
Fri, Apr 19, 2024

Volume 9, Issue 1 (1-2021)
J. Pediatr. Rev 2021, 9(1): 37-46 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nasiri P, Malekzadeh Shafaroudi A, Elyassi Gorgi N, Arab-Nozari M, Nahvi A. Efficacy and Safety of Fluoride in Children: A Narrative Review. J. Pediatr. Rev 2021; 9 (1) :37-46
URL: http://jpr.mazums.ac.ir/article-1-296-en.html
URL: http://jpr.mazums.ac.ir/article-1-296-en.html
Pegah Nasiri1 

 , Ali Malekzadeh Shafaroudi1 , Nadia Elyassi Gorgi1 , Milad Arab-Nozari2 , Azam Nahvi 3
, Ali Malekzadeh Shafaroudi1 , Nadia Elyassi Gorgi1 , Milad Arab-Nozari2 , Azam Nahvi 3
, Ali Malekzadeh Shafaroudi1 , Nadia Elyassi Gorgi1 , Milad Arab-Nozari2 , Azam Nahvi 3
1- Student Research Committee, Mazandaran University of Medical Sciences, Sari, Iran.
2- Department of Toxicology and Pharmacology, Faculty of Pharmacy, Ayatollah Amoli Branch, Islamic Azad University, Amol, Iran.
3- Dental Research Center, Mazandaran University of Medical Sciences, Sari, Iran. , azamnahvi.pedodontist@gmail.com
2- Department of Toxicology and Pharmacology, Faculty of Pharmacy, Ayatollah Amoli Branch, Islamic Azad University, Amol, Iran.
3- Dental Research Center, Mazandaran University of Medical Sciences, Sari, Iran. , azamnahvi.pedodontist@gmail.com
Full-Text [PDF 679 kb]
(2621 Downloads)
| Abstract (HTML) (3489 Views)
Full-Text: (2043 Views)
1. Context
Fluorine (F) is the ninth element in the periodic table of elements, a halogen family member that forms approximately 0.08% of the earth’s crust. Fluorine is naturally found in soil, water, air, plants, and animals in various amounts (1). Fluoride is the simplest anion of fluorine. From the chemical perspective, fluoride is the most electronegative element because of its small atomic radius and high oxidizing potential, allowing it to bond to all other chemical components (2).
In low concentrations, fluoride has a beneficial effect on longevity and dental health (3). It is one of the basic anions required for bone growth and the prevention of caries (4). But, when humans are exposed to high concentrations of this anion, some adverse effects such as skeletal fluorosis or thyroid function alteration may occur (3).
Many scientific papers have noted the efficacy of fluoride in improving oral health (2). All natural water sources contain fluoride in various concentrations. For instance, according to recent studies, the fluoride concentration in seawater is approximately 1.2-1.5 ppm, while fresh drinking water typically exhibits a concentration ranging from 0.01 to 0.03 ppm (5).
Generally, nutritional sources such as meat, fruit, and vegetables contain very low fluoride levels (6). But except for these sources, tea and rice contain high fluoride doses (about 2 ppm) (7). The concentration of fluoride in black tea is the highest among different types of tea (8). Diet and dentifrices are the most significant sources of fluoride exposure in children (9-14).
In dentistry, there are various topical agents and supplements to prevent dental decay, such as dental varnishes, rinses, drops, gels, and tablets (6).
Dental fluorosis is a developmental defect that occurs in the immature enamel during the crown formation of permanent teeth and is the most common impact of excessive fluoride which appears on tooth surfaces (during the first 6 years of life) (5, 6). Because of the variety of flavors in children’s toothpaste, they like to swallow toothpaste and therefore are at a higher risk of developing this complication (15).
Nowadays, fluoride poisoning can occur due to the uncontrolled consumption of dental and oral hygiene products and over-fluoridated water (5). Therefore, it is crucial to control the amount of fluoride intake (16). Studying and understanding the metabolism of fluoride elucidate the influence of fluoride on human health (17).
Our study aimed to review the previous studies on fluoride toxicity and also provide relevant information to dentists and specialists about fluoride safety protocols in children. This article pronounced the beneficial and adverse effects of fluoride on human health.
In low concentrations, fluoride has a beneficial effect on longevity and dental health (3). It is one of the basic anions required for bone growth and the prevention of caries (4). But, when humans are exposed to high concentrations of this anion, some adverse effects such as skeletal fluorosis or thyroid function alteration may occur (3).
Many scientific papers have noted the efficacy of fluoride in improving oral health (2). All natural water sources contain fluoride in various concentrations. For instance, according to recent studies, the fluoride concentration in seawater is approximately 1.2-1.5 ppm, while fresh drinking water typically exhibits a concentration ranging from 0.01 to 0.03 ppm (5).
Generally, nutritional sources such as meat, fruit, and vegetables contain very low fluoride levels (6). But except for these sources, tea and rice contain high fluoride doses (about 2 ppm) (7). The concentration of fluoride in black tea is the highest among different types of tea (8). Diet and dentifrices are the most significant sources of fluoride exposure in children (9-14).
In dentistry, there are various topical agents and supplements to prevent dental decay, such as dental varnishes, rinses, drops, gels, and tablets (6).
Dental fluorosis is a developmental defect that occurs in the immature enamel during the crown formation of permanent teeth and is the most common impact of excessive fluoride which appears on tooth surfaces (during the first 6 years of life) (5, 6). Because of the variety of flavors in children’s toothpaste, they like to swallow toothpaste and therefore are at a higher risk of developing this complication (15).
Nowadays, fluoride poisoning can occur due to the uncontrolled consumption of dental and oral hygiene products and over-fluoridated water (5). Therefore, it is crucial to control the amount of fluoride intake (16). Studying and understanding the metabolism of fluoride elucidate the influence of fluoride on human health (17).
