly in our province.
Conclusion
The trend of T1DM onset and DKA presentation is shifting towards the warm seasons. Our province has experienced an increase in T1DM cases, with an increase in both the age of onset and DKA frequency at diagnosis.
Limitations and perspectives
The findings of our study may be influenced by several potential factors that could impact our results. Firstly, it is essential to highlight that this study was retrospective. In addition, missing data may have affected the accuracy of our findings. Furthermore, because some information was selfreported, the potential for memory and desirability biases may have constrained the study’s accuracy. We did not categorize children or adolescents by age group, unlike many other studies. This limits our ability to identify distinct seasonal patterns within specific age groups, as seasonality may vary by age. Moreover, while our study included all patients referred to our center from Mazandaran Province in Iran during 2011-2020, the singlecenter design limits the generalizability of the findings. Additional research using multicenter designs that include patients from diverse ethnic backgrounds is needed to improve the applicability of these findings. Furthermore, the relatively small sample size is another limitation, and it is possible that the results may differ with a larger cohort. In addition, future research should focus on determining the actual incidence of brain edema in pediatric patients with DKA, ideally through studies with larger sample sizes. The study is also limited by the lack of access to populationlevel comparison data. Moreover, analyzing viral epidemiological data from two distinct time periods in relation to the month and season of T1DM onset could yield valuable insights into the seasonality of T1DM diagnosis in future studies.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethichs Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.RIB.REC.1400.022).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, methodology, data curation, interpretation, writing, and final approval: All authors; Formal analysis: Behnam Najafi; Validation: Mobin Ghazaiean and Behnam Najafi.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors thank all the participants who contributed to the publication of this article.
References
Type 1 diabetes mellitus (T1DM) is a chronic autoimmune condition resulting from the immune-mediated destruction of pancreatic beta cells [1]. The incidence of T1DM is steadily increasing, with an estimated annual increase of 3%. Projections indicate that by 2025, the number of individuals with T1DM is projected to reach 285 million [2]. Numerous studies have shown a seasonal trend in the occurrence of T1DM, while others have not. Moreover, specific subgroups have been found to exhibit seasonal variations, as indicated by several studies [3, 4]. It has been suggested that seasonality may be more pronounced in regions with higher T1DM rates, but a definitive conclusion has not been reached [5]. Therefore, this variability has made it difficult to compare studies, resulting in conflicting results. Understanding the frequency and distribution of T1DM and other diseases is crucial for guiding epidemiological, etiological, and clinical research, as well as designing, implementing, and assessing public health initiatives [6]. The incidence and temporal patterns of T1DM have been extensively documented, particularly in high- and middle-income nations [7]. Prevalence estimates, on the other hand, are sparse and often derived by applying incidence rates to age- and sex-specific estimates of population size, assuming childhood mortality is very low [8]. The current study aimed to investigate the seasonal variability of T1DM onset and initial presentation with diabetic ketoacidosis (DKA) in a 10-year period comparing two 5-year intervals.
Materials and Methods
Ethics
The researchers prioritized the confidentiality of all information obtained from study participants and obtained written informed consent from patients or their guardians who participated in the study. The study proposal underwent thorough review and received approval from the Ethics Committee of Mazandaran University of Medical Sciences, ensuring its alignment with the ethical standards outlined in the Declaration of Helsinki (1964) and subsequent amendments or similar ethical standards and Ethics Committee approval date was on 2021.
Study design and population
This retrospective study investigated the seasonal variation in demographic characteristics and initial presentation of children and adolescents with T1DM referred to the pediatric diabetes clinic from 2011 to 2020. Our center’s pediatric diabetes clinic serves as the primary referral center for T1DM patients in Mazandaran Province, attracting the majority of its patients from both urban and rural areas in the region. This study utilized a census sampling approach to include all children and adolescents diagnosed with T1DM over the decade. The selection criteria included the inclusion of children and adolescents aged 18 or younger diagnosed with T1DM, while those with other types of diabetes (such as maturity-onset diabetes of the young [MODY]), those without consent from their guardians, or those with incomplete medical records were excluded.
