
Mon, Jul 13, 2026


Volume 14, Issue 2 (April 2026)
J. Pediatr. Rev 2026, 14(2): 145-154 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Emadi Majd F, Langari S F, Langari S H. Artificial Intelligence in Pediatric Lateral Cephalometric Detection and Analysis: A Narrative Review. J. Pediatr. Rev 2026; 14 (2) :145-154
URL: http://jpr.mazums.ac.ir/article-1-819-en.html
URL: http://jpr.mazums.ac.ir/article-1-819-en.html



1- Department of Orthodontics, TD.C., Islamic Azad University, Tehran, Iran.
2- Department of Restorative Dentistry, School of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Radiology, Taleghani Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,seyyedhasanlangari@gmail.com
2- Department of Restorative Dentistry, School of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Department of Radiology, Taleghani Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,
Keywords: Artificial intelligence (AI), Pediatric cephalometry, Cephalometric landmark detection, Deep learning, Diagnostic automation, Orthodontics, Explainable artificial intelligence (XAI)
Full-Text [PDF 1989 kb]
(120 Downloads)
| Abstract (HTML) (248 Views)
Full-Text: (46 Views)
Introduction
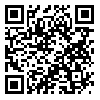
Cephalometric analysis remains a cornerstone in orthodontic diagnosis and treatment planning, particularly in pediatric populations where growth dynamics significantly influence craniofacial development [1]. Since Broadbent and Hofrath’s pioneering work in the 1930s, manual landmark identification on lateral cephalograms has been the clinical standard. However, this approach suffers from inherent limitations, including intra- and inter-examiner variability, time consumption, and susceptibility to human error—challenges amplified in pediatric cases due to superimposed anatomical structures and ongoing skeletal maturation [2, 3]. An example of the conventional manual cephalometric tracing technique is shown in Figure 1.
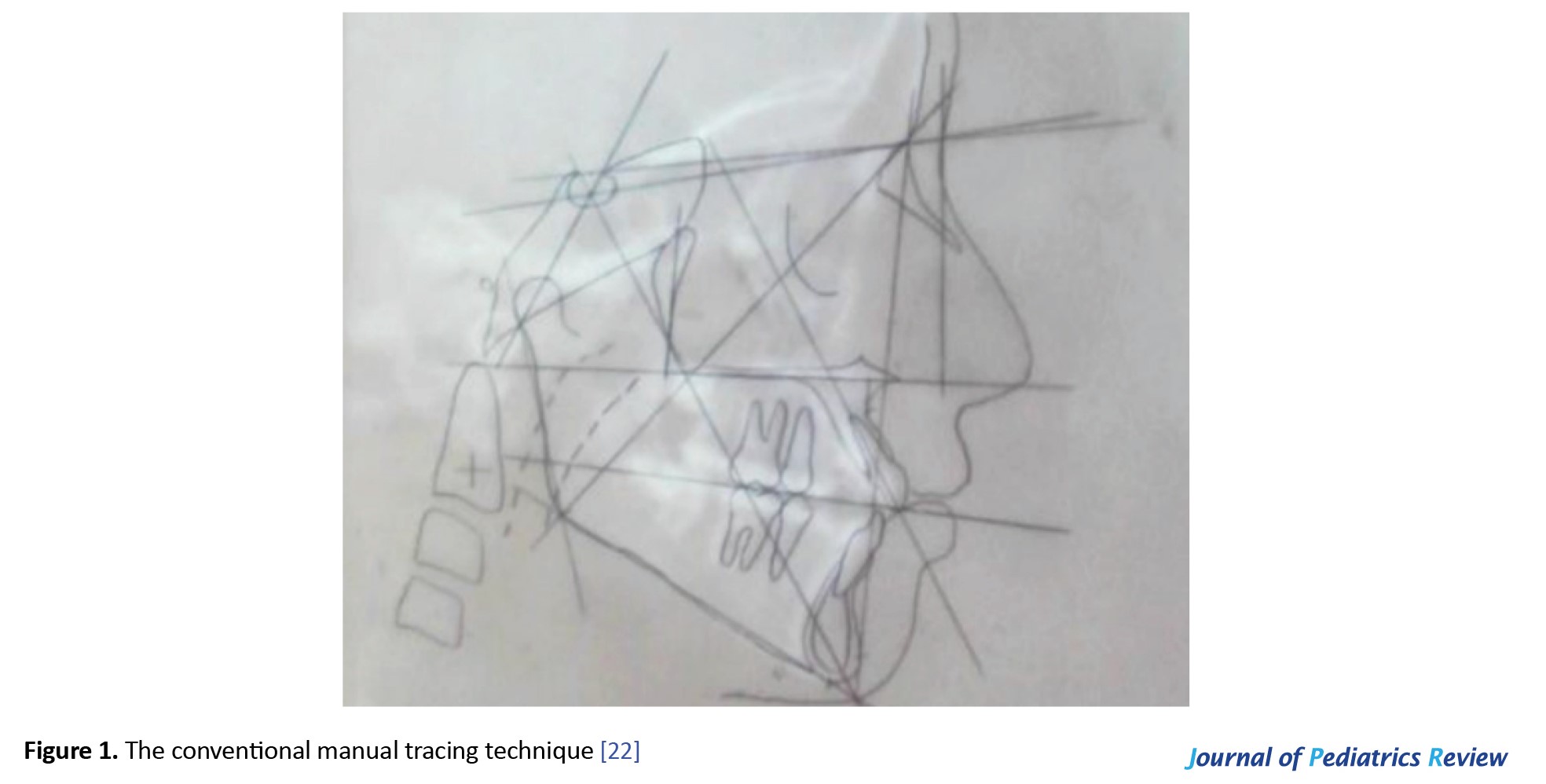 The emergence of artificial intelligence (AI), particularly deep learning algorithms, offers transformative potential for automating cephalometric landmark detection. Convolutional neural networks (CNNs) have demonstrated remarkable accuracy in identifying anatomical landmarks, with recent studies reporting MRE below 1.0 mm—approaching or exceeding human expert performance [2, 4]. These advancements promise not only enhanced precision but also substantial time savings, enabling clinicians to focus on treatment strategy rather than labor-intensive tracing procedures. An example of digital landmark identification using Dolphin Imaging software is presented in Figure 2.