Our study aimed to review the previous studies on fluoride toxicity and also provide relevant information to dentists and specialists about fluoride safety protocols in children. This article pronounced the beneficial and adverse effects of fluoride on human health.
2. Evidence Acquisition
The data we used in our review were found from articles published until August 2019 and using fluoride, toxicity, and children as keywords, collected from official web pages (Google Scholar, Scopus, Ovid, PubMed, and ScienceDirect) and documents published from different international institutions. The search was restricted to articles published in the English language. Topics discussed in this review are the history of fluoride intake, dietary intake of fluoride, fluoride metabolism, the mechanism of fluoride action and overuse, and toxicity of fluoride. After the abstract screening, the full-text of related studies was reviewed. The following types of studies were excluded from this review: in vitro studies, animal studies, studies published in languages other than English, case reports, narrative reviews, medical record reviews, meeting abstracts, historical articles, editorials, letters, and commentaries. The included studies were the ones in which authors published information about exposure to fluoride in children and reported outcomes of interest (such as caries and fluorosis) in participants over time.
3. Results
Dietary intake of fluoride
Fluoride is generally found in our daily diet regimen. It exists in different concentrations in many foods that are mentioned in Table 1 (5). Various fluoride sources include fluoride supplements, fluoride dentifrices, fluoride in water, and foodstuffs (7, 8).

In a previous study, Cardoso et al. reported that the amount of fluoride intake through dentifrices was higher than that through diet (11). Mizira et al. reported the intake of fluoride via dentifrices as 56.3%, water 17.2%, food 11.8%, and in other beverages, this amount was reported 14.7%. It should be noted that this study was conducted in a region with fluoridated water (12). The concentration of fluoride in toothpaste is approximately 0.1% or 1000 ppm (6).
Several organizations, such as the United States Food and Drug Administration, recommended using a smear of toothpaste (a portion the size of a grain of rice) for children under 2 years old and also a pea-size for children younger than 6 years old (13).
Fluoride metabolism
Approximately 90% of ingested fluoride is absorbed from the Gastrointestinal (GI) tract, and the remainder is excreted in the feces (14). Fluoride is bounded to proteins in the plasma; the peak concentration of fluoride in the blood reaches about 20-60 minutes after consumption (15). The concentration of fluoride in the blood is approximately 1% ppm. Fluoride retention in different organs is around 30% in adults and 50% in children. About 99% of these amounts are present in mineralized tissues (teeth and bones), and the remaining 1% is stored in soft tissues (15). Kidney is the main organ responsible for fluoride excretion. Excretion from other sources (such as saliva and sweat) is negligible (14).
Generally, various factors can affect fluoride metabolism, such as acid-base disorders, physical activity, diet, genetics, and kidney function (15). When the fluoride concentration is low, it can enter into the placenta from the mother’s body (16). If its concentration exceeds 0.4 ppm, the placenta acts as a protective barrier and prevents additional fluoride from penetrating the fetus (16, 17). Fluoride can be transmitted to the mothers’ milk, but its concentration is low (18).
