
Mon, Jul 27, 2026


Volume 8, Issue 3 (7-2020)
J. Pediatr. Rev 2020, 8(3): 163-174 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abedian Kasgari K, Peyman N, Momeni Badeleh S, Gholian Avval M, Momeni Badeleh K, Vahedian Shahroodi M et al . Health Literacy Measurement in Childhood: A Systematic Review. J. Pediatr. Rev 2020; 8 (3) :163-174
URL: http://jpr.mazums.ac.ir/article-1-260-en.html
URL: http://jpr.mazums.ac.ir/article-1-260-en.html
Kobra Abedian Kasgari1 
 , Nooshin Peyman2 , Safa Momeni Badeleh3 , Mehdi Gholian Avval2 , Kosar Momeni Badeleh4 , Mohammad Vahedian Shahroodi2 , Seyedeh Belin Tavakoly Sany *5
, Nooshin Peyman2 , Safa Momeni Badeleh3 , Mehdi Gholian Avval2 , Kosar Momeni Badeleh4 , Mohammad Vahedian Shahroodi2 , Seyedeh Belin Tavakoly Sany *5 
, Nooshin Peyman2 , Safa Momeni Badeleh3 , Mehdi Gholian Avval2 , Kosar Momeni Badeleh4 , Mohammad Vahedian Shahroodi2 , Seyedeh Belin Tavakoly Sany *5
1- Department of Health Education and Health Promotion, Faculty of Health, Mashhad University of Medical Sciences, Mashhad, Iran.
2- Department of Health Education and Health Promotion, Faculty of Health, Mashhad University of Medical Sciences, Mashhad, Iran. & Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Food and Drug Control, School of Pharmacy, Zanjan University of Medical Science, Zanjan, Iran.
4- Department of Science, Islamic Azad University, Sari Branch, Sari, Iran.
5- Department of Health Education and Health Promotion, Faculty of Health, Mashhad University of Medical Sciences, Mashhad, Iran. & Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. ,tavakkolisanib@mums.ac.ir
2- Department of Health Education and Health Promotion, Faculty of Health, Mashhad University of Medical Sciences, Mashhad, Iran. & Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Food and Drug Control, School of Pharmacy, Zanjan University of Medical Science, Zanjan, Iran.
4- Department of Science, Islamic Azad University, Sari Branch, Sari, Iran.
5- Department of Health Education and Health Promotion, Faculty of Health, Mashhad University of Medical Sciences, Mashhad, Iran. & Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. ,
Full-Text [PDF 577 kb]
(2803 Downloads)
| Abstract (HTML) (6987 Views)

Full-Text: (4112 Views)
1. Introduction
From a public health viewpoint, children are among the main target populations for Health Literacy (HL) studies and health educational interventions. This is because, during childhood, fundamental cognitive skills, as well as emotional and physical development processes occur, and health-related behaviors and abilities are developed. Consequently, this stage of life is essential for personal health and welfare during adulthood (1-4). Furthermore, HL is understood as a key construct to attain a life learning action, i.e., begins in early childhood (5-7). Then, target groups of HL interventions could be enabled to reducing health risks and promoting healthy behaviors. In clinical settings, more studies have focused on the impact of maternal and parental HL on children’s health status. Several studies clarified how children are influenced by their parents’ lack of adequate skills and knowledge. Such deficits complicate making health decisions and taking actions regarding their children’s health (1, 2, 8).
Therefore, some studies investigated children’s HL for health promotion in schools (2, 9, 10). Furthermore, there is limited academic agreement and measurement of children concerning the knowledge and skills required to make health decisions. For the European population, the HL consortium included differing dimensions and drivers to recommend HL. HL is “linked to literacy and improves individuals’ knowledge, incentive, and abilities to access, understand, appraise, and use health information”. “Such a process helps to make judgments and take decisions in daily living regarding healthcare, disease prevention, and health promotion to maintain or improve the quality of life” (11, 12). It was evidenced that a specific outline for child HL is missing. Therefore, it is unclear how theoretical actions for demonstrating HL in children identify related trials and do consider the sole features of the target population. Rothman et al. identified 4 classifications of unique requirements and features to balance the child population from the adults. These classes include dependency on skills and resources, developmental changes, vulnerability to social-demographic predictors and health determinants, and epidemiological differences (13). Therefore, we attempted to address these gaps in the present research.
This study aimed to scope the recent definition and understandings of HL in children. Moreover, we attempted to comprehend what available theories and models provide the distinct requirements and characteristics of children. To our knowledge, this systematic review is the first study to investigate the theoretical definitions and understanding of HL in children. This finding could be practical for future HL interventions to promote children’s health.
2. Methods
Six databases, including Scopus, PubMed, Cumulative Index to Nursing, Educational Resources Information Centre (ERIC), Web of Science, and Allied Health Literatures (CINAHL) were searched. We conducted search strategy based on the Medical Subject Heading (MESH) keywords related to term “health competence”, “health literacy”, and combined the following terms: “concept”, “skills”, “model”, “theory”, “framework”, and “childhood”. There were no limitations on the publication time frame, peer-review criteria, or study design.
Interventional and cross-sectional studies with main focuses on generic HL and relevant content for conceptualizing and defining HL in children were included in this study. The papers were included if they met the following criteria: a. full-texts available in English; b. being focused on the HL concept and its core dimensions in childhood, and c. providing the relevant concept for conceptualizing and defining HL in children. The exclusion criteria consisted of letters, reviews, poor quality articles, conference abstracts, and editorials. Initially, two independent authors screened the titles and abstracts of the collected articles. Then, they evaluated the selected full-texts to examine whether the included articles meet the inclusion criteria. The two authors were in 100% agreement over the articles included, and a third reviewer resolved any doubts and discrepancies.
This systematic review was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for ensuring the high quality and clarity of the collected information (12). In this study, HL was considered as a multidimensional construct or dimension for which the available studies were assessed and synthesized. We attempted to extract HL dimensions from available theoretical definitions and models. Overall, 356 articles were identified (Figure 1), and 100 abstracts were selected after removing duplicates. Figure 1 shows that 25 articles met the inclusion criteria and were selected for the full-text analysis. All these selected studies were qualitatively evaluated. First, selected articles were checked for theoretical models and definitions, i.e., adapted for the children, and included pertinent concept on HL of children. Then, we coded these models and definitions following an inductive attitude. The relevant characteristics were extracted, such as the author’s name, the time of research conduction, the age of the target group, models and theories explained, the primary target of study, target participation in development, empirical test, as well as the definitions and identified dimensions of HL. The quality of all studies was assessed by a 12-item checklist; accordingly, those studies that obtained the minimum acceptable score were included in this review.