The emergence of artificial intelligence (AI), particularly deep learning algorithms, offers transformative potential for automating cephalometric landmark detection. Convolutional neural networks (CNNs) have demonstrated remarkable accuracy in identifying anatomical landmarks, with recent studies reporting MRE below 1.0 mm—approaching or exceeding human expert performance [2, 4]. These advancements promise not only enhanced precision but also substantial time savings, enabling clinicians to focus on treatment strategy rather than labor-intensive tracing procedures. An example of digital landmark identification using Dolphin Imaging software is presented in Figure 2.
 Pediatric cephalometry presents unique challenges that demand specialized AI solutions: smaller anatomical structures, variable tooth eruption stages, and rapid growth-related morphological changes necessitate age-specific algorithms [4]. While initial AI applications focused on adult populations, recent research has begun addressing pediatric-specific requirements through age-stratified training datasets and growth-stage-aware architectures [5].
Pediatric cephalometry presents unique challenges that demand specialized AI solutions: smaller anatomical structures, variable tooth eruption stages, and rapid growth-related morphological changes necessitate age-specific algorithms [4]. While initial AI applications focused on adult populations, recent research has begun addressing pediatric-specific requirements through age-stratified training datasets and growth-stage-aware architectures [5].
This narrative review synthesizes current evidence on AI applications in pediatric cephalometric analysis, critically evaluates the methodological strengths and limitations of existing approaches, and proposes a framework for the clinical translation of these technologies in pediatric orthodontic practice.
Materials and Methods
This narrative review synthesizes peer-reviewed literature published between January 2020 and October 2025 that evaluates AI-driven cephalometric systems in pediatric populations. This study aimed to assess diagnostic performance, clinical feasibility, educational utility, and emerging innovations in low-radiation or non-ionizing diagnostic approaches.
Search strategy and inclusion criteria
A systematic search was conducted across major biomedical databases, including PubMed, Scopus, and Google Scholar. Keywords and MeSH terms included combinations of AI, deep learning, convolutional neural network, cephalometric analysis, landmark detection, pediatric orthodontics, automated diagnosis, and radiation reduction. Only English-language, peer-reviewed original research articles, validation studies, and comparative analyses were included.