The liver is a major site of metabolism in the body; therefore, it is especially prone to fluoride intoxication (19). On the other hand, the kidney is also susceptible to toxicity induced by fluoride as it is the main organ responsible for the excretion of fluoride (20). Figure 1 is a diagram that gives a summary of fluoride metabolism. Several animal epidemiological studies have confirmed that excessive fluoride concentrations could damage the liver and kidneys (21).

Water fluoridation
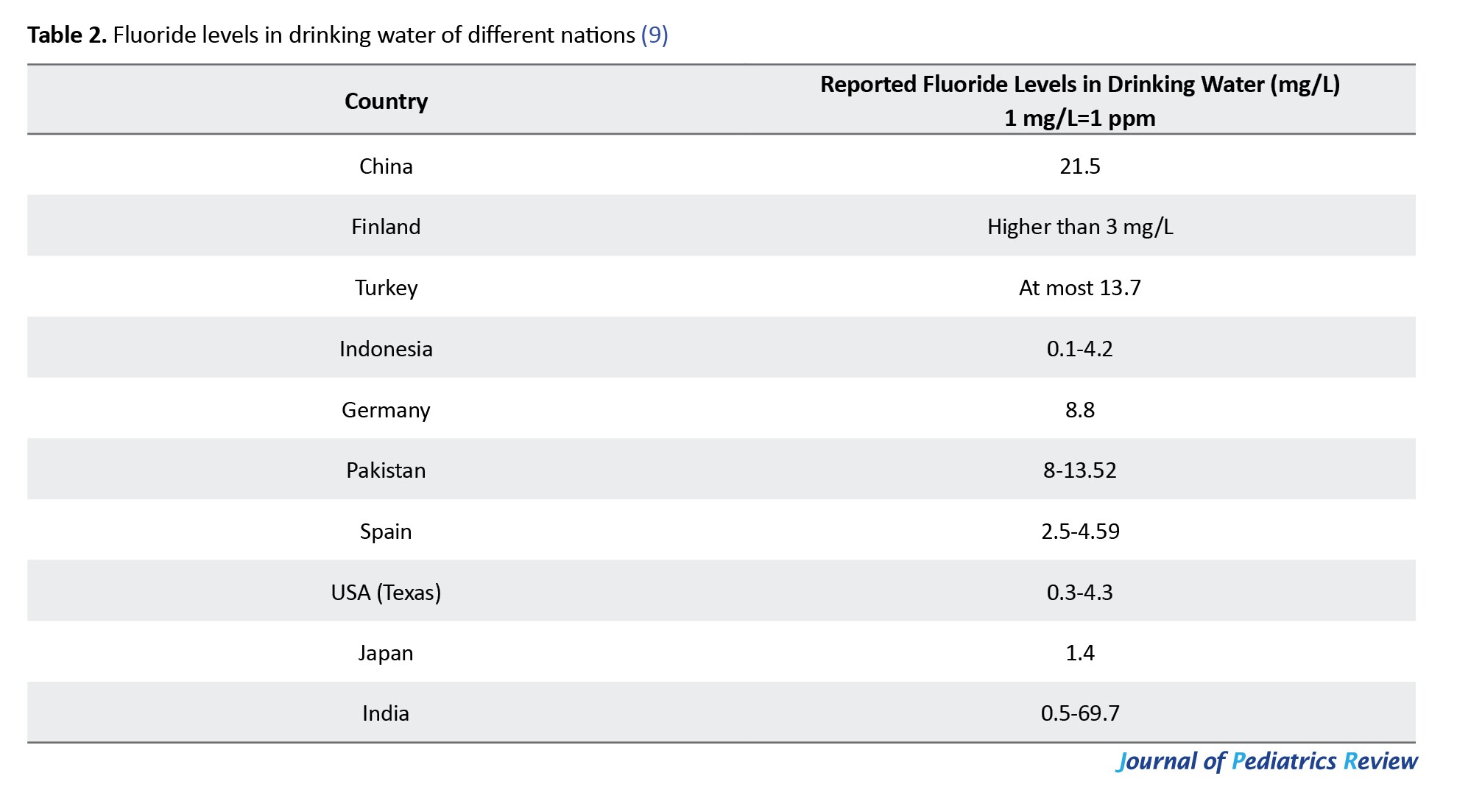
Water fluoridation is an effective way to establish good oral health (22). When fluoride is exposed to teeth surfaces, it bonds with hydroxyapatite crystals and increases their resistance against acids; therefore, it reduces the dental caries progression (23). Water fluoridation is an effective remedy for preventing dental caries due to establishing fluorohydroxyapatite crystals and their higher resistance against microorganisms. This method is routinely used in developed countries (24). Water fluoridation should be done under control because excessive fluoride in drinking water can lead to fluorosis (25). In the united states, water fluoridation was introduced in the 1940s at the level of 0.7 to 1.2 ppm (26). According to Table 2, due to the high concentration of fluoride in some regions of countries such as China, Turkey, and Pakistan, a method should remove excessive fluoride from public and individual water supplies (9).
The beneficial effect of fluoride upon dental health
Topical use of fluoride leads to the prevention of dental caries via several mechanisms described below. As we know, hydroxyapatite crystals are the main mineral components in the teeth’s enamel (27). When fluoride ions bond to hydroxyapatite, they form fluorohydroxyapatite crystals, which are more resistant to dissolution in acidic conditions that occur in dental caries (28).

(hydroxyapatite) (fluorapatite)
According to this formula, fluoride ions replace hydroxyl ions in the hydroxyapatite crystal. Since fluoride ions are much bigger than hydroxyl ions, they increase hydrogen bonding and the density of crystal lattice, therefore, decrease the solubility of the crystals in an acidic environment (29).
The caries preventive effect of fluoride may also occur due to the inhibition of enzymes involved in glycolysis processes such as enolase and proton releasing adenosine triphosphatase (ATPase) (30). Dental caries is the most common chronic diseases in children all around the world. It is proved that fluoride exposure can provide the highest protection against dental caries (31).
Toxicity of fluoride
Fluoride toxicity is classified into chronic and acute toxicity. Excessive ingestion of fluoride in a short time can result in acute toxicity. Nausea, vomiting, abdominal pain, and diarrhea are early symptoms of acute fluoride toxicity that can be followed by shallow breathing, cyanosis, dilated pupils, spasms of extremities, hypotension, respiratory acidosis, and convulsion. Generally, death from high doses of fluoride ingestion can occur within a few hours (32).
According to previous studies, the Probable Toxic Dose (PTD) of fluoride was defined at 5 mg/kg of body weight, as mentioned in Table 3 for different age groups.

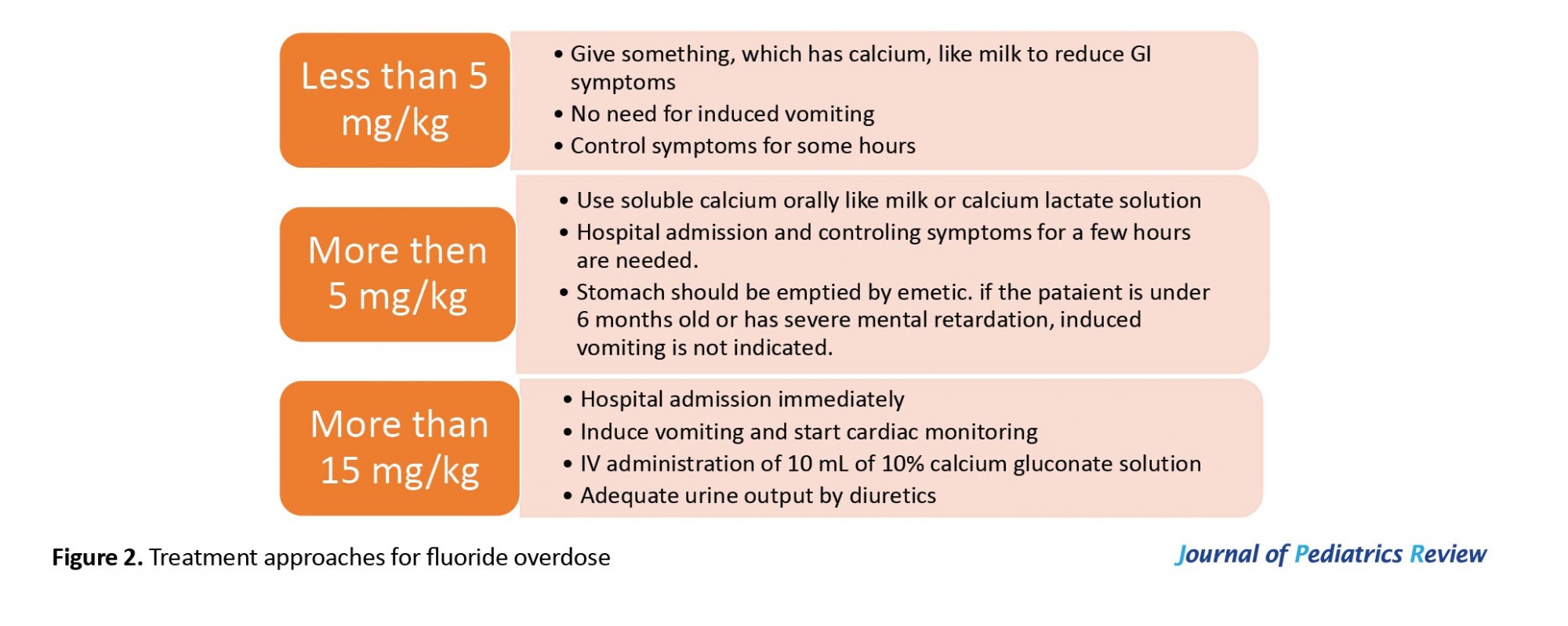
PTD is the dose of a substance in the body that higher than this level that can be associated with life-threatening symptoms that may require immediate treatment. Emergency treatment is needed when the PTD of 15 mg/kg has been exceeded (33). Figure 2 demonstrates some emergency treatments that could be used in the case of fluoride overdose.