3. Results
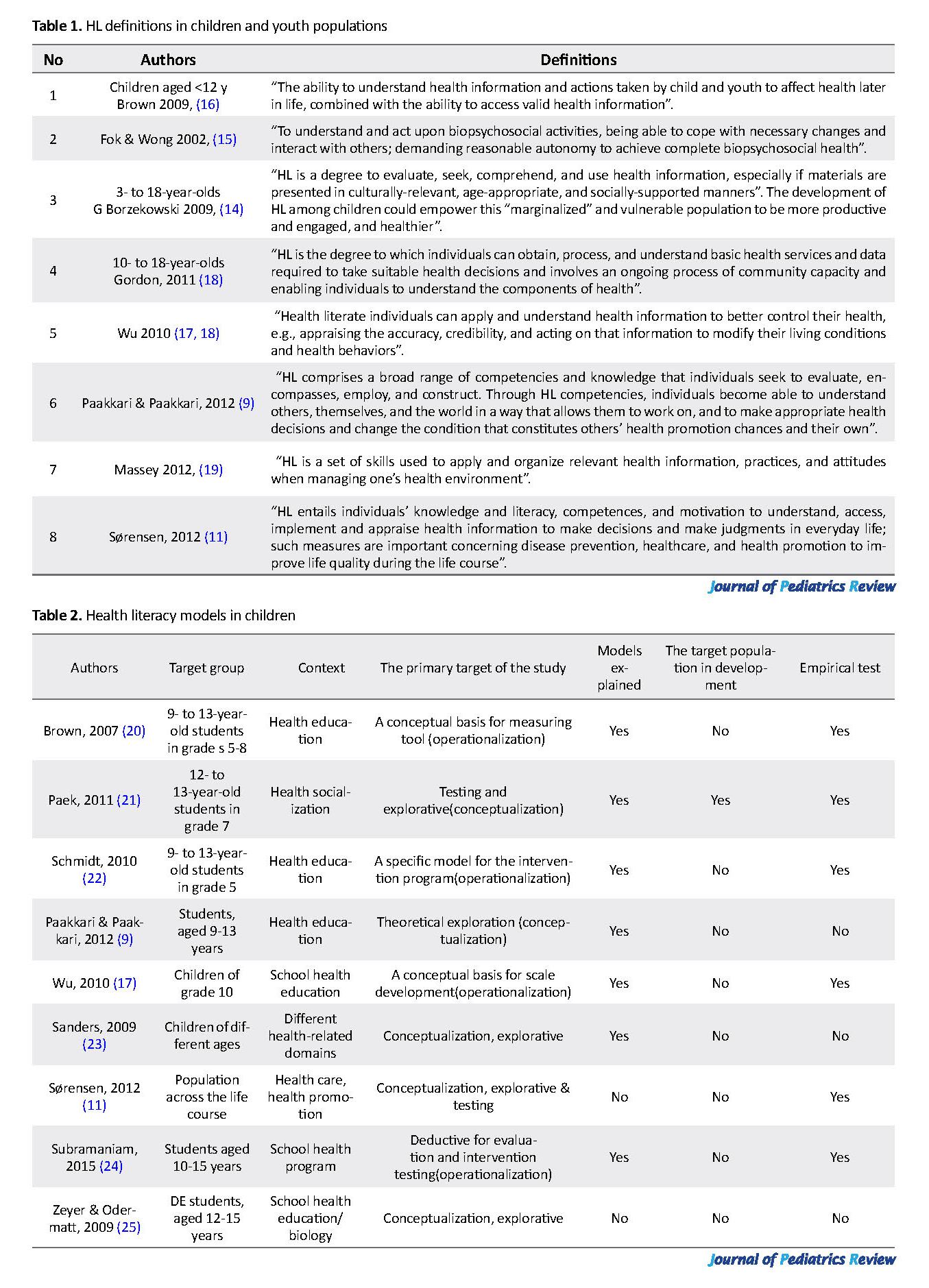
In this review of the literature, 8 definitions (Table 1) and 9 models (Table 2) on children’s HL were presented.
Of the 8 definitions (Table 1), one study was related to children aged 3 to 18 years (14); another two articles targeted children <12 years (15, 16), and 4 definitions targeted 13- to 18-year-olds (9, 17-19). Five definitions focused on a school health education program (9, 11, 17, 18, 20). However, Massey et al. specifically targeted HL in the healthcare system (19).
From a public health viewpoint, children are among the main target populations for Health Literacy (HL) studies and health educational interventions. This is because, during childhood, fundamental cognitive skills, as well as emotional and physical development processes occur, and health-related behaviors and abilities are developed. Consequently, this stage of life is essential for personal health and welfare during adulthood (1-4). Furthermore, HL is understood as a key construct to attain a life learning action, i.e., begins in early childhood (5-7). Then, target groups of HL interventions could be enabled to reducing health risks and promoting healthy behaviors. In clinical settings, more studies have focused on the impact of maternal and parental HL on children’s health status. Several studies clarified how children are influenced by their parents’ lack of adequate skills and knowledge. Such deficits complicate making health decisions and taking actions regarding their children’s health (1, 2, 8).
Therefore, some studies investigated children’s HL for health promotion in schools (2, 9, 10). Furthermore, there is limited academic agreement and measurement of children concerning the knowledge and skills required to make health decisions. For the European population, the HL consortium included differing dimensions and drivers to recommend HL. HL is “linked to literacy and improves individuals’ knowledge, incentive, and abilities to access, understand, appraise, and use health information”. “Such a process helps to make judgments and take decisions in daily living regarding healthcare, disease prevention, and health promotion to maintain or improve the quality of life” (11, 12). It was evidenced that a specific outline for child HL is missing. Therefore, it is unclear how theoretical actions for demonstrating HL in children identify related trials and do consider the sole features of the target population. Rothman et al. identified 4 classifications of unique requirements and features to balance the child population from the adults. These classes include dependency on skills and resources, developmental changes, vulnerability to social-demographic predictors and health determinants, and epidemiological differences (13). Therefore, we attempted to address these gaps in the present research.
This study aimed to scope the recent definition and understandings of HL in children. Moreover, we attempted to comprehend what available theories and models provide the distinct requirements and characteristics of children. To our knowledge, this systematic review is the first study to investigate the theoretical definitions and understanding of HL in children. This finding could be practical for future HL interventions to promote children’s health.
2. Methods
Six databases, including Scopus, PubMed, Cumulative Index to Nursing, Educational Resources Information Centre (ERIC), Web of Science, and Allied Health Literatures (CINAHL) were searched. We conducted search strategy based on the Medical Subject Heading (MESH) keywords related to term “health competence”, “health literacy”, and combined the following terms: “concept”, “skills”, “model”, “theory”, “framework”, and “childhood”. There were no limitations on the publication time frame, peer-review criteria, or study design.
Interventional and cross-sectional studies with main focuses on generic HL and relevant content for conceptualizing and defining HL in children were included in this study. The papers were included if they met the following criteria: a. full-texts available in English; b. being focused on the HL concept and its core dimensions in childhood, and c. providing the relevant concept for conceptualizing and defining HL in children. The exclusion criteria consisted of letters, reviews, poor quality articles, conference abstracts, and editorials. Initially, two independent authors screened the titles and abstracts of the collected articles. Then, they evaluated the selected full-texts to examine whether the included articles meet the inclusion criteria. The two authors were in 100% agreement over the articles included, and a third reviewer resolved any doubts and discrepancies.
This systematic review was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for ensuring the high quality and clarity of the collected information (12). In this study, HL was considered as a multidimensional construct or dimension for which the available studies were assessed and synthesized. We attempted to extract HL dimensions from available theoretical definitions and models. Overall, 356 articles were identified (Figure 1), and 100 abstracts were selected after removing duplicates. Figure 1 shows that 25 articles met the inclusion criteria and were selected for the full-text analysis. All these selected studies were qualitatively evaluated. First, selected articles were checked for theoretical models and definitions, i.e., adapted for the children, and included pertinent concept on HL of children. Then, we coded these models and definitions following an inductive attitude. The relevant characteristics were extracted, such as the author’s name, the time of research conduction, the age of the target group, models and theories explained, the primary target of study, target participation in development, empirical test, as well as the definitions and identified dimensions of HL. The quality of all studies was assessed by a 12-item checklist; accordingly, those studies that obtained the minimum acceptable score were included in this review.
3. Results
In this review of the literature, 8 definitions (Table 1) and 9 models (Table 2) on children’s HL were presented.
Of the 8 definitions (Table 1), one study was related to children aged 3 to 18 years (14); another two articles targeted children <12 years (15, 16), and 4 definitions targeted 13- to 18-year-olds (9, 17-19). Five definitions focused on a school health education program (9, 11, 17, 18, 20). However, Massey et al. specifically targeted HL in the healthcare system (19).
The only research groups that linked empirical and exploratory dimensions to development in defining HL were Fok and Wong (15), as well as Massey and associates (19). Gordon et al. introduced this concept as stakeholder participation with school health community partners (18). Therefore, HL was introduced not limited to reading, writing, or understanding the numbers (14). HL was expressed as a combination of abilities, competencies, health awareness, and an individual’s motivational factors (11). In all definitions, the focus was on collaborative actions that often led to access, process, and the use of health information (11). This required cognitive or behavioral functioning that enables personal empowerment in their life course in certain situations on demand of health-related decision-making or implementing healthcare data and by benefiting the HL, is prepared for actions. Therefore, children were considered as rule-makers who are actively evaluating, processing and seeking health information (knowledge, health services, practices, & attitudes).
They use the obtained data in the health-related decisions-making. This approach could be a strategy for the diagnosis and measurement of HL in children and adolescents (9). Fok and Wong (15) focused not only on health information and practices but also on measures related to biopsychosocial activities in which children participated. They describe the process of accomplishing the specific characteristics that children need to achieve for health and well-being. Moreover, these characteristics include personal health, enjoying school time, emotional stability, and the ability to cope with multiple situations (15). Definitions of HL express one dimension, as well as the medium- and long-term objectives of HL outcomes; they include specific performance concerning health-related decision-making that express the other dimensions, e.g., personal environmental health management (19) or the correct and informed selection (17).