The study population consisted of patients diagnosed with T1DM before the onset of the COVID-19 pandemic, divided into two groups. Group 1 comprised children and adolescents aged ≤18 years and under who received a T1DM diagnosis between 2011 and 2015. Group 2 included children and adolescents ≤18 years diagnosed between 2016 and 2020, prior to the COVID-19 pandemic. In our study, 90% of the patients presented with severe DKA based on the International Society for Pediatric and Adolescent Diabetes (ISPAD) categorization [9], while the remaining cases were classified as mild or moderate DKA. The severity of DKA at diagnosis was determined by assessing pH levels in capillary blood samples collected at presentation.
Despite the common practice of categorizing months and seasons as cold or warm, it is essential to recognize that seasonality can vary significantly based on geographical location. To accurately define the cold and warm months and seasons of each region, it is crucial to consider mean temperature data. Our study utilized existing data to establish the temperature thresholds for categorizing months and seasons in our province from 2011-2020. We gathered average monthly and seasonal temperature data from 15 regions in our province, obtained from the Statistics and Research Department of Mazandaran Meteorological Center. This data was then correlated with the residential locations of most patients included in our study over the same time period. In our study, the majority of participants were from 14 cities in Mazandaran Province. It is important to note that the ten-year average temperature data were available for only 9 of these cities. Consequently, we initially gathered average temperature information for cities, such as Sari, Qaem Shahr, Amol, Babolsar, Alasht, Nowshahr, Galugah, Dasht-e Naz, and Amirabad For the remaining regions without available average temperature data, we strategically selected areas in close proximity to the cities with available data to ensure the accuracy of their average temperatures. These areas included Syahbisheh, Polsefid, Kojor, Kiasar, and Baladeh. To assess the temperature patterns in our province, we performed a comprehensive analysis. This involved calculating the annual mean temperature by averaging monthly data from the 14 regions. Furthermore, we derived the seasonal mean temperature by averaging monthly data for each season. Subsequently, we determined the cut-off temperature for months and seasons for each 5-year period by averaging the temperatures of the 15 regions. These cut-offs were then utilized to identify the cold and warm months and seasons for each 5-year period. Finally, we compared the mean temperature of each month and season over a 10-year period to the calculated cut-off values. This rigorous comparison allowed us to identify the cold and warm months as well as seasons, enabling a more accurate evaluation of T1DM patients based on the month and season of diagnosis.
Data collection
During face-to-face interviews and medical record reviews, a comprehensive checklist of patient information was compiled. This encompassed demographic data, including the year of T1DM diagnosis, age at disease onset, sex, birth weight, birth height, month and season of birth, order of birth, number of children, body mass index (BMI, kg/m2), month and season of T1DM onset, blood group (A, B, AB, O), location (city or village), parental relationship (consanguineous or non-consanguineous), type of delivery (natural vaginal delivery [NVD] or caesarean), type of birth (term or preterm), duration of breastfeeding, age of starting supplementary feeding, history of underlying disease (celiac, Hashimoto disease, hypothyroidism, Down syndrome, allergy, favism, dyslipidemia, asthma, lymphoma, dystrophy, seizures and Graves disease), family history of diabetes, family history of dyslipidemia, family history of autoimmune diseases (hypothyroidism, graves, multiple sclerosis, and rheumatism), and the initial patient presentation with hyperglycemic symptoms including polyuria, polydipsia, polyphagia, nocturia, and weight loss or DKA were collected by two physicians.