Dental fluorosis, as a type of chronic fluoride toxicity, is defined as hypo-mineralization of the enamel that can occur during the first few years of life due to excessive exposure to fluoride (6). The severity of this disorder depends on the dose of fluoride, duration of exposure, and age of the individuals (34). Yellowish or brownish striations on teeth, deformity of enamel and dentin, and interference with enamel mineralization are the main clinical manifestations of dental fluorosis (20). In 1934, Dean created an index commonly used for classifying different types of dental fluorosis (35). Table 4 demonstrates the Dean’s fluorosis index.

Usually, young children tend to swallow toothpaste and are at a higher risk of developing dental fluorosis because they are typically unable to rinse out toothpaste from their mouths (36). Therefore, the primary source of dental fluorosis remains inside oral hygiene products (37). The severity of dental fluorosis lesions increases when the amount of fluoride in drinking water exceeds from 0.7 ppm (2).
However, the mechanism of chronic fluoride toxicity in the whole body is not yet clearly understood. Some studies reported that oxidative stress is one of the essential mechanisms of toxicity in dental fluorosis. Oxidative stress is defined as the imbalance between the production rate of free radicals and the effects of protective antioxidants in the body (38). Chronic fluorosis can induce the generation of free radicals and also inhibit the enzymatic antioxidant defense system in the body that can lead to cellular damage (39).
Fluoride and alteration on thyroid function
High fluoride concentrations (100-200 ppm) can interfere with normal thyroid function. It can increase Thyroid-Stimulating Hormone (TSH) and decreases the levels of T4 and T3 hormones and consequently leads to hypothyroidism (40) So, in areas which fluoride intake is exceptionally high, the secretion of thyroid hormones can be affected (41). Fluoride interferes with the activity of enzymes that accelerate the conversion of thyroxin into active hormones. According to an experimental study conducted by Rahman and Fetouh, sodium fluoride exposure led to thyrocytes’ structural and functional damage. Therefore the production of thyroid hormones is disturbed (42).
Fluoride effect on neuronal health
Recent studies showed that exposure to a high fluoride concentration has a destructive impact on mental development, such as Intelligence Quotient (IQ) in children (43). For example, in a meta-analysis review study conducted in China, it was observed that children who live in areas where fluorosis is prevalent have 5 times lower IQ compared to those who live in areas where fluorosis is scarce (44). The developmental neurotoxicity associated with fluoride is a significant concern these days (45). Ingesting a high amount of fluoride can cause brain-specific metabolic disorders because fluoride can inhibit several neuronal enzymes (46). The brain damage mechanism is related to different reactions such as increased myelin-associated glycoprotein levels, a decrease in nicotinic receptors, changes in phospholipid content, and some other reactions (47). Vani and Reddy conducted a study on mice to analyze the effects of fluoride on some brain enzymes. They concluded that high doses of fluoride in the hippocampus causes degeneration of neurons and changes in free radical metabolism (48).
Fluoride effect on soft tissue
Excessive fluoride exposure has a destructive impact on different soft tissues, including the lungs, kidney, liver, and heart (20). Many studies have declared that the adverse effects of fluoride on soft tissues might be associated with free radicals and oxidative stress (49). For example, the ingestion of excessive fluoride can elevate liver enzymes levels and decreases plasma antioxidant status (20, 50). Song et al. showed in an in vivo experiment that ingestion of high sodium fluoride levels stimulates apoptosis pathways and DNA damage in rats (51).
Developmental effects of fluoride
There are three types of developmental disorders caused by excessive fluoride intake: Closed spina bifida, sudden infant death, Down’s syndrome (52). Some studies show that excessive fluoride intake has adverse developmental effects in animals, but human studies are inconclusive (20). Table 5 gives a summary of the effects of fluoride mentioned in this article.

Fluoride is generally found in our daily diet regimen. It exists in different concentrations in many foods that are mentioned in Table 1 (5). Various fluoride sources include fluoride supplements, fluoride dentifrices, fluoride in water, and foodstuffs (7, 8).
In a previous study, Cardoso et al. reported that the amount of fluoride intake through dentifrices was higher than that through diet (11). Mizira et al. reported the intake of fluoride via dentifrices as 56.3%, water 17.2%, food 11.8%, and in other beverages, this amount was reported 14.7%. It should be noted that this study was conducted in a region with fluoridated water (12). The concentration of fluoride in toothpaste is approximately 0.1% or 1000 ppm (6).