The intermediate- or long-term HL outcomes are generally related to personal health promotion (17); health outcomes address health risks reduction and quality of life improvement (17) or one’s living conditions (18). Borzkfasky (14) believes that children are especially vulnerable, and to some extent, “marginalized” social groups that must be engaged with their health and resist to remain healthier. Paakkari et al. (9) emphasized the social dimension of HL and suggested that HL allows students to identify and change factors that threaten their health and that of the others (15). The first prerequisite for HL is an ability, i.e., the level of reasoning and independence on sociocultural-related health issues and should be presented at an appropriate age (14).
In total, 9 studies defined HL models (Table 2). Five dimensions reconstructed the HL models, either operationally to develop measurement tools (17, 20), or as an impact or assessment model for an intervention program (22, 24). In these studies, HL was examined in terms of several systems (health, community, & educational systems). Besides, numerous fields, such as healthcare, health promotion, and disease prevention are related to health. In the field of school health education, 6 models with 4 articles (20, 22, 24-26) related to children aged <12 years, and 5 articles related to those aged ≥12 years (9, 11, 17, 21, 25) were assessed.
In total, 9 studies defined HL models (Table 2). Five dimensions reconstructed the HL models, either operationally to develop measurement tools (17, 20), or as an impact or assessment model for an intervention program (22, 24). In these studies, HL was examined in terms of several systems (health, community, & educational systems). Besides, numerous fields, such as healthcare, health promotion, and disease prevention are related to health. In the field of school health education, 6 models with 4 articles (20, 22, 24-26) related to children aged <12 years, and 5 articles related to those aged ≥12 years (9, 11, 17, 21, 25) were assessed.
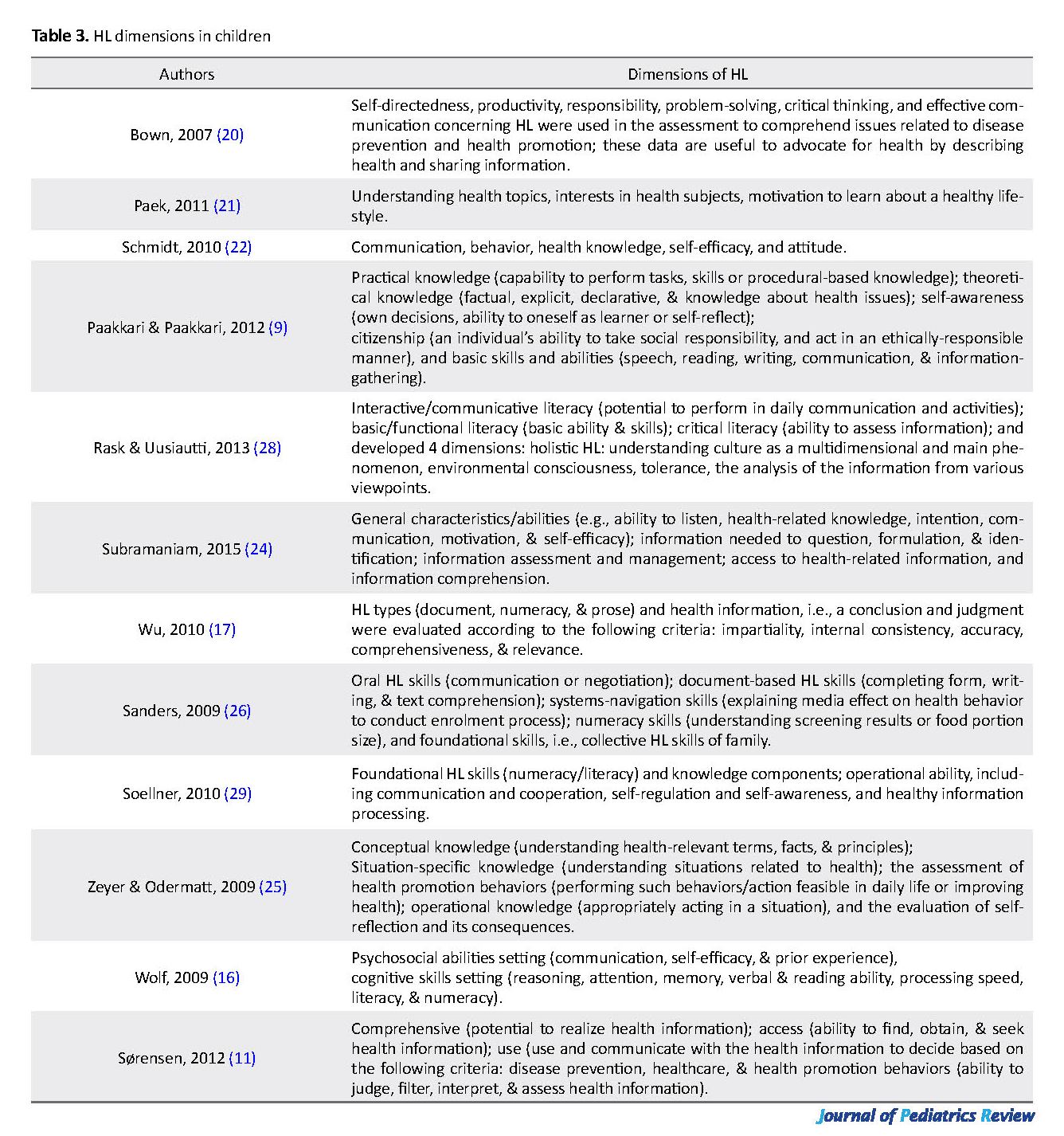
Child HL is defined as a set of capabilities, skills, commitments, and information that allows individuals to access the health information competently and efficiently to benefit from the health-related decision-making and actions. Likewise, our findings suggested the main aspects of children’s HL (Table 3). Due to focus on individual characteristics, the dimensions with three main categories were selected; cognitive (9, 20-22, 27), behavioral or functional (17, 23, 24, 26, 28), and emotional (3, 11, 16, 25, 29).
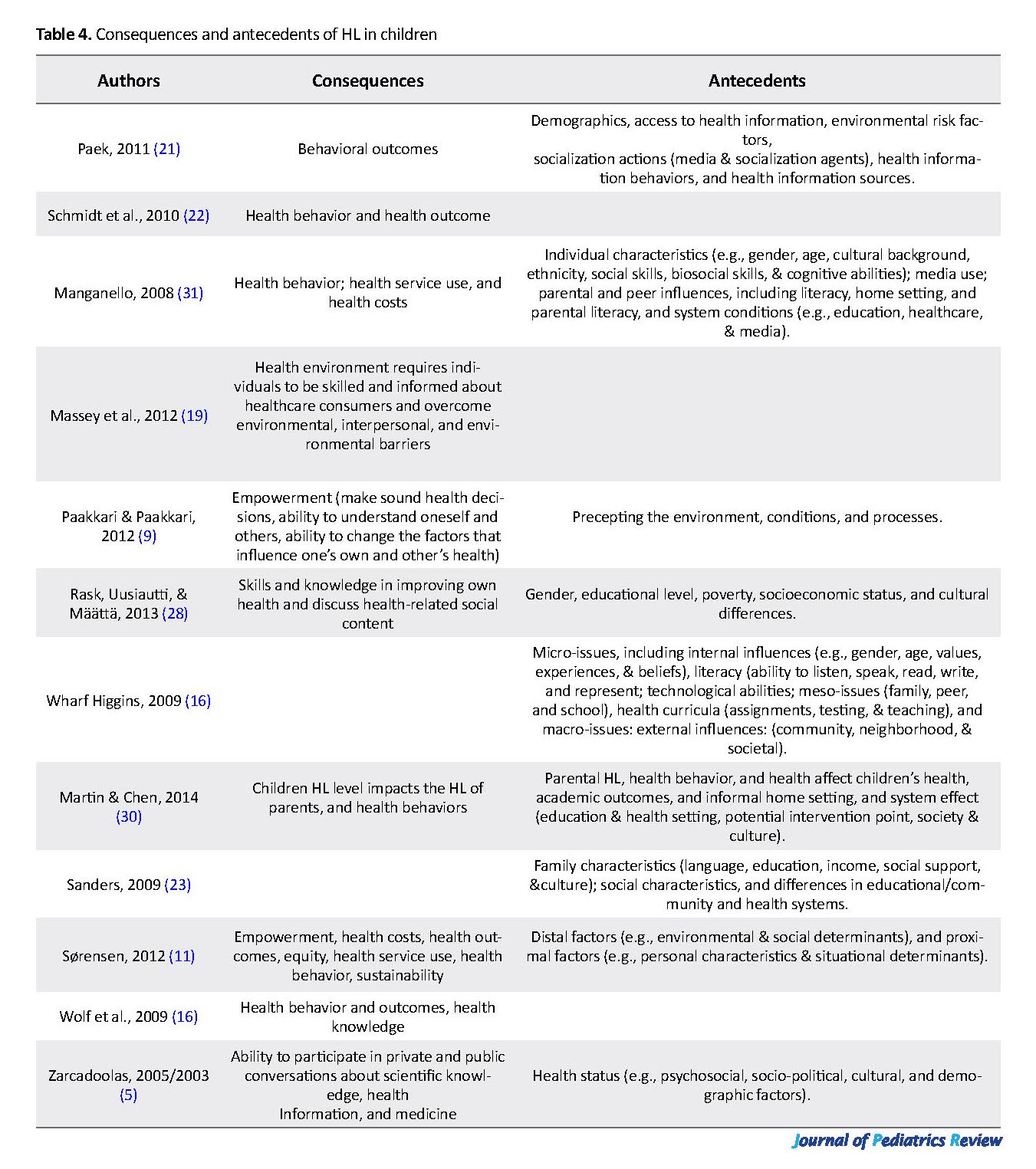
The factors affecting the HL of children and youth or the outcomes, i.e., influenced by HL are listed in Table 4. In the 9 identified models, differentiation has been made between individual characteristics, demographic factors, situation or context, and the broader system (the social factors) (5, 21, 22). These studies highlighted the effect of parental influences and family’s demographic factors. Younger children are more prone to trusting their parents concerning socioeconomic support. In these conditions, the individual’s socioeconomic status or occupation plays no role in these variables (18, 26, 30). Family demographic factors include socioeconomic status, health status, and parental HL.