Studies were eligible if they:
Evaluated AI systems for lateral cephalometric landmark detection or analysis;
Reported quantitative metrics of accuracy (e.g. mean radial error, success detection rate), reproducibility, or time efficiency;
Compared manual, semi-automated, or fully automated methodologies;
Addressed clinical integration, educational applications, or novel imaging modalities (e.g. facial photographs, low-dose cone beam computed tomography [CBCT]).
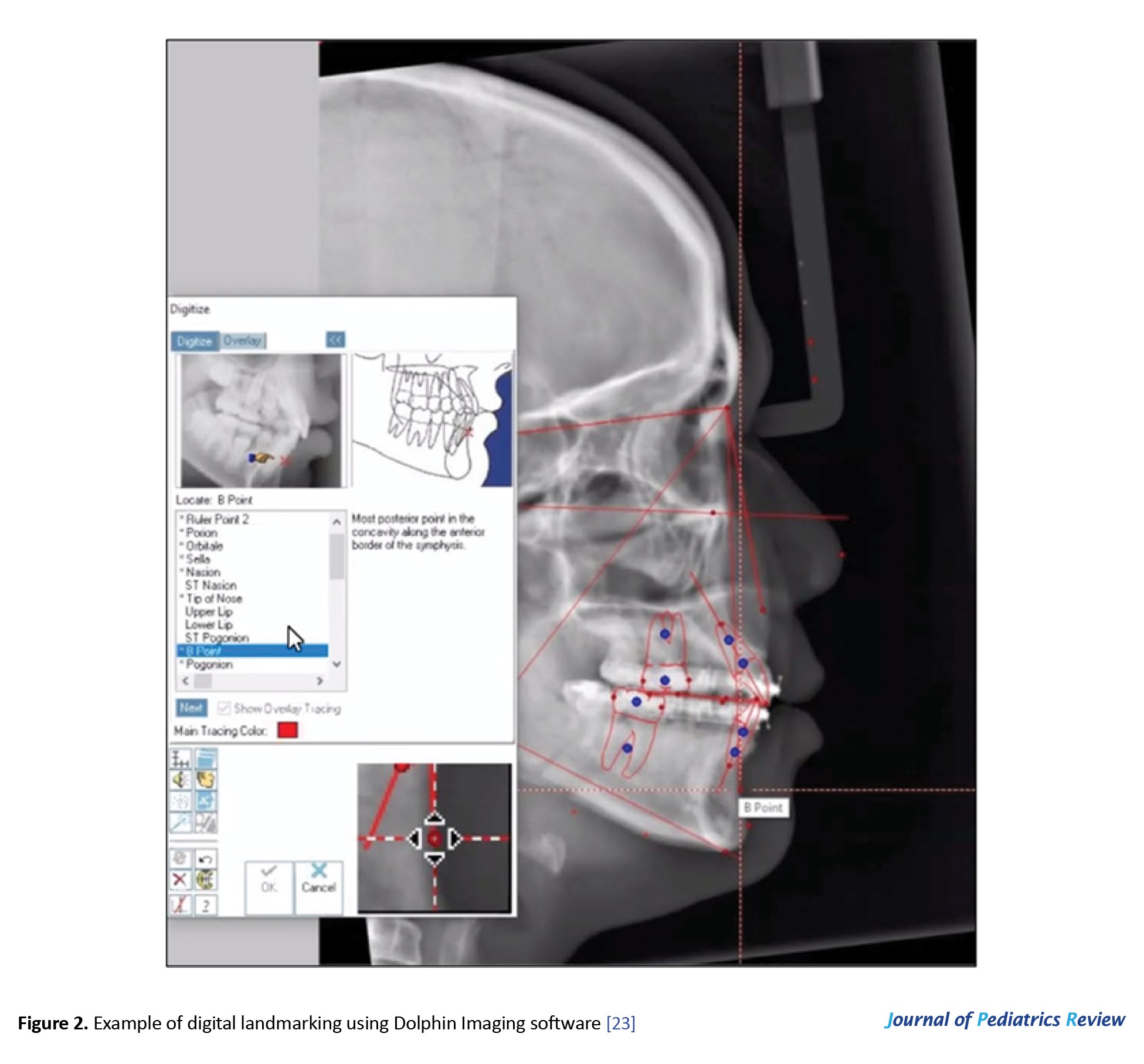
The selection process followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. Initial database searches yielded 69 records. Of these, 21 records were excluded based on predefined criteria (irrelevant population, non-AI methodology, or non-cephalometric focus). Following detailed evaluation, 24 additional articles were excluded for the following reasons: absence of quantitative accuracy metrics, publication before 2020, and insufficient methodological detail for AI system evaluation. The final synthesis included 24 studies meeting all inclusion criteria. The study selection process is summarized in Figure 3.