Several organizations, such as the United States Food and Drug Administration, recommended using a smear of toothpaste (a portion the size of a grain of rice) for children under 2 years old and also a pea-size for children younger than 6 years old (13).
Fluoride metabolism
Approximately 90% of ingested fluoride is absorbed from the Gastrointestinal (GI) tract, and the remainder is excreted in the feces (14). Fluoride is bounded to proteins in the plasma; the peak concentration of fluoride in the blood reaches about 20-60 minutes after consumption (15). The concentration of fluoride in the blood is approximately 1% ppm. Fluoride retention in different organs is around 30% in adults and 50% in children. About 99% of these amounts are present in mineralized tissues (teeth and bones), and the remaining 1% is stored in soft tissues (15). Kidney is the main organ responsible for fluoride excretion. Excretion from other sources (such as saliva and sweat) is negligible (14).
Generally, various factors can affect fluoride metabolism, such as acid-base disorders, physical activity, diet, genetics, and kidney function (15). When the fluoride concentration is low, it can enter into the placenta from the mother’s body (16). If its concentration exceeds 0.4 ppm, the placenta acts as a protective barrier and prevents additional fluoride from penetrating the fetus (16, 17). Fluoride can be transmitted to the mothers’ milk, but its concentration is low (18).
The liver is a major site of metabolism in the body; therefore, it is especially prone to fluoride intoxication (19). On the other hand, the kidney is also susceptible to toxicity induced by fluoride as it is the main organ responsible for the excretion of fluoride (20). Figure 1 is a diagram that gives a summary of fluoride metabolism. Several animal epidemiological studies have confirmed that excessive fluoride concentrations could damage the liver and kidneys (21).
Water fluoridation
Water fluoridation is an effective way to establish good oral health (22). When fluoride is exposed to teeth surfaces, it bonds with hydroxyapatite crystals and increases their resistance against acids; therefore, it reduces the dental caries progression (23). Water fluoridation is an effective remedy for preventing dental caries due to establishing fluorohydroxyapatite crystals and their higher resistance against microorganisms. This method is routinely used in developed countries (24). Water fluoridation should be done under control because excessive fluoride in drinking water can lead to fluorosis (25). In the united states, water fluoridation was introduced in the 1940s at the level of 0.7 to 1.2 ppm (26). According to Table 2, due to the high concentration of fluoride in some regions of countries such as China, Turkey, and Pakistan, a method should remove excessive fluoride from public and individual water supplies (9).
The beneficial effect of fluoride upon dental health
Topical use of fluoride leads to the prevention of dental caries via several mechanisms described below. As we know, hydroxyapatite crystals are the main mineral components in the teeth’s enamel (27). When fluoride ions bond to hydroxyapatite, they form fluorohydroxyapatite crystals, which are more resistant to dissolution in acidic conditions that occur in dental caries (28).
(hydroxyapatite) (fluorapatite)
According to this formula, fluoride ions replace hydroxyl ions in the hydroxyapatite crystal. Since fluoride ions are much bigger than hydroxyl ions, they increase hydrogen bonding and the density of crystal lattice, therefore, decrease the solubility of the crystals in an acidic environment (29).
The caries preventive effect of fluoride may also occur due to the inhibition of enzymes involved in glycolysis processes such as enolase and proton releasing adenosine triphosphatase (ATPase) (30). Dental caries is the most common chronic diseases in children all around the world. It is proved that fluoride exposure can provide the highest protection against dental caries (31).
Toxicity of fluoride
Fluoride toxicity is classified into chronic and acute toxicity. Excessive ingestion of fluoride in a short time can result in acute toxicity. Nausea, vomiting, abdominal pain, and diarrhea are early symptoms of acute fluoride toxicity that can be followed by shallow breathing, cyanosis, dilated pupils, spasms of extremities, hypotension, respiratory acidosis, and convulsion. Generally, death from high doses of fluoride ingestion can occur within a few hours (32).
According to previous studies, the Probable Toxic Dose (PTD) of fluoride was defined at 5 mg/kg of body weight, as mentioned in Table 3 for different age groups.
PTD is the dose of a substance in the body that higher than this level that can be associated with life-threatening symptoms that may require immediate treatment. Emergency treatment is needed when the PTD of 15 mg/kg has been exceeded (33). Figure 2 demonstrates some emergency treatments that could be used in the case of fluoride overdose.
Dental fluorosis, as a type of chronic fluoride toxicity, is defined as hypo-mineralization of the enamel that can occur during the first few years of life due to excessive exposure to fluoride (6). The severity of this disorder depends on the dose of fluoride, duration of exposure, and age of the individuals (34). Yellowish or brownish striations on teeth, deformity of enamel and dentin, and interference with enamel mineralization are the main clinical manifestations of dental fluorosis (20). In 1934, Dean created an index commonly used for classifying different types of dental fluorosis (35). Table 4 demonstrates the Dean’s fluorosis index.
Usually, young children tend to swallow toothpaste and are at a higher risk of developing dental fluorosis because they are typically unable to rinse out toothpaste from their mouths (36). Therefore, the primary source of dental fluorosis remains inside oral hygiene products (37). The severity of dental fluorosis lesions increases when the amount of fluoride in drinking water exceeds from 0.7 ppm (2).
However, the mechanism of chronic fluoride toxicity in the whole body is not yet clearly understood. Some studies reported that oxidative stress is one of the essential mechanisms of toxicity in dental fluorosis. Oxidative stress is defined as the imbalance between the production rate of free radicals and the effects of protective antioxidants in the body (38). Chronic fluorosis can induce the generation of free radicals and also inhibit the enzymatic antioxidant defense system in the body that can lead to cellular damage (39).