Martin and Chen (30) reported that these family characteristics significantly impact health status, HL, and educational variables in children. These characteristics include their willingness on going to school and the educational outcomes. In addition, families, schools, and peers are the main socialization factors in children’s lives; they affect their potential for being health literate. Peers and family can encourage or discourage HL practices and health-promotion behaviors through their social supports, norms, and practices (11, 32, 33). Parents and peers could be a role model for achieving and interpreting HL by teaching their children to assess the credibility of the sources from which they obtain information. In this context, the type and quality of communication significantly affect children. This is because children mainly consult with their trusted peers and family. Access to online media and resources also influences their health status. The social level also refers to health, education, social systems, as well as cultural and political forces. This includes the general conditions and learning environment of the individual. Such factors may include the safety of students at school, and the teacher’s skills that could promote reflexing and critical thinking in students (9, 32).
Ten articles suggested that HL in children leads to individual and social benefits (Table 4). At the individual level, HL enables the young population to be skilled users of the healthcare system and to overcome the related interpersonal and environmental problems (14, 17, 27). Moreover, HL allows children to better perceive themselves, others, and the world, discuss health-related social issues and make proper health decisions (9, 21, 28). It is also believed that young people with adequate HL could start and accomplish their health objectives, including participating in physical activity or avoid alcohol consumption (25). Furthermore, HL benefits cover a wide range of living performances, at home, work, community, and even economic levels (5, 11). In terms of communicational and societal benefits, HL could promote participation in community health programs to increase the general capacity and community empowerment; it could eventually impact one’s health, the health of others, and the social norms (9, 16, 34).
4. Discussion
In this review article, we identified 8 definitions and 9 models regarding the HL status for children and young individuals. As a high heterogeneous definition and complex model, HL is a complex concept with multidimensional constructs or dimensions. Furthermore, by explaining these constructs along with multiple integrated classifications, presenting a combination of the HL constructs recovered from the literature seems reasonable (35, 36). However, these definitions may overlap due to different reasons, resulting in differential focuses. These findings are consistent with those of Paakkari and colleagues (4); they highlighted that “there are differences in the components of HL and its associated characteristics” (9, 37). Concerning the first research question, in most definitions and models, the focus of HL is beyond the set of healthcare settings. It seems that HL in children is related to multiple contexts and occasions of daily life that influence the promotion of one’s health and well-being.
HL in children, like adults (11), involves agency and actions which alter according to the HL viewpoint; e.g., from healthcare or clinical setting models to a more general public health or health system and health promotion model (24, 28, 35). As a result, HL is content- and context-specific and concordant with the present contextual factors and the complexity of the task (20). The contextual factors’ influence was supported in the literature; however, they often remained underscored. It was evidenced that the individual characteristics include the skills and knowledge that an individual requires to encounter certain situational requirements. These necessities include the general health center-related situational requirements that communities pose upon an individual (35). Furthermore, the behavioral components of HL are usually not distinguished from the HL outcome (Table 4). Some strong skills and individual-based HL concepts are required for individuals to be actively involved in understanding, seeking, making health-related decisions. Moreover, such skills also facilitate accessing information that reflects children’s everyday lives.
HL models especially focus on the healthcare system; they seem to significantly and primarily view individuals. They adhere to a perspective complying with the professional health instructions and receive the provided health information. Models that target the healthcare system appear to be fully supportive of the behavioral approach. In this attitude, health promotion considerations must be fully identified, because it holds individuals accountable for their health. Concerning the social determinants of health, socioeconomic conditions strongly influence the ability of individuals and communities (30, 36). By ignoring the nature and complexity of decision-making, changing human behavior is challenged and the goals of health promotion, at the individual level may not have much justification (16, 38). Thus, employing HL is only possible by participation in HL planning efforts and participation in day-to-day decision making. In the future, families and communities must enable youth to dynamically participate in their health-related issues and engage in the literacy process (35, 39).
In terms of the interrelatedness of sociocultural and environmental characteristics, the following is emphasized; the children and youth are especially dependent upon their caregivers or parents for accessing social, financial, and material resources (29). Initially, these socio-economic and cultural factors are discussed to act as mediators or antecedents for HL and tend to be ignored at the core of HL. Focusing on HL, as specific abilities and skills, leads to disregarding the condition in which HL occurs, as well as the relevant social action to that (11). Likewise, the main gap is observed between the recognition of the effect of cultural and contextual characteristics for HL and their usage within skill-based conceptualizations, individualism, and operationalization that emphasize specific HL dimensions (22, 29). Thus, more effort is required to shift from a skill- and functional-based HL perspective to an alternative viewpoint of understanding HL.
The second research objective identified the extent to which the current HL models cover the characteristics and needs of children and youth. In included studies in this review, specific attention was contributed to characteristics in the analysis of the children and youth groups’ recognition. Accordingly, the findings highlighted the main points, as follow: while several models and definitions of HL were presented for young people (>10 years or secondary school level), same results are lacking for children aged <10 years (primary school) (20, 22, 40). Moreover, the same is true for transitional stages, including from youth to adulthood, or primary school to secondary school.
Our findings indicated that the emphasis is strongly on caregiver or material’s HL abilities; empowering them to secure their children’s healthcare requirements (14, 20, 41). Children under the age of 10 years have not been at the focus of HL intervention and conceptual study plans. Studies investigated the relationship between the health outcome, HL, and healthcare costs for adults. Furthermore, studies explored the literature to assess such relationships for children and youth (14). Therefore, the social condition has a significant contribution to HL in children by their communities, society, and caregivers. Overall, younger children are more dependent on their parents in terms of social support, economic resources, and parents’ HL (14, 20, 42). However, data about how children and parents’ HL interact and interwoven in the development process are scarce.
Besides, most HL dimensions in children and youth were similar to those considered for adults (14, 43). This poor linkage of life stage factors may result from the fact that their perspectives mainly remain unaddressed. Overlaps to HL dimensions in adults were mainly reported in models that emphasized on a life course viewpoint of HL. Therefore, their applicability and validity for the children and youth populations were questionable. This is the main challenge and gap of data since they have considered it as conceptual foundations for HL educational health interventions for children and youth (14, 35).
Implementing general HL models to the children and youth, i.e., not particularly developed to cover the demands and needs of this target group may hinder the effectiveness of HL development in these groups. Thus, children’s and youth’s HL, due to their life situations and needs, must be conceptualized as a concept in its character and not as the extraction of adult HL”. Therefore, the further empirical and conceptual study is required to detect children’s and youth’s specific characteristics; such measures encourages them to further engage with HL concepts and eventually promote healthy behaviors.