Statistical analysis
The normality of the data was assessed using Q-Q plots, histograms, and formal tests (Shapiro-Wilk or Kolmogorov-Smirnov, depending on sample size). Categorical variables were presented as both counts and percentages, while quantitative variables were expressed as Mean±SD. Group comparisons for categorical variables were conducted using the chi-squared test or Fisher’s exact test. For numerical variables, two-group comparisons were performed using either the independent t-test or the Mann–Whitney U test, based on the normality of the corresponding variables. To assess trends over time, we conducted the Mann-Kendall test for monotonic trend. Additionally, bivariate correlation analysis was performed to explore potential relationships between variables. Statistical analysis was conducted using STATA software (version 17) (StataCorp, College Station, TX). Statistical significance was set at P<0.05, using two-tailed P values for all statistical analyses.
Results
Study selection
In a cohort of 250 subjects, 29 patients were excluded from the study. Sixteen were excluded due to a MODY diagnosis (one MODY 1, six MODY 2, one MODY 4, one MODY 8, one MODY 9, four MODY 11, one MODY 12, and one MODY 13), and thirteen were excluded due to incomplete medical records. Table 1 presents the characteristics of the study sample.
Trends of T1DM and DKA onset during the 10-year period
During the observed period, 221 pediatric patients with T1DM were included in the study, all of whom were from the Clinical Hospital Centre in Mazandaran Province. Out of the participants, 82 presented with DKA as the initial symptom (Figure 1).
Age and sex distribution of the study findings
Of 221 participants, 101(45.7%) were in group 1 and 120(54.3%) in group 2. Among these participants, 55.2% (n=122) were female. In group 1 and group 2, 54.4% and 55.8% of the patients were female, respectively. The mean age at diagnosis was 7.2±4 years; group 1 (6.63 years, 95% CI, 5.75%, 7.51%) was younger than group 2 (7.58 years, 95% CI, 6.83%, 8.33%). However, the difference was not statistically significant (P=0.09). Male patients in group 2 were older than those in group 1 (7.34±4.1 years vs 5.32±3.3 years). The mean age of female patients in group 2 was nearly the same as that of group 1 (7.68±4.2 years vs 7.76±4.1 years). A marginally significant increase was observed among female patients under 5 years diagnosed during the second period compared to the first period (P=0.051). The frequency of preschool-age children increased during the second 5-year period compared to the first 5-year period, but the increase was not statistically significant (53% vs 47%, P=0.16). The proportion of adolescent patients was significantly higher in group 2 than group 1 (71.2% vs 28.8%, P=0.04). The age distribution of T1DM across the 5-year periods is presented in supplementary file (Figure 2).
An analysis of the gender of the patients and the type of delivery revealed that the number of patients born by caesarean section was approximately double that of those born by NVD, for both males and females. The mean age of patients born via NVD and cesarean section in group 1 was 7.21±4.2 and 6.17±3.64 years, respectively. In contrast, the mean age of patients delivered by NVD or cesarean section in group 2 was 7.75±3.9 and 7.51±4.2 years.
Upon analyzing the initial presentation of the patients, it was found that polydipsia and polyuria were the most prevalent clinical manifestations in children at the time of diagnosis, with 51.8% (74 out of 143 participants) and 50.4% (72 out of 143), respectively. This was followed by weight loss (12.9%, 18 out of 140), nocturia (9.3%, 13 out of 140), and polyphagia (5.7%, 8 out of 140). The frequency of DKA at presentation was 37.1% (95% CI, 30.9%, 43.7%) over a ten-year period, with 32.7% (95% CI, 24.2%, 42.4%) in group 1 and 41% (95% CI, 32.4%, 50%) in group 2 (P=0.35). It is noteworthy that the greatest increase in DKA at presentation occurred in the adolescent age group. Notably, 90% of the patients with DKA at diagnosis were presented with severe DKA (pH <7.1), necessitating intensive care unit hospitalization.