Fluoride and alteration on thyroid function
High fluoride concentrations (100-200 ppm) can interfere with normal thyroid function. It can increase Thyroid-Stimulating Hormone (TSH) and decreases the levels of T4 and T3 hormones and consequently leads to hypothyroidism (40) So, in areas which fluoride intake is exceptionally high, the secretion of thyroid hormones can be affected (41). Fluoride interferes with the activity of enzymes that accelerate the conversion of thyroxin into active hormones. According to an experimental study conducted by Rahman and Fetouh, sodium fluoride exposure led to thyrocytes’ structural and functional damage. Therefore the production of thyroid hormones is disturbed (42).
Fluoride effect on neuronal health
Recent studies showed that exposure to a high fluoride concentration has a destructive impact on mental development, such as Intelligence Quotient (IQ) in children (43). For example, in a meta-analysis review study conducted in China, it was observed that children who live in areas where fluorosis is prevalent have 5 times lower IQ compared to those who live in areas where fluorosis is scarce (44). The developmental neurotoxicity associated with fluoride is a significant concern these days (45). Ingesting a high amount of fluoride can cause brain-specific metabolic disorders because fluoride can inhibit several neuronal enzymes (46). The brain damage mechanism is related to different reactions such as increased myelin-associated glycoprotein levels, a decrease in nicotinic receptors, changes in phospholipid content, and some other reactions (47). Vani and Reddy conducted a study on mice to analyze the effects of fluoride on some brain enzymes. They concluded that high doses of fluoride in the hippocampus causes degeneration of neurons and changes in free radical metabolism (48).
Fluoride effect on soft tissue
Excessive fluoride exposure has a destructive impact on different soft tissues, including the lungs, kidney, liver, and heart (20). Many studies have declared that the adverse effects of fluoride on soft tissues might be associated with free radicals and oxidative stress (49). For example, the ingestion of excessive fluoride can elevate liver enzymes levels and decreases plasma antioxidant status (20, 50). Song et al. showed in an in vivo experiment that ingestion of high sodium fluoride levels stimulates apoptosis pathways and DNA damage in rats (51).
Developmental effects of fluoride
There are three types of developmental disorders caused by excessive fluoride intake: Closed spina bifida, sudden infant death, Down’s syndrome (52). Some studies show that excessive fluoride intake has adverse developmental effects in animals, but human studies are inconclusive (20). Table 5 gives a summary of the effects of fluoride mentioned in this article.
4. Conclusion
Fluoride is present in our daily lives. We are exposed to fluoride through different sources such as fluoride supplements. Fluoride is beneficial for our dental health and bone growth, but it can be toxic in high concentrations and cause various problems such as dental fluorosis. Brown stains, deformity of enamel and dentin, and change in the color of teeth can be signs of dental fluorosis and is essential to notice. Also, if the fluoride concentration is between 100-200 ppm, it can interfere with normal thyroid function. Although using high doses of fluoride has adverse effects, it can improve children’s dental health in several ways, especially preventing caries.
Ethical Considerations
Compliance with ethical guidelines
This was a review study and did not require ethical considerations.
Funding
This study was supported by the Student Research Committee of Mazandaran University of Medical Sciences.
Authors' contributions
Conceptualization: Azam Nahvi, Pegah Nasiri; Methodology: Milad Arab-nozari; Investigation: Pegah Nasiri, Nadia Elyassi Gorgi; Writing – original draft: All authors; Writing – review & editing: Ali Malekzadeh Shafaroudi; Supervision: Azam Nahvi, Ali Malekzadeh Shafaroudi.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank and appreciate the Deputy Director General of Research and Technology of Mazandaran University of Medical Sciences and the Student Research Committee of the Faculty of Dentistry.
References
- Dey S, Giri B. Fluoride fact on human health and health problems: A review. Reviews in Clinical Medicine. 2016; 2(1):11. [DOI:10.21767/2471-299X.1000011]
- Medjedovic E, Medjedovic S, Deljo D, Sukalo A. Impact of fluoride on dental health quality. Materia Socio-Medica. 2015; 27(6):395-8. [DOI:10.5455/msm.2015.27.395-398] [PMID] [PMCID]
- Dean JA. McDonald and Avery’s Dentistry for the child and adolescent-e-book. Elsevier Health Sciences; 2015.
- Guo H, Kuang P, Luo Q, Cui H, Deng H, Liu H, et al. Effects of sodium fluoride on blood cellular and humoral immunity in mice. Oncotarget. 2017; 8(49):85504. [DOI:10.18632/oncotarget.20198] [PMID] [PMCID]
- Kanduti D, Sterbenk P, Artnik B. Fluoride: A review of use and effects on health. Materia Socio Medica. 2016; 28(2):133. [DOI:10.5455/msm.2016.28.133-137] [PMID] [PMCID]
- Yeung CA. A systematic review of the efficacy and safety of fluoridation. Evidence-Based Dentistry. 2008; 9(2):39-43. https://www.nature.com/articles/6400578
- Barbier O, Arreola-Mendoza L, Del Razo LM. Molecular mechanisms of fluoride toxicity. Chemico-Biological Interactions. 2010; 188(2):319-33. [DOI:10.1016/j.cbi.2010.07.011] [PMID]
- Edmunds W, Smedley P. Groundwater geochemistry and health: An overview. Geological Society, London, Special Publications. 1996; 113(1):91-105. [DOI:10.1144/GSL.SP.1996.113.01.08]
- Mumtaz N, Pandey G, Labhasetwar P K. Global fluoride occurrence, available technologies for fluoride removal and electrolytic defluoridation: A review. Critical Reviews in Environmental Science and Technology. 2015. [DOI:10.1080/10643389.2015.1046768]
- Yadav KK, Kumar S, Pham QB, Gupta N, Rezania S, Kamyab H, et al. Fluoride contamination, health problems and remediation methods in Asian groundwater: A comprehensive review. Ecotoxicology and Environmental Safety. 2019; 182:109362. [DOI:10.1016/j.ecoenv.2019.06.045] [PMID]
- Ophaug R, Singer L, Harland B. Dietary fluoride intake of 6-month and 2-year-old children in four dietary regions of the United States. The American Journal of Clinical Nutrition. 1985; 42(4):701-7. [DOI:10.1093/ajcn/42.4.701] [PMID]
- Schamschula R, Duppenthaler J, Sugar E, Un P, Toth K, Barmes D. Fluoride intake and utilization by Hungarian children: associations and interrelationships. Acta Physiologica Hungarica. 1988; 72(2):253-61. [PMID]
- Wright JT, Hanson N, Ristic H, Whall CW, Estrich CG, Zentz RR. Fluoride toothpaste efficacy and safety in children younger than 6 years: A systematic review. The Journal of the American Dental Association. 2014; 145(2):182-9. [DOI:10.14219/jada.2013.37] [PMID]
- Fawell J, Bailey K, Chilton J, Dahi E, Magara Y. Fluoride in drinking-water. London: IWA Publishing; 2006.