This systematic review concentrated on searching the models and definitions of general HL in children; thus, it excluded domain, disease-specific health literacies, or target groups. Though, focusing on general HL facilitates an extensive recognition of the whole field of HL (17). Extending the review links a life period viewpoint on HL; thus, it could have biased the analysis towards non-target group models and definitions. However, we included all articles based on the agreement that if they claim to provide a life period viewpoint on HL, they comprise young persons and children, as well. Accordingly, they are of relevance for the complete framework of the present HL concept for the children. Likewise, this review implemented the PRISMA method to ensure its validity and correctness, and other limitations must be considered.
5. Conclusion
Addressing the HL concept and its key dimensions in children must be designed based on experimental studies. Moreover, thorough and measurable descriptions and applicable theoretical scopes that meet the characteristics of children must be considered. This review recognized a wide theoretical base for HL in children while pointing to key concepts and dimensions, especially correlated to the data and abilities accepted for the children. Moreover, implementing these HL dimensions is required to examine whether these models and definitions are measurable to explain the specific HL constructs or dimensions for children and youth. Similarly, HL could endow children susceptible to become more involved with their health and receive more up-to-date data for future health-related decision making. The relevance of social support and structures based on HL skills are used in very life positions. Besides, children’s distinctiveness from adults is a critical consideration in understanding HL. We believed that numerous critical reflections influence the current understanding of HL; these data could be useful when considered in future health promotion explorations and interventions. Thus, further efforts are required to address these gaps and challenges based on a multidisciplinary viewpoint.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles are considered in this article. The participants were informed about the purpose of the research and its implementation stages; they were also assured about the confidentiality of their information; moreover, they were free to leave the study whenever they wished, and if desired, the research results would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed to designing, running, and writing all parts of the research.
Conflicts of interest
The authors declared no conflicts of interest.
References
Clarke AM, Kuosmanen T, Barry MM. A systematic review of online youth mental health promotion and prevention interventions. Journal of Youth and Adolescence. 2015; 44(1):90-113. [DOI:10.1007/s10964-014-0165-0] [PMID]
Robinson C, Seaman EL, Montgomery L, Winfrey A. A review of hip hop-based interventions for health literacy, health behaviors, and mental health. Journal of Racial and Ethnic Health Disparities. 2018; 5(3):468-84. [DOI:10.1007/s40615-017-0389-2] [PMID] [PMCID]
Peyman N, Oakley D. Married Iranian women’s knowledge, attitude, and sense of self-efficacy about oral contraceptives: Focus group discussion. Journal of Reproduction & Infertility. 2011; 12(4):281.
Peyman N, Alipour Anbarani M. The effect of training diabetes prevention behaviors on promotion of knowledge, attitude and practice of students for prevention of diabetes in Mashhad city. International Journal of Pediatrics. 2015; 3(2.2):501-7.
Zarcadoolas C, Pleasant A, Greer DS. Understanding health literacy: An expanded model. Health Promotion International. 2005; 20(2):195-203. [DOI:10.1093/heapro/dah609] [PMID]
Tavakoly Sany SB, Peyman N, Behzhad F, Esmaeily H, Taghipoor A, Ferns G. Health providers’ communication skills training affects hypertension outcomes. Medical Teacher. 2018; 40(2):154-63. [DOI:10.1080/0142159X.2017.1395002] [PMID]
Avan A, Tavakoly Sany SB, Ghayour‐Mobarhan M, Rahimi HR, Tajfard M, Ferns G. Serum C‐reactive protein in the prediction of cardiovascular diseases: Overview of the latest clinical studies and public health practice. Journal of Cellular Physiology. 2018; 233(11):8508-25. [DOI:10.1002/jcp.26791] [PMID]
Kharazi SS, Peyman N, Esmaily H. Association between maternal health literacy level with pregnancy care and its outcomes. Iranian Journal of Obstetrics, Gynecology and Infertility. 2016; 19(37):40-50.
Paakkari L, Paakkari O. Health literacy as a learning outcome in schools. Health Education. 2012; 112(2):133-52. [DOI:10.1108/09654281211203411]
Siuki HA, Peyman N, Vahedian-Shahroodi M, Gholian-Aval M, Tehrani H. Health education intervention on HIV/AIDS prevention behaviors among health volunteers in healthcare centers: An applying the theory of planned behavior. Journal of Social Service Research. 2019; 45(4):582-8. [DOI:10.1080/01488376.2018.1481177]
Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health. 2012; 12(1):80. [DOI:10.1186/1471-2458-12-80] [PMID] [PMCID]
Dehghankar L, Panahi R, Kekefallah L, Hosseini N, Hasannia E. The study of health literacy and its related factors among female students at high schools in Qazvin. Journal of Health Literacy. 2019; 4(2):18-26.
Rothman RL, Yin HS, Mulvaney S, Homer C, Lannon C. Health literacy and quality: Focus on chronic illness care and patient safety. Pediatrics. 2009; 124(Suppl 3):S315-S26. [DOI:10.1542/peds.2009-1163H] [PMID]
Borzekowski D. Considering children and health literacy: A theoretical approach. Pediatrics. 2009; 124:S282-8. [DOI:10.1542/peds.2009-1162D] [PMID]
Fok MS, Wong TK. What does health literacy mean to children? Contemporary Nurse. 2002; 13(2-3):249-58. [DOI:10.5172/conu.13.2-3.249] [PMID]
Wolf MS, Wilson EA, Rapp DN, Waite KR, Bocchini MV, Davis TC, et al. Literacy and learning in health care. Pediatrics. 2009; 124(Suppl 3):S275-S81. [DOI:10.1542/peds.2009-1162C] [PMID] [PMCID]
Wu AD, Begoray DL, MacDonald M, Wharf Higgins J, Frankish J, Kwan B, et al. Developing and evaluating a relevant and feasible instrument for measuring health literacy of Canadian high school students. Health Promotion International. 2010; 25(4):444-52. [DOI:10.1093/heapro/daq032] [PMID]
Gordon SC, Barry CD, Dunn DJ, King B. Clarifying a vision for health literacy: A holistic school-based community approach. Holistic Nursing Practice. 2011; 25(3):120-6. [DOI:10.1097/HNP.0b013e3182157c34] [PMID]
Massey PM, Prelip M, Calimlim BM, Quiter ES, Glik DC. Contextualizing an expanded definition of health literacy among adolescents in the health care setting. Health Education Research. 2012; 27(6):961-74. [DOI:10.1093/her/cys054] [PMID] [PMCID]
Brown SL, Teufel JA, Birch DA. Early adolescents perceptions of health and health literacy. Journal of School Health. 2007; 77(1):7-15. [DOI:10.1111/j.1746-1561.2007.00156.x] [PMID]
Paek H-J, Reber BH, Lariscy RW. Roles of interpersonal and media socialization agents in adolescent self-reported health literacy: A health socialization perspective. Health Education Research. 2011; 26(1):131-49. [DOI:10.1093/her/cyq082] [PMID]
Schmidt CO, Fahland RA, Franze M, Splieth C, Thyrian JR, Plachta-Danielzik S, et al. Health-related behaviour, knowledge, attitudes, communication and social status in school children in Eastern Germany. Health Education Research. 2010; 25(4):542-51. [DOI:10.1093/her/cyq011] [PMID]
Sanders LM, Federico S, Klass P, Abrams MA, Dreyer B. Literacy and child health: A systematic review. Archives of Pediatrics & Adolescent Medicine. 2009; 163(2):131-40. [DOI:10.1001/archpediatrics.2008.539] [PMID]
Subramaniam M, Jean BS, Taylor NG, Kodama C, Follman R, Casciotti D. Bit by bit: Using design-based research to improve the health literacy of adolescents. JMIR Research Protocols. 2015; 4(2):e62.