An analysis of the gender distribution of patients referred with DKA revealed that 32(39%) were male and 50(61%) were female, with no statistically significant difference (P=0.17). Among female patients with DKA, 40% were in the 5-9 age range, while nearly 30% of male patients aged 10-14 presented with DKA. Over a 10-year period, 33.3% of children under 5 years old presented with DKA, with frequencies of 32.3% and 34.3% in the first and second 5-year periods, respectively. The frequency of DKA in preschool-age children did not show a significant increase between the first and second periods (46.2% vs 53.9%, P=0.55). During the second period, a significant increase was observed in adolescent patients presenting with DKA compared to the first period (83.3% vs 16.7%, P=0.03). However, the correlation between adolescent age and DKA at presentation was not significant in the second period (chi-squared=0.049, P=0.09). Age distribution of DKA at diagnosis across the 5-year periods is presented in supplementary file (Figure 2).
The comparison of average age between patients presenting with and without DKA revealed significant findings. In group 1, patients referred with DKA were diagnosed at a younger age on average compared to those without DKA (6±3.5 vs 6.9±4.1). Conversely, in group 2, patients referred with DKA were older on average than those without DKA (8.06±4.2 vs 7.3±4.2). Notably, the mean age of patients presenting with DKA in group 2 was significantly higher than those in group 1 (8.06±4.18 vs 6±3.5, P=0.04). In group 2, the mean age of male patients with positive DKA was 7.2 years (95% CI, 5.26%, 9.14%), which was higher than group one’s mean age of 4.6 years (95% CI, 1.86%, 7.25%) (P=0.11). Similarly, the mean age of female patients with DKA in group 2 was 8.5 years (95% CI, 6.82%, 10.22%) compared to 6.8 (95% CI, 5.04%, 8.48%) in group 1 (P=0.16).
Monthly and seasonal variation of diagnosis
In the initial cohort, an analysis of birth seasons indicated that the highest proportion of patients with T1DM occurred during autumn (28.7%) and winter (25.7%). Conversely, in the second cohort, spring (29.2%) and summer (30%) exhibited the highest frequencies of T1DM cases. A comparison of birth months between the two cohorts revealed that December (10.9%) and July (10.9%) were the most common birth months in the group 1, whereas January (10.8%), March (10.8%), May (10.8%), and July (10.8%) were the most common birth months in group 2. Furthermore, the seasonality of T1DM diagnosis between the two cohorts (Figures 3a and 3b), according to age at diagnosis (Figures 4a and 4b), sex (Figures 5a and 5b), and initial presentation with DKA (Figures 6a and 6b) is presented in detail in the mentioned figures.
Discussion
The seasonal pattern of T1DM onset and DKA presentation appears to be shifting toward a higher number of cases during the warmer seasons. The trend of T1DM has shown significant changes from 2011 to 2020. Although the trend in DKA presentation changed significantly, this cannot be attributed solely to the increased number of T1DM patients presenting with DKA during this period. During 2016–2020, the increase in T1DM cases was observed across all age groups, particularly during the warmer seasons. The presentation of DKA shifted towards warmer seasons in group 2. Although the mean monthly and seasonal temperatures of the two 5-periods did not differ significantly, using regionspecific temperature cutoffs may provide a more accurate assessment of T1DM onset and DKA presentation.