- Buzalaf MAR, Whitford GM. Fluoride metabolism. Fluoride and the Oral Environment. 2011; (22):20-36.[DOI:10.1159/000325107] [PMID]
- Gurumurthy Sastry M, Mohanty S, Rao P. Role of placenta to combat fluorosis (in fetus) in endemic fluorosis area. National Journal of Integrated Research in Medicine. 2010; 1(4):16-9. https://imsear.searo.who.int/handle/123456789/152582
- Gupta S, Seth A, Gupta A, Gavane A. Transplacental passage of fluorides. The Journal of Pediatrics. 1993; 123(1):139-41. [DOI:10.1016/S0022-3476(05)81558-6]
- Ekstrand J, Boreus L, De Chateau P. No evidence of transfer of fluoride from plasma to breast milk. British Medical Journal (Clinical research ed). 1981; 283(6294):761. [DOI:10.1136/bmj.283.6294.761] [PMID] [PMCID]
- Wang T L, Maierhofer C, Speicher M R, Lengauer C, Vogelstein B, Kinzler K W, et al. Digital karyotyping. Proceedings of the National Academy of Sciences. 2002; 99(25):16156-61. [DOI:10.1073/pnas.202610899] [PMID] [PMCID]
- Kabir H, Gupta AK, Tripathy S. Fluoride and human health: Systematic appraisal of sources, exposures, metabolism, and toxicity. Critical Reviews in Environmental Science and Technology. 2020; 50(11):1116-93. [DOI:10.1080/10643389.2019.1647028]
- Xiong X, Liu J, He W, Xia T, He P, Chen X, et al. Dose-effect relationship between drinking water fluoride levels and damage to liver and kidney functions in children. Environmental Research. 2007; 103(1):112-6. [DOI:10.1016/j.envres.2006.05.008] [PMID]
- O’Connell J, Rockell J, Ouellet J, Tomar SL, Maas W. Costs and savings associated with community water fluoridation in the United States. Health Affairs. 2016; 35(12):2224-32. [DOI:10.1377/hlthaff.2016.0881] [PMID]
- Pajor K, Pajchel L, Kolmas J. Hydroxyapatite and fluorapatite in conservative dentistry and oral implantology-a review. Materials. 2019; 12(17):2683. [DOI:10.3390/ma12172683] [PMID] [PMCID]
- Iheozor‐Ejiofor Z, Worthington H V, Walsh T, O’Malley L, Clarkson J E, Macey R, et al. Water fluoridation for the prevention of dental caries. Cochrane Database of Systematic Reviews. 2015; (6). [DOI:10.1002/14651858.CD010856.pub2]
- Tulchinsky TH, Varavikova EA. The new public health Cambridge. Cambridge: Academic Press; 2014.
- Tinanoff N. Dental caries. Pediatric Dentistry: Elsevier; 2019.
- Fincham A, Moradian-Oldak J, Simmer J. The structural biology of the developing dental enamel matrix. Journal of Structural Biology. 1999; 126(3):270-99. [DOI:10.1006/jsbi.1999.4130] [PMID]
- Buzalaf MAR, Pessan JP, Honório HM, Ten Cate JM. Mechanisms of action of fluoride for caries control. Fluoride and the oral environment. Fluoride and the Oral Environment. 2011; (22):97-114. [DOI:10.1159/000325151] [PMID]
- Brown W, Gregory T, Chow L. Effects of fluoride on enamel solubility and cariostasis. Caries Research. 1977; 11(Suppl. 1):118-41. [DOI:10.1159/000260298] [PMID]
- Sutton S, Bender GR, Marquis RE. Fluoride inhibition of proton-translocating ATPases of oral bacteria. Infection and Immunity. 1987; 55(11):2597-603. [DOI:10.1128/IAI.55.11.2597-2603.1987] [PMID] [PMCID]
- Ijaz S, Croucher R, Onwude O, Rutterford C, Marinho VC. Professionally applied fluoride paint‐on solutions for the control of dental caries in children and adolescents. The Cochrane Database of Systematic Reviews. 2018; 2018(5):CD008364. [DOI:10.1002/14651858.CD008364.pub2] [PMCID]
- Featherstone J. The continuum of dental caries-evidence for a dynamic disease process. Journal of Dental Research. 2004; 83(1_suppl):39-42. [DOI:10.1177/154405910408301s08] [PMID]
- Whitford G M. Acute toxicity of ingested fluoride. Fluoride and the Oral Environment. 2011; (22):66-80. [DOI:10.1159/000325146] [PMID]
- Fejerskov O, Kidd E. Dental caries: The disease and its clinical management. Hoboken: John Wiley & Sons; 2009.