Zeyer A, Odermatt F. [Gesundheitskompetenz (Health Literacy)-Bindeglied zwischen Gesundheitsbildung und naturwissenschaftlichem Unterricht (German)] (Health Literacy – a Link between Health Education and Science Education). Zeitschrift für Didaktik der Naturwissenschaften. 2009; 15:265-85. [DOI:10.5167/uzh-31004]
Sanders LM, Shaw JS, Guez G, Baur C, Rudd R. Health literacy and child health promotion: Implications for research, clinical care, and public policy. Pediatrics. 2009; 124(Suppl 3):S306-S14. [DOI:10.1542/peds.2009-1162G] [PMID]
Funnell MM, Brown TL, Childs BP, Haas LB, Hosey GM, Jensen B, et al. National standards for diabetes self-management education. Diabetes Care. 2008; 31(Suppl 1):S97-S104. [DOI:10.2337/dc08-S097] [PMID]
Rask M, Uusiautti S, Määttä K. The fourth level of health literacy. International Quarterly of Ccommunity Health Education. 2014; 34(1):51-71. [DOI:10.2190/IQ.34.1.e] [PMID]
von Eckhard Klieme H, Leutner D, Kenk M. [Kompetenzmodellierung Zwischenbilanz des DFG-Schwerpunktprogramms und Perspektiven des Forschungsansatzes. In: Soellner R, Huber S, Lenartz N, Rudinger G, editors. Facetten der Gesundheitskompetenz-eine Expertenbefragung (German)]. Projekt Gesundheitskompetenz. Frankfurt: Pedocs; 2010. https://www.pedocs.de/volltexte/2010/3384/pdf/Soellner_Huber_Lenartz_Rudinger_Projekt_Gesundheitskompetenz_D_A.pdf
Martin LT, Chen P. Child health and school readiness: The significance of health literacy. In: Health and Education in Early Childhood: Predictors, Interventions, and Policies. Reynolds JA, Rolnick JA, Temple JA (Eds). Cambridge: Cambridge University Press; 2014. [DOI:10.1017/CBO9781139814805.018] [PMCID]
Manganello JA. Health literacy and adolescents: A framework and agenda for future research. Health Education Research. 2007; 23(5):840-7. [DOI:10.1093/her/cym069] [PMID]
Higgins JW, Begoray D, MacDonald M. A social ecological conceptual framework for understanding adolescent health literacy in the health education classroom. American Journal of Community Psychology. 2009; 44(3-4):350. [DOI:10.1007/s10464-009-9270-8] [PMID]
Jafari Y, Vahedian-Shahroodi M, Tehrani H, Haresabadi M, Shariati M. The relationship between caregivers’ health literacy and the behavior of women with multiple sclerosis. Iranian Journal of Obstetrics, Gynecology and Infertility. 2018; 21(7):71-64.
Pirzadeh A, Nodooshan T, Nasirian M. Association between maternal health literacy level and prenatal care in Iran. Journal of Health Literacy. 2019; 4(1):60-7.
Bröder J, Okan O, Bauer U, Bruland D, Schlupp S, Bollweg TM, et al. Health literacy in childhood and youth: A systematic review of definitions and models. BMC Public Health. 2017; 17(1):361. [DOI:10.1186/s12889-017-4365-x] [PMID] [PMCID]
Mackert M, Champlin S, Su Z, Guadagno M. The many health literacies: Advancing research or fragmentation? Health Communication. 2015; 30(12):1161-5. [DOI:10.1080/10410236.2015.1037422] [PMID]
Mahdizadeh F, Tatari M, Sheykhotayefeh M. Study of health literacy and its related factors in Torbat Heydarieh students of medical sciences in 2019. Journal of Health Literacy. 2019; 4(2):44-8.
Olyani S, Tehrani H, Esmaily H, Rezaii MM, Vahedian-shahroodi M. Assessment of health literacy with the newest vital sign and its correlation with Body Mass Index in female adolescent students. International Journal of Adolescent Medicine and Health. 2017; 32(2):/j/ijamh.2020.32.issue-2/ijamh-2017-0103/ijamh-2017-0103.xml. [DOI:10.1515/ijamh-2017-0103] [PMID]
Nejatian M, Alami A, Tehrani H, Lael-Monfared E, Jafari A. Perceptions and personal use of Complementary and Alternative Medicine (CAM) by Iranian health care providers. Complementary Therapies in Clinical Practice. 2018; 32:145-50. [DOI:10.1016/j.ctcp.2018.06.002] [PMID]
Lael-Monfared E, Tehrani H, Moghaddam ZE, Ferns GA, Tatari M, Jafari A. Health literacy, knowledge and self-care behaviors to take care of diabetic foot in low-income individuals: Application of extended parallel process model. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. 2019; 13(2):1535-41. [DOI:10.1016/j.dsx.2019.03.008] [PMID]
Hejazi S, Peyman N, Esmaily H. Effect of educational intervention based on self-efficacy on preventive behaviors of overweight and obesity among secondary-school female students in Mashhad. Iranian Journal of Endocrinology and Metabolism. 2017; 19(4):261-9.
Charoghchian Khorasani E, Peyman N, Esmaily H. Relations between breastfeeding self-efficacy and maternal health literacy among pregnant women. Evidence Based Care. 2017; 6(4):18-25.
Mazloomy Mahmoodabad SS, Tehrani H, Gholian-aval M, Gholami H, Nematy M. The effect of social class on the amount of salt intake in patients with hypertension. Blood Pressure. 2016; 25(6):360-3. [DOI:10.1080/08037051.2016.1179508] [PMID]
The factors affecting the HL of children and youth or the outcomes, i.e., influenced by HL are listed in Table 4. In the 9 identified models, differentiation has been made between individual characteristics, demographic factors, situation or context, and the broader system (the social factors) (5, 21, 22). These studies highlighted the effect of parental influences and family’s demographic factors. Younger children are more prone to trusting their parents concerning socioeconomic support. In these conditions, the individual’s socioeconomic status or occupation plays no role in these variables (18, 26, 30). Family demographic factors include socioeconomic status, health status, and parental HL.
Martin and Chen (30) reported that these family characteristics significantly impact health status, HL, and educational variables in children. These characteristics include their willingness on going to school and the educational outcomes. In addition, families, schools, and peers are the main socialization factors in children’s lives; they affect their potential for being health literate. Peers and family can encourage or discourage HL practices and health-promotion behaviors through their social supports, norms, and practices (11, 32, 33). Parents and peers could be a role model for achieving and interpreting HL by teaching their children to assess the credibility of the sources from which they obtain information. In this context, the type and quality of communication significantly affect children. This is because children mainly consult with their trusted peers and family. Access to online media and resources also influences their health status. The social level also refers to health, education, social systems, as well as cultural and political forces. This includes the general conditions and learning environment of the individual. Such factors may include the safety of students at school, and the teacher’s skills that could promote reflexing and critical thinking in students (9, 32).
Ten articles suggested that HL in children leads to individual and social benefits (Table 4). At the individual level, HL enables the young population to be skilled users of the healthcare system and to overcome the related interpersonal and environmental problems (14, 17, 27). Moreover, HL allows children to better perceive themselves, others, and the world, discuss health-related social issues and make proper health decisions (9, 21, 28). It is also believed that young people with adequate HL could start and accomplish their health objectives, including participating in physical activity or avoid alcohol consumption (25). Furthermore, HL benefits cover a wide range of living performances, at home, work, community, and even economic levels (5, 11). In terms of communicational and societal benefits, HL could promote participation in community health programs to increase the general capacity and community empowerment; it could eventually impact one’s health, the health of others, and the social norms (9, 16, 34).
4. Discussion
In this review article, we identified 8 definitions and 9 models regarding the HL status for children and young individuals. As a high heterogeneous definition and complex model, HL is a complex concept with multidimensional constructs or dimensions. Furthermore, by explaining these constructs along with multiple integrated classifications, presenting a combination of the HL constructs recovered from the literature seems reasonable (35, 36). However, these definitions may overlap due to different reasons, resulting in differential focuses. These findings are consistent with those of Paakkari and colleagues (4); they highlighted that “there are differences in the components of HL and its associated characteristics” (9, 37). Concerning the first research question, in most definitions and models, the focus of HL is beyond the set of healthcare settings. It seems that HL in children is related to multiple contexts and occasions of daily life that influence the promotion of one’s health and well-being.
HL in children, like adults (11), involves agency and actions which alter according to the HL viewpoint; e.g., from healthcare or clinical setting models to a more general public health or health system and health promotion model (24, 28, 35). As a result, HL is content- and context-specific and concordant with the present contextual factors and the complexity of the task (20). The contextual factors’ influence was supported in the literature; however, they often remained underscored. It was evidenced that the individual characteristics include the skills and knowledge that an individual requires to encounter certain situational requirements. These necessities include the general health center-related situational requirements that communities pose upon an individual (35). Furthermore, the behavioral components of HL are usually not distinguished from the HL outcome (Table 4). Some strong skills and individual-based HL concepts are required for individuals to be actively involved in understanding, seeking, making health-related decisions. Moreover, such skills also facilitate accessing information that reflects children’s everyday lives.