In the first 5-year period, the peak of T1DM diagnosis occurred in January and March, while June and November showed the highest number of diagnoses in the second 5-year period. Previous studies have produced conflicting results regarding the seasonal variation of T1DM diagnoses. The SWEET database, encompassing 23,603 patients, reported that the highest rate of T1DM onset was in January and the lowest in June [10]. A meta-analysis by Moltchanova et al. encompassing 53 countries found that the seasonal variation of type 1 diabetes diagnosis is a global phenomenon, likely linked to geographical position. A study of 105 World Health Organization Diabetes Mondiale (WHODiaMond) centers revealed that 42 of them observed seasonality in T1DM onset. Among these, 33 centers reported a peak in T1DM onset during the summer months (June-August), while 28 centers showed troughs in the winter months (October-January) [11]. This study found a significant 10% increase in the rate of T1DM diagnosis during the springtime in the second 5-year period compared to the first. The rate of T1DM diagnosis remained relatively constant in autumn between the two periods, highlighting a noteworthy trend among young individuals. The heightened risk of T1DM during autumn has been associated with higher rates of infections, which can spread more easily due to heightened interaction among children. This trend is likely influenced by a combination of factors, such as higher humidity, lower temperatures, and variations in sunshine hours, all of which can potentially trigger autoimmune processes [12]. As the season transitions from winter to spring, the frequency of T1DM increases, likely due to the lingering effects of winter-borne infections. Specifically, a connection between specific enteroviruses and the advancement to clinical type 1 diabetes has been suggested [13]. Evidence suggests that enteroviruses might act as a catalyst for beta-cell autoimmunity and could also be the final trigger for clinical type 1 diabetes. Enteroviruses primarily impact younger children, and in Finland, over 80% of enterovirus cases are identified from August to December [14]. Hanberger et al. noted comparable results for HbA1c [11], with the levels reaching their highest in late spring and summer when the count of children diagnosed with type 1 diabetes was at its lowest. The outcomes could be attributed to the elevated risk of dehydration or the concealment of heightened thirst in warmer seasons, resulting in more severe metabolic decompensation, or due to delays in diagnosis during summer breaks and reduced access to healthcare services. These findings suggest that the effects of such infections may extend into the following season. While there is a potential link between viral infections and the etiopathogenesis of T1DM, epidemiological studies have indicated that hygiene conditions, geographical locations, vitamin D, nutrition, and sunlight exposure may influence the seasonality of T1DM onset. Environmental factors, including local climate patterns, may influence earlylife risk of T1DM; however, the evidence remains inconclusive.
Both the SWEET database [10] and EURODIAB study [15] have highlighted a clear sinusoidal trend in the seasonality of T1DM diagnosis, with the highest incidence occurring in winter and the lowest in summer. This pattern has been consistently observed across genders and age groups. Furthermore, a comprehensive study by Patterson et al. (1998-2008) involving over 50,000 children under 15 years from 23 European countries also demonstrated a significant sinusoidal pattern, with only two minor exceptions [16]. Our study conducted from 2011 to 2015 revealed a consistent sinusoidal pattern in T1DM diagnosis seasonality. However, this pattern was not observed during 2016-2020. The current study found that T1DM onset seasonality was nearly identical for both sexes in the initial 5-year period, aligning with previous research [10, 11]. However, in the subsequent 5-year period, the seasonality of T1DM diagnosis differed between sexes, consistent with findings from the European Community Concerted Action Program in Diabetes (EURODIAB) registry [16] and data from Finland [17]. Our study revealed that patients diagnosed with T1DM during colder seasons and months tended to be younger on average than those diagnosed during warmer seasons and months. The current study identified a rise in T1DM cases during warmer seasons (spring and summer) across all age groups in the second period, particularly among children aged 5 years and above. These findings align with previous studies and underscore the seasonal variation in T1DM diagnoses [16, 18]. Green et al. [18], similarly found that the onset of T1DM showed marked seasonality in the 10-14 age group. Additionally, Turtinen et al. observed that seasonality was particularly evident in older children aged 5-14 years [19]. Consistent with our study, Moltchanova et al. also noted seasonality in older children, but not in those younger than 5 years [11]. Studies with small sample sizes did not provide evidence supporting seasonality in younger children [17, 20].