Results
Diagnostic accuracy and technical performance
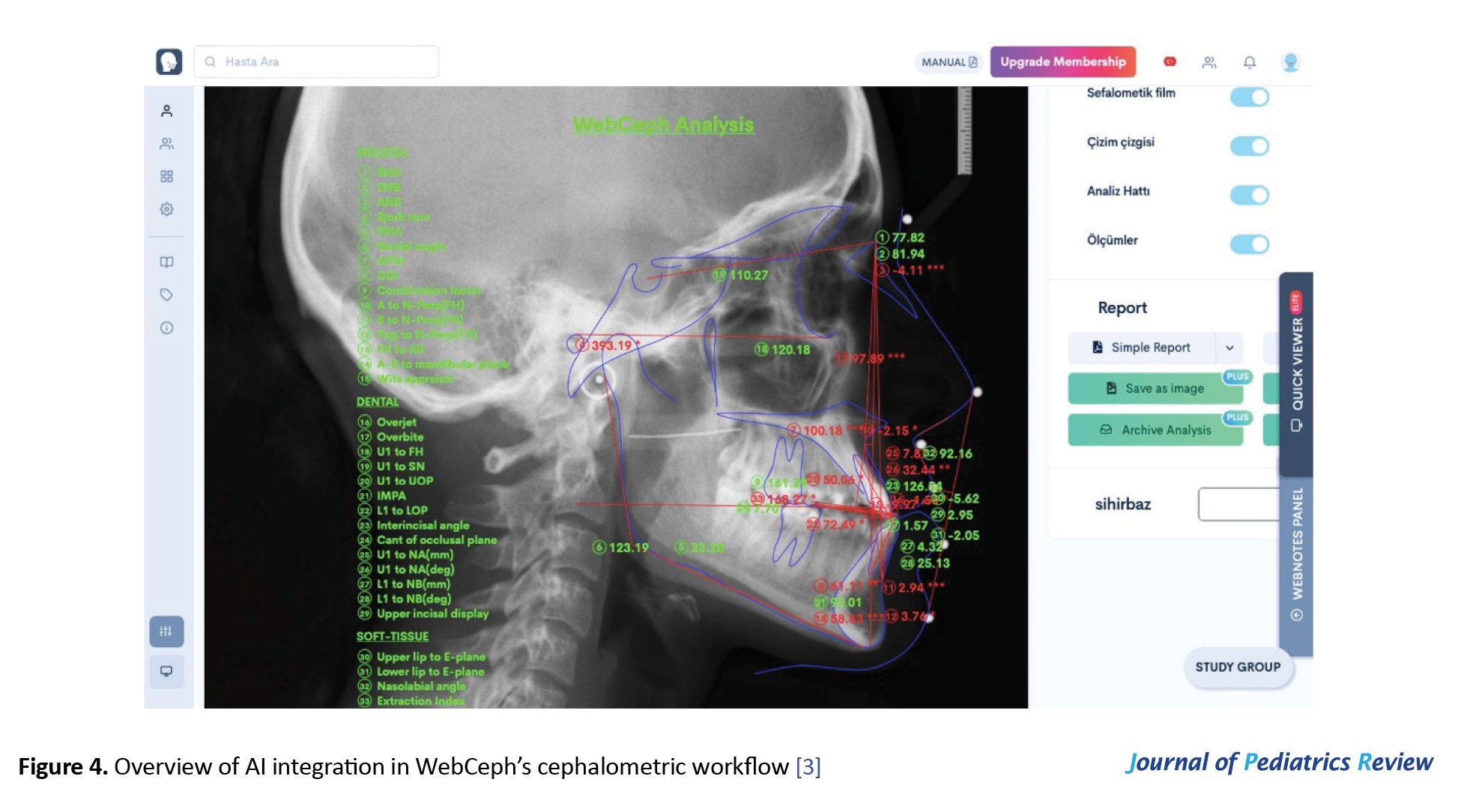