HL models especially focus on the healthcare system; they seem to significantly and primarily view individuals. They adhere to a perspective complying with the professional health instructions and receive the provided health information. Models that target the healthcare system appear to be fully supportive of the behavioral approach. In this attitude, health promotion considerations must be fully identified, because it holds individuals accountable for their health. Concerning the social determinants of health, socioeconomic conditions strongly influence the ability of individuals and communities (30, 36). By ignoring the nature and complexity of decision-making, changing human behavior is challenged and the goals of health promotion, at the individual level may not have much justification (16, 38). Thus, employing HL is only possible by participation in HL planning efforts and participation in day-to-day decision making. In the future, families and communities must enable youth to dynamically participate in their health-related issues and engage in the literacy process (35, 39).
In terms of the interrelatedness of sociocultural and environmental characteristics, the following is emphasized; the children and youth are especially dependent upon their caregivers or parents for accessing social, financial, and material resources (29). Initially, these socio-economic and cultural factors are discussed to act as mediators or antecedents for HL and tend to be ignored at the core of HL. Focusing on HL, as specific abilities and skills, leads to disregarding the condition in which HL occurs, as well as the relevant social action to that (11). Likewise, the main gap is observed between the recognition of the effect of cultural and contextual characteristics for HL and their usage within skill-based conceptualizations, individualism, and operationalization that emphasize specific HL dimensions (22, 29). Thus, more effort is required to shift from a skill- and functional-based HL perspective to an alternative viewpoint of understanding HL.
The second research objective identified the extent to which the current HL models cover the characteristics and needs of children and youth. In included studies in this review, specific attention was contributed to characteristics in the analysis of the children and youth groups’ recognition. Accordingly, the findings highlighted the main points, as follow: while several models and definitions of HL were presented for young people (>10 years or secondary school level), same results are lacking for children aged <10 years (primary school) (20, 22, 40). Moreover, the same is true for transitional stages, including from youth to adulthood, or primary school to secondary school.
Our findings indicated that the emphasis is strongly on caregiver or material’s HL abilities; empowering them to secure their children’s healthcare requirements (14, 20, 41). Children under the age of 10 years have not been at the focus of HL intervention and conceptual study plans. Studies investigated the relationship between the health outcome, HL, and healthcare costs for adults. Furthermore, studies explored the literature to assess such relationships for children and youth (14). Therefore, the social condition has a significant contribution to HL in children by their communities, society, and caregivers. Overall, younger children are more dependent on their parents in terms of social support, economic resources, and parents’ HL (14, 20, 42). However, data about how children and parents’ HL interact and interwoven in the development process are scarce.
Besides, most HL dimensions in children and youth were similar to those considered for adults (14, 43). This poor linkage of life stage factors may result from the fact that their perspectives mainly remain unaddressed. Overlaps to HL dimensions in adults were mainly reported in models that emphasized on a life course viewpoint of HL. Therefore, their applicability and validity for the children and youth populations were questionable. This is the main challenge and gap of data since they have considered it as conceptual foundations for HL educational health interventions for children and youth (14, 35).
Implementing general HL models to the children and youth, i.e., not particularly developed to cover the demands and needs of this target group may hinder the effectiveness of HL development in these groups. Thus, children’s and youth’s HL, due to their life situations and needs, must be conceptualized as a concept in its character and not as the extraction of adult HL”. Therefore, the further empirical and conceptual study is required to detect children’s and youth’s specific characteristics; such measures encourages them to further engage with HL concepts and eventually promote healthy behaviors.
This systematic review concentrated on searching the models and definitions of general HL in children; thus, it excluded domain, disease-specific health literacies, or target groups. Though, focusing on general HL facilitates an extensive recognition of the whole field of HL (17). Extending the review links a life period viewpoint on HL; thus, it could have biased the analysis towards non-target group models and definitions. However, we included all articles based on the agreement that if they claim to provide a life period viewpoint on HL, they comprise young persons and children, as well. Accordingly, they are of relevance for the complete framework of the present HL concept for the children. Likewise, this review implemented the PRISMA method to ensure its validity and correctness, and other limitations must be considered.
5. Conclusion
Addressing the HL concept and its key dimensions in children must be designed based on experimental studies. Moreover, thorough and measurable descriptions and applicable theoretical scopes that meet the characteristics of children must be considered. This review recognized a wide theoretical base for HL in children while pointing to key concepts and dimensions, especially correlated to the data and abilities accepted for the children. Moreover, implementing these HL dimensions is required to examine whether these models and definitions are measurable to explain the specific HL constructs or dimensions for children and youth. Similarly, HL could endow children susceptible to become more involved with their health and receive more up-to-date data for future health-related decision making. The relevance of social support and structures based on HL skills are used in very life positions. Besides, children’s distinctiveness from adults is a critical consideration in understanding HL. We believed that numerous critical reflections influence the current understanding of HL; these data could be useful when considered in future health promotion explorations and interventions. Thus, further efforts are required to address these gaps and challenges based on a multidisciplinary viewpoint.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles are considered in this article. The participants were informed about the purpose of the research and its implementation stages; they were also assured about the confidentiality of their information; moreover, they were free to leave the study whenever they wished, and if desired, the research results would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed to designing, running, and writing all parts of the research.
Conflicts of interest
The authors declared no conflicts of interest.
References
Clarke AM, Kuosmanen T, Barry MM. A systematic review of online youth mental health promotion and prevention interventions. Journal of Youth and Adolescence. 2015; 44(1):90-113. [DOI:10.1007/s10964-014-0165-0] [PMID]
Robinson C, Seaman EL, Montgomery L, Winfrey A. A review of hip hop-based interventions for health literacy, health behaviors, and mental health. Journal of Racial and Ethnic Health Disparities. 2018; 5(3):468-84. [DOI:10.1007/s40615-017-0389-2] [PMID] [PMCID]
Peyman N, Oakley D. Married Iranian women’s knowledge, attitude, and sense of self-efficacy about oral contraceptives: Focus group discussion. Journal of Reproduction & Infertility. 2011; 12(4):281.
Peyman N, Alipour Anbarani M. The effect of training diabetes prevention behaviors on promotion of knowledge, attitude and practice of students for prevention of diabetes in Mashhad city. International Journal of Pediatrics. 2015; 3(2.2):501-7.
Zarcadoolas C, Pleasant A, Greer DS. Understanding health literacy: An expanded model. Health Promotion International. 2005; 20(2):195-203. [DOI:10.1093/heapro/dah609] [PMID]
Tavakoly Sany SB, Peyman N, Behzhad F, Esmaeily H, Taghipoor A, Ferns G. Health providers’ communication skills training affects hypertension outcomes. Medical Teacher. 2018; 40(2):154-63. [DOI:10.1080/0142159X.2017.1395002] [PMID]
Avan A, Tavakoly Sany SB, Ghayour‐Mobarhan M, Rahimi HR, Tajfard M, Ferns G. Serum C‐reactive protein in the prediction of cardiovascular diseases: Overview of the latest clinical studies and public health practice. Journal of Cellular Physiology. 2018; 233(11):8508-25. [DOI:10.1002/jcp.26791] [PMID]
Kharazi SS, Peyman N, Esmaily H. Association between maternal health literacy level with pregnancy care and its outcomes. Iranian Journal of Obstetrics, Gynecology and Infertility. 2016; 19(37):40-50.
Paakkari L, Paakkari O. Health literacy as a learning outcome in schools. Health Education. 2012; 112(2):133-52. [DOI:10.1108/09654281211203411]
Siuki HA, Peyman N, Vahedian-Shahroodi M, Gholian-Aval M, Tehrani H. Health education intervention on HIV/AIDS prevention behaviors among health volunteers in healthcare centers: An applying the theory of planned behavior. Journal of Social Service Research. 2019; 45(4):582-8. [DOI:10.1080/01488376.2018.1481177]
Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health. 2012; 12(1):80. [DOI:10.1186/1471-2458-12-80] [PMID] [PMCID]
Dehghankar L, Panahi R, Kekefallah L, Hosseini N, Hasannia E. The study of health literacy and its related factors among female students at high schools in Qazvin. Journal of Health Literacy. 2019; 4(2):18-26.