In our study, the classical symptoms of polydipsia and polyuria were the prevailing clinical indicators of T1DM. Notably, approximately 37% of the children in the study exhibited DKA, with nearly 90% experiencing severe DKA. It is worth noting that most children with DKA demonstrated severe metabolic acidosis upon admission, aligning with findings from other studies [21, 22]. In contrast to the findings from centers in China and Turkey, where the percentages of children with severe metabolic acidosis on admission were 33.9% and 15.9%, respectively, our results revealed a higher rate of this condition [23, 24]. Nearly two-thirds of patients with the onset of T1DM require treatment in a pediatric intensive care unit (PICU) due to the severe clinical manifestations of DKA. There are limited studies on PICU hospitalization rates at the onset of T1DM; however, our findings suggest that the prevalence of PICU admissions for severe DKA is higher than previously reported by Passanisi et al. [25] and Lah Tomulić et al. [22]. These findings suggest that in our region, if symptoms of T1DM are not recognized early by caregivers, particularly when only polyuria and polydipsia are present, they are identified much later when severe metabolic acidosis has developed, leading to a heightened risk of severe DKA complications. This delay in diagnosis is further exacerbated by mismanagement, limited access to experienced physicians, and a lack of adequately equipped centers. Our study uncovered a distinct pattern in the presentation of DKA, with a higher frequency during the warmer months. This finding contrasts with the observations by Babar et al. [26] and previous studies, which reported the highest frequency of DKA cases during winter [27, 28]. Apart from genetic heterogeneity and racial differences [29], environmental factors specific to the Asian population and other populations could account for the differences in DKA occurrence across geographical areas [30]. Another potential explanation for this variation could be the longer and hotter summers experienced in certain regions, particularly in our province.
Conclusion
The trend of T1DM onset and DKA presentation is shifting towards the warm seasons. Our province has experienced an increase in T1DM cases, with an increase in both the age of onset and DKA frequency at diagnosis.
Limitations and perspectives
The findings of our study may be influenced by several potential factors that could impact our results. Firstly, it is essential to highlight that this study was retrospective. In addition, missing data may have affected the accuracy of our findings. Furthermore, because some information was selfreported, the potential for memory and desirability biases may have constrained the study’s accuracy. We did not categorize children or adolescents by age group, unlike many other studies. This limits our ability to identify distinct seasonal patterns within specific age groups, as seasonality may vary by age. Moreover, while our study included all patients referred to our center from Mazandaran Province in Iran during 2011-2020, the singlecenter design limits the generalizability of the findings. Additional research using multicenter designs that include patients from diverse ethnic backgrounds is needed to improve the applicability of these findings. Furthermore, the relatively small sample size is another limitation, and it is possible that the results may differ with a larger cohort. In addition, future research should focus on determining the actual incidence of brain edema in pediatric patients with DKA, ideally through studies with larger sample sizes. The study is also limited by the lack of access to populationlevel comparison data. Moreover, analyzing viral epidemiological data from two distinct time periods in relation to the month and season of T1DM onset could yield valuable insights into the seasonality of T1DM diagnosis in future studies.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethichs Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.RIB.REC.1400.022).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, methodology, data curation, interpretation, writing, and final approval: All authors; Formal analysis: Behnam Najafi; Validation: Mobin Ghazaiean and Behnam Najafi.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors thank all the participants who contributed to the publication of this article.