- Medina-Solis C E, Pontigo-Loyola A P, Maupome G, Lamadrid-Figueroa H, Loyola-Rodríguez J P, Hernández-Romano J, et al. Dental fluorosis prevalence and severity using Dean’s index based on six teeth and on 28 teeth. Clinical oral Investigations. 2008; 12(3):197-202. [DOI:10.1007/s00784-007-0171-7] [PMID]
- Padi S. Review on efficacy and alternative approaches for fluoride toothpaste used in younger children. Dentistry. 2019; 9(538):2161-1122. https://www.longdom.org/open-access/
- Ullah R, Zafar M S, Shahani N. Potential fluoride toxicity from oral medicaments: A review. Iranian Journal Of Basic Medical Sciences. 2017; 20(8):841-8. [PMCID] [PMID]
- Liguori I, Russo G, Curcio F, Bulli G, Aran L, Della-Morte D, et al. Oxidative stress, aging, and diseases. Clinical Interventions in Aging. 2018; 13:757. [DOI:10.2147/CIA.S158513] [PMID] [PMCID]
- Guney M, Oral B, Take G, Giray S G, Mungan T. Effect of fluoride intoxication on endometrial apoptosis and lipid peroxidation in rats: Role of vitamins E and C. Toxicology. 2007; 231(2-3):215-23. [DOI:10.1016/j.tox.2006.12.020] [PMID]
- Basha P M, Rai P, Begum S. Fluoride toxicity and status of serum thyroid hormones, brain histopathology, and learning memory in rats: A multigenerational assessment. Biological Trace Element Research. 2011; 144(1-3):1083-94. [DOI:10.1007/s12011-011-9137-3] [PMID]
- Sarkar C, Pal S. Ameliorative effect of resveratrol against fluoride-induced alteration of thyroid function in male Wistar rats. Biological Trace Element Research. 2014; 162(1-3):278-87. [DOI:10.1007/s12011-014-0108-3] [PMID]
- Rahman M M A, Fetouh F A. Effect of sodium fluoride on the thyroid follicular cells and the amelioration by calcium supplementation in Albino rats: A light and an electron microscopic study. Journal of American Science. 2013; 9(10):107-14. https://www.researchgate.net/profile/Fathy_Fetouh3/publication/262731572_
- Peckham S, Awofeso N. Water fluoridation: A critical review of the physiological effects of ingested fluoride as a public health intervention. The Scientific World Journal. 2014; 2014:293019. [DOI:10.1155/2014/293019] [PMID] [PMCID]
- Choi AL, Sun G, Zhang Y, Grandjean P. Developmental fluoride neurotoxicity: A systematic review and meta-analysis. Environmental Health Perspectives. 2012; 120(10):1362-8. [DOI:10.1289/ehp.1104912] [PMID] [PMCID]
- Yu X, Chen J, Li Y, Liu H, Hou C, Zeng Q, et al. Threshold effects of moderately excessive fluoride exposure on children’s health: A potential association between dental fluorosis and loss of excellent intelligence. Environment International. 2018; 118:116-24. [DOI:10.1016/j.envint.2018.05.042] [PMID]
- Zuo H, Chen L, Kong M, Qiu L, Lü P, Wu P, et al. Toxic effects of fluoride on organisms. Life Sciences. 2018; 198:18-24. [DOI:10.1016/j.lfs.2018.02.001] [PMID]
- Banala RR, Karnati PR. Vitamin A deficiency: An oxidative stress marker in sodium fluoride (NaF) induced oxidative damage in developing rat brain. International Journal of Developmental Neuroscience. 2015; 47:298-303. [DOI:10.1016/j.ijdevneu.2015.08.010] [PMID]
- Vani ML, Reddy KP. Effects of fluoride accumulation on some enzymes of brain and gastrocnemius muscle of mice. Fluoride. 2000; 33(1):17-26. http://www.mercurioenlaboca.org/comunidad/uploads/FileUpload/94/8eb23f3cdf69079fa3b481ae7fcf60.pdf
- Ekambaram P, Namitha T, Bhuvaneswari S, Aruljothi S, Vasanth D, Saravanakumar M. Therapeutic efficacy of Tamarindus indica (L) to protect against fluoride-induced oxidative stress in the liver of female rats. Fluoride. 2010; 43(2):134-40. https://www.researchgate.net/profile/Ekambaram_Perumal/publication/268428354_
- Niu R, Han H, Sun Z, Zhang Y, Yin W, Wang J, et al. Effects of fluoride exposure on the antioxidative status in the kidneys of offspring mice during the embryonic and suckling phases. Fluoride. 2016; 49(1):5-12. https://www.fluorideresearch.org/491/files/FJ2016_v49_n1_p005-012_sfs.pdf
- Song GH, Gao JP, Wang CF, Chen CY, Yan XY, Guo M, et al. Sodium fluoride induces apoptosis in the kidney of rats through caspase-mediated pathways and DNA damage. Journal of Physiology and Biochemistry. 2014; 70(3):857-68. [DOI:10.1007/s13105-014-0354-z] [PMID]
- Doull J, Boekelheide K, Farishian B, Isaacson R, Klotz J, Kumar J, et al. Fluoride in drinking water: A scientific review of EPA’s standards. Washington: National Academies; 2006. https://books.google.com/books?
Type of Study: Narrative Review |
Subject:
Pediatrics
Received: 2019/12/23 | Accepted: 2020/09/5 | Published: 2021/01/21
Received: 2019/12/23 | Accepted: 2020/09/5 | Published: 2021/01/21
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Articles Copyright © The Author(s).
Owned by Mazandaran University of Medical Sciences.
Published by Negah Institute for Scientific Communication.
Journal of Pediatrics Review (JPR)
Bou Ali Sina Hospital, Pasdaran Boulevard, Sari, Iran.
Journal Tel: +98 - 1133342331
Publisher Tel: +9821 8603 6497-
+9821 8603 7228 (EXT: 104)
Website: http://jpr.mazums.ac.ir/
E-mail: jpr.mazums@gmail.com,
jpr@mazums.ac.ir