Rothman RL, Yin HS, Mulvaney S, Homer C, Lannon C. Health literacy and quality: Focus on chronic illness care and patient safety. Pediatrics. 2009; 124(Suppl 3):S315-S26. [DOI:10.1542/peds.2009-1163H] [PMID]
Borzekowski D. Considering children and health literacy: A theoretical approach. Pediatrics. 2009; 124:S282-8. [DOI:10.1542/peds.2009-1162D] [PMID]
Fok MS, Wong TK. What does health literacy mean to children? Contemporary Nurse. 2002; 13(2-3):249-58. [DOI:10.5172/conu.13.2-3.249] [PMID]
Wolf MS, Wilson EA, Rapp DN, Waite KR, Bocchini MV, Davis TC, et al. Literacy and learning in health care. Pediatrics. 2009; 124(Suppl 3):S275-S81. [DOI:10.1542/peds.2009-1162C] [PMID] [PMCID]
Wu AD, Begoray DL, MacDonald M, Wharf Higgins J, Frankish J, Kwan B, et al. Developing and evaluating a relevant and feasible instrument for measuring health literacy of Canadian high school students. Health Promotion International. 2010; 25(4):444-52. [DOI:10.1093/heapro/daq032] [PMID]
Gordon SC, Barry CD, Dunn DJ, King B. Clarifying a vision for health literacy: A holistic school-based community approach. Holistic Nursing Practice. 2011; 25(3):120-6. [DOI:10.1097/HNP.0b013e3182157c34] [PMID]
Massey PM, Prelip M, Calimlim BM, Quiter ES, Glik DC. Contextualizing an expanded definition of health literacy among adolescents in the health care setting. Health Education Research. 2012; 27(6):961-74. [DOI:10.1093/her/cys054] [PMID] [PMCID]
Brown SL, Teufel JA, Birch DA. Early adolescents perceptions of health and health literacy. Journal of School Health. 2007; 77(1):7-15. [DOI:10.1111/j.1746-1561.2007.00156.x] [PMID]
Paek H-J, Reber BH, Lariscy RW. Roles of interpersonal and media socialization agents in adolescent self-reported health literacy: A health socialization perspective. Health Education Research. 2011; 26(1):131-49. [DOI:10.1093/her/cyq082] [PMID]
Schmidt CO, Fahland RA, Franze M, Splieth C, Thyrian JR, Plachta-Danielzik S, et al. Health-related behaviour, knowledge, attitudes, communication and social status in school children in Eastern Germany. Health Education Research. 2010; 25(4):542-51. [DOI:10.1093/her/cyq011] [PMID]
Sanders LM, Federico S, Klass P, Abrams MA, Dreyer B. Literacy and child health: A systematic review. Archives of Pediatrics & Adolescent Medicine. 2009; 163(2):131-40. [DOI:10.1001/archpediatrics.2008.539] [PMID]
Subramaniam M, Jean BS, Taylor NG, Kodama C, Follman R, Casciotti D. Bit by bit: Using design-based research to improve the health literacy of adolescents. JMIR Research Protocols. 2015; 4(2):e62.
Zeyer A, Odermatt F. [Gesundheitskompetenz (Health Literacy)-Bindeglied zwischen Gesundheitsbildung und naturwissenschaftlichem Unterricht (German)] (Health Literacy – a Link between Health Education and Science Education). Zeitschrift für Didaktik der Naturwissenschaften. 2009; 15:265-85. [DOI:10.5167/uzh-31004]
Sanders LM, Shaw JS, Guez G, Baur C, Rudd R. Health literacy and child health promotion: Implications for research, clinical care, and public policy. Pediatrics. 2009; 124(Suppl 3):S306-S14. [DOI:10.1542/peds.2009-1162G] [PMID]
Funnell MM, Brown TL, Childs BP, Haas LB, Hosey GM, Jensen B, et al. National standards for diabetes self-management education. Diabetes Care. 2008; 31(Suppl 1):S97-S104. [DOI:10.2337/dc08-S097] [PMID]
Rask M, Uusiautti S, Määttä K. The fourth level of health literacy. International Quarterly of Ccommunity Health Education. 2014; 34(1):51-71. [DOI:10.2190/IQ.34.1.e] [PMID]
von Eckhard Klieme H, Leutner D, Kenk M. [Kompetenzmodellierung Zwischenbilanz des DFG-Schwerpunktprogramms und Perspektiven des Forschungsansatzes. In: Soellner R, Huber S, Lenartz N, Rudinger G, editors. Facetten der Gesundheitskompetenz-eine Expertenbefragung (German)]. Projekt Gesundheitskompetenz. Frankfurt: Pedocs; 2010. https://www.pedocs.de/volltexte/2010/3384/pdf/Soellner_Huber_Lenartz_Rudinger_Projekt_Gesundheitskompetenz_D_A.pdf
Martin LT, Chen P. Child health and school readiness: The significance of health literacy. In: Health and Education in Early Childhood: Predictors, Interventions, and Policies. Reynolds JA, Rolnick JA, Temple JA (Eds). Cambridge: Cambridge University Press; 2014. [DOI:10.1017/CBO9781139814805.018] [PMCID]
Manganello JA. Health literacy and adolescents: A framework and agenda for future research. Health Education Research. 2007; 23(5):840-7. [DOI:10.1093/her/cym069] [PMID]
Higgins JW, Begoray D, MacDonald M. A social ecological conceptual framework for understanding adolescent health literacy in the health education classroom. American Journal of Community Psychology. 2009; 44(3-4):350. [DOI:10.1007/s10464-009-9270-8] [PMID]
Jafari Y, Vahedian-Shahroodi M, Tehrani H, Haresabadi M, Shariati M. The relationship between caregivers’ health literacy and the behavior of women with multiple sclerosis. Iranian Journal of Obstetrics, Gynecology and Infertility. 2018; 21(7):71-64.
Pirzadeh A, Nodooshan T, Nasirian M. Association between maternal health literacy level and prenatal care in Iran. Journal of Health Literacy. 2019; 4(1):60-7.
Bröder J, Okan O, Bauer U, Bruland D, Schlupp S, Bollweg TM, et al. Health literacy in childhood and youth: A systematic review of definitions and models. BMC Public Health. 2017; 17(1):361. [DOI:10.1186/s12889-017-4365-x] [PMID] [PMCID]
Mackert M, Champlin S, Su Z, Guadagno M. The many health literacies: Advancing research or fragmentation? Health Communication. 2015; 30(12):1161-5. [DOI:10.1080/10410236.2015.1037422] [PMID]
Mahdizadeh F, Tatari M, Sheykhotayefeh M. Study of health literacy and its related factors in Torbat Heydarieh students of medical sciences in 2019. Journal of Health Literacy. 2019; 4(2):44-8.
Olyani S, Tehrani H, Esmaily H, Rezaii MM, Vahedian-shahroodi M. Assessment of health literacy with the newest vital sign and its correlation with Body Mass Index in female adolescent students. International Journal of Adolescent Medicine and Health. 2017; 32(2):/j/ijamh.2020.32.issue-2/ijamh-2017-0103/ijamh-2017-0103.xml. [DOI:10.1515/ijamh-2017-0103] [PMID]
Nejatian M, Alami A, Tehrani H, Lael-Monfared E, Jafari A. Perceptions and personal use of Complementary and Alternative Medicine (CAM) by Iranian health care providers. Complementary Therapies in Clinical Practice. 2018; 32:145-50. [DOI:10.1016/j.ctcp.2018.06.002] [PMID]
Lael-Monfared E, Tehrani H, Moghaddam ZE, Ferns GA, Tatari M, Jafari A. Health literacy, knowledge and self-care behaviors to take care of diabetic foot in low-income individuals: Application of extended parallel process model. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. 2019; 13(2):1535-41. [DOI:10.1016/j.dsx.2019.03.008] [PMID]
Hejazi S, Peyman N, Esmaily H. Effect of educational intervention based on self-efficacy on preventive behaviors of overweight and obesity among secondary-school female students in Mashhad. Iranian Journal of Endocrinology and Metabolism. 2017; 19(4):261-9.
Charoghchian Khorasani E, Peyman N, Esmaily H. Relations between breastfeeding self-efficacy and maternal health literacy among pregnant women. Evidence Based Care. 2017; 6(4):18-25.
Mazloomy Mahmoodabad SS, Tehrani H, Gholian-aval M, Gholami H, Nematy M. The effect of social class on the amount of salt intake in patients with hypertension. Blood Pressure. 2016; 25(6):360-3. [DOI:10.1080/08037051.2016.1179508] [PMID]
Type of Study: Systematic Review |
Subject:
Pediatric Psychology
Received: 2019/09/17 | Accepted: 2019/11/10 | Published: 2020/07/1
Received: 2019/09/17 | Accepted: 2019/11/10 | Published: 2020/07/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