References
- American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2020. Diabetes Care. 2020; 43(Suppl 1):S14-S31. [DOI:10.2337/dc20-S002] [PMID]
- Diamond Project Group. Incidence and trends of childhood type 1 diabetes worldwide 1990-1999. Diabet Med. 2006; 23(8):857-66. [DOI:10.1111/j.1464-5491.2006.01925.x] [PMID]
- Douglas S, McSporran B, Smail P. Seasonality of presentation of type I diabetes mellitus in children. Scottish Study Group for the Care of Young Diabetics. Scott Med J. 1999; 44(2):41-6. [DOI:10.1177/003693309904400205] [PMID]
- Michalková DM, Cernay J, Danková A, Rusnák M, Fandáková K. Incidence and prevalence of childhood diabetes in Slovakia (1985-1992). Slovak Childhood Diabetes Epidemiology Study Group. Diabetes Care. 1995; 18(3):315-20.[DOI:10.2337/diacare.18.3.315] [PMID]
- Onda Y, Sugihara S, Ogata T, Yokoya S, Yokoyama T, Tajima N; et al. Incidence and prevalence of childhood-onset Type 1 diabetes in Japan: The T1D study. Diabet Med. 2017; 34(7):909-15. [DOI:10.1111/dme.13295] [PMID]
- Thacker SB, Berkelman RL. Public health surveillance in the United States. Epidemiol Rev. 1988; 10:164-90.[DOI:10.1093/oxfordjournals.epirev.a036021] [PMID]
- Imperatore G, Mayer-Davis EJ, Orchard TJ, Zhong VW. Prevalence and Incidence of type 1 diabetes among children and adults in the United States and comparison with non-U.S. countries. In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, et al, editors. Diabetes in America. 3rd ed. Bethesda: National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018. [PMID]
- Patterson CC, Dahlquist GG, Gyürüs E, Green A, Soltész G; EURODIAB Study Group. Incidence trends for childhood type 1 diabetes in Europe during 1989-2003 and predicted new cases 2005-20: Multicentre prospective registration study. Lancet. 2009; 373(9680):2027-33. [DOI:10.1016/S0140-6736(09)60568-7] [PMID]
- Wolfsdorf JI, Allgrove J, Craig ME, Edge J, Glaser N, Jain V, et al. ISPAD clinical practice consensus guidelines 2014. Diabetic ketoacidosis and hyperglycemic hyperosmolar state. Pediatr Diabetes. 2014; 15(Suppl 20):154-79. [DOI:10.1111/pedi.12165] [PMID]
- Gerasimidi Vazeou A, Kordonouri O, Witsch M, Hermann JM, Forsander G, de Beaufort C, et al. Seasonality at the clinical onset of type 1 diabetes-lessons from the SWEET database. Pediatr Diabetes. 2016; 17(Suppl 23):32-37.[DOI:10.1111/pedi.12433] [PMID]
- Moltchanova EV, Schreier N, Lammi N, Karvonen M. Seasonal variation of diagnosis of type 1 diabetes mellitus in children worldwide. Diabet Med. 2009; 26(7):673-8. [DOI:10.1111/j.1464-5491.2009.02743.x] [PMID]
- Oikarinen S, Tauriainen S, Hober D, Lucas B, Vazeou A, Sioofy-Khojine A, et al. Virus antibody survey in different European populations indicates risk association between coxsackievirus B1 and type 1 diabetes. Diabetes. 2014; 63(2):655-62. [DOI:10.2337/db13-0620] [PMID]
- Hyöty H, Leon F, Knip M. Developing a vaccine for type 1 diabetes by targeting coxsackievirus B. Expert Rev Vaccines. 2018; 17(12):1071-83. [DOI:10.1080/14760584.2018.1548281] [PMID]
- Jaakola S, Lyytikäinen O, Rimhanen-Finne R, Salmenlinna S, Pirhonen J, Savolainen-Kopra C, Liitsola K, et al. Infectious diseases in Finland 2015. Finnish Institute for Health and Welfare (THL). Helsinki: 2016. [Link]
- Lévy-Marchal C, Patterson C, Green A. Variation by age group and seasonality at diagnosis of childhood IDDM in Europe. The EURODIAB ACE study group. Diabetologia. 1995; 38(7):823-30. [DOI:10.1007/s001250050359] [PMID]
- Patterson CC, Gyürüs E, Rosenbauer J, Cinek O, Neu A, Schober E, et al. Seasonal variation in month of diagnosis in children with type 1 diabetes registered in 23 European centers during 1989-2008: Little short-term influence of sunshine hours or average temperature. Pediatr Diabetes. 2015; 16(8):573-80. [DOI:10.1111/pedi.12227] [PMID]
- Karvonen M, Tuomilehto J, Virtala E, Pitkäniemi J, Reunanen A, Tuomilehto-Wolf E, et al. Seasonality in the clinical onset of insulin-dependent diabetes mellitus in Finnish children. childhood diabetes in Finland (DiMe) study group. Am J Epidemiol. 1996; 143(2):167-76. [DOI:10.1093/oxfordjournals.aje.a008726] [PMID]
- Green A, Patterson CC; EURODIAB TIGER study group. Europe and diabetes. Trends in the incidence of childhood-onset diabetes in Europe 1989-1998. Diabetologia. 2001; 44(Suppl 3):B3-8. [DOI:10.1007/PL00002950] [PMID]
- Turtinen M, Härkönen T, Ilonen J, Parkkola A, Knip M; Finnish Pediatric Diabetes Register. Seasonality in the manifestation of type 1 diabetes varies according to age at diagnosis in Finnish children. Acta Paediatr. 2022; 111(5):1061-9. [DOI:10.1111/apa.16282] [PMID]
- Imkampe AK, Gulliford MC. Trends in Type 1 diabetes incidence in the UK in 0- to 14-year-olds and in 15- to 34-year-olds, 1991-2008. Diabet Med. 2011; 28(7):811-4. [DOI:10.1111/j.1464-5491.2011.03288.x] [PMID]
- Burcul I, Arambasic N, Polic B, Kovacevic T, Bartulovic I, Catipovic Ardalic T, et al. Characteristics of children with diabetic ketoacidosis treated in pediatric intensive care unit: Two-center cross-sectional study in Croatia. Medicina (Kaunas). 2019; 55(7):362. [DOI:10.3390/medicina55070362] [PMID]
- Lah Tomulić K, Matko L, Verbić A, Milardović A, Severinski S, Kolić I, et al. Epidemiologic characteristics of children with diabetic ketoacidosis treated in a pediatric intensive care unit in a 10-year-period: Single centre experience in croatia. Medicina (Kaunas). 2022; 58(5):638.[DOI:10.3390/medicina58050638] [PMID]
- Peng W, Yuan J, Chiavaroli V, Dong G, Huang K, Wu W, et al. 10-year incidence of diabetic ketoacidosis at type 1 diabetes diagnosis in children aged less than 16 years from a large regional center (Hangzhou, China). Front Endocrinol (Lausanne). 2021; 12:653519. [DOI:10.3389/fendo.2021.653519] [PMID]
- Demir F, Günöz H, Saka N, Darendeliler F, Bundak R, Baş F, et al. Epidemiologic features of type 1 diabetic patients between 0 and 18 years of age in İstanbul City. J Clin Res Pediatr Endocrinol. 2015; 7(1):49-56. [DOI:10.4274/jcrpe.1694] [PMID]
- Passanisi S, Salzano G, Basile P, Bombaci B, Caime F, Rulli I, et al. Prevalence and clinical features of severe diabetic ketoacidosis treated in pediatric intensive care unit: A 5-year monocentric experience. Ital J Pediatr. 2023; 49(1):58. [DOI:10.1186/s13052-023-01448-1] [PMID]
- Babar B, Aamir AH. Seasonal variation and severity of Diabetic Ketoacidosis in patients at a tertiary care hospital in Pakistan. Pak J Med Sci. 2022; 38(5):1199-204.[DOI:10.12669/pjms.38.5.5227] [PMID]
- Hou L, Li M, Huang X, Wang L, Sun P, Shi R, et al. Seasonal variation of hemoglobin A1c levels in patients with type 2 diabetes. Int J Diabetes Dev Ctries. 2017; 37(4):432-6. [DOI:10.1007/s13410-016-0500-y]
- ÷Usher-Smith JA, Thompson M, Ercole A, Walter FM. Variation between countries in the frequency of diabetic ketoacidosis at first presentation of type 1 diabetes in children: A systematic review. Diabetologia. 2012; 55(11):2878-94. [DOI:10.1007/s00125-012-2690-2] [PMID]
- Soliman AT, al-Salmi IS, Asfour MG. Epidemiology of childhood insulin-dependent diabetes mellitus in the Sultanate of Oman. Diabet Med. 1996; 13(6):582-6. [DOI:10.1002/(SICI)1096-9136(199606)13:63.0.CO;2-E]
Type of Study: Research Article |
Subject:
Endocrinology
Received: 2025/12/2 | Accepted: 2026/04/3 | Published: 2026/04/3
Received: 2025/12/2 | Accepted: 2026/04/3 | Published: 2026/04/3
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