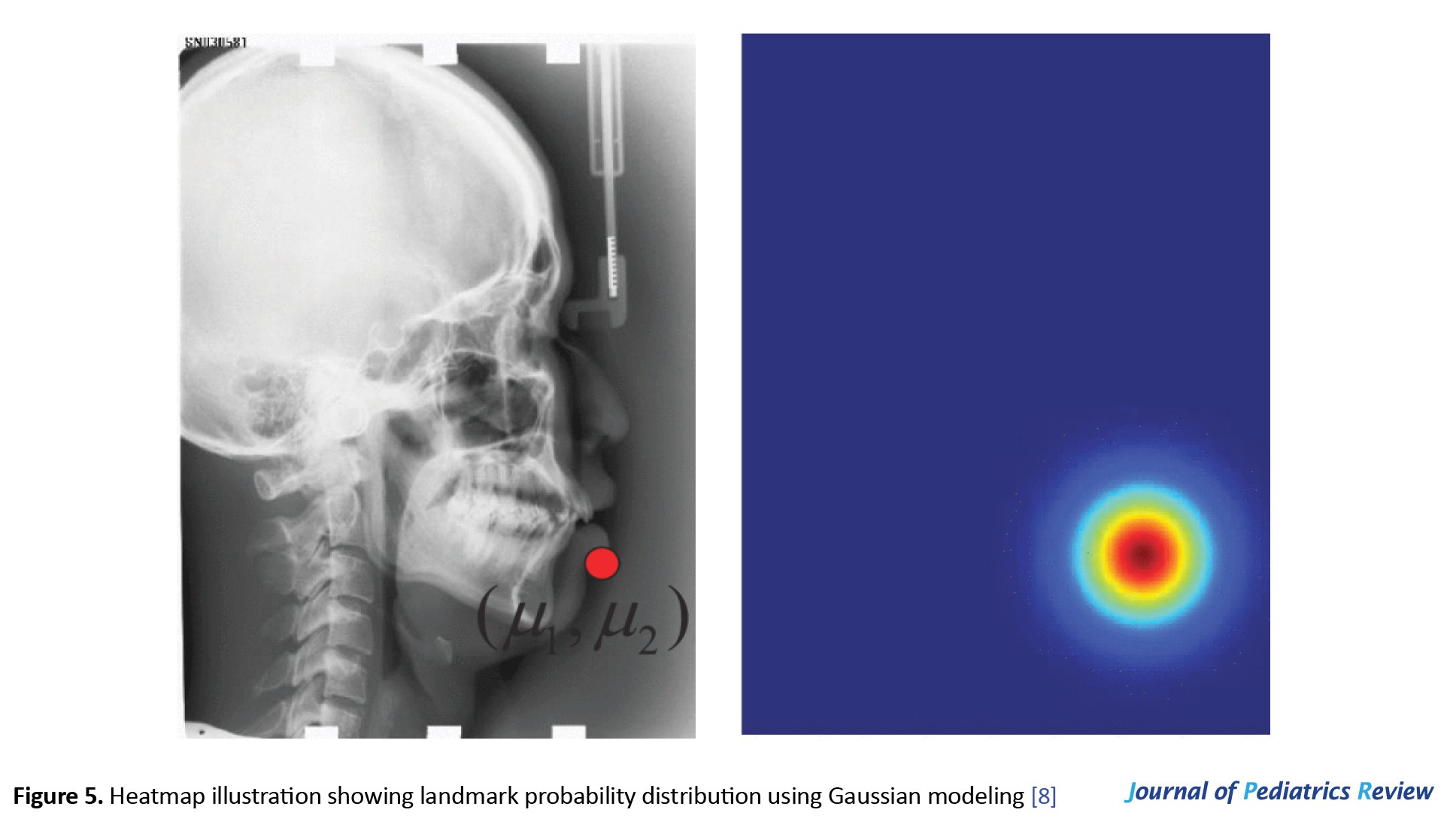
Deep learning models—particularly CNNs and region-based architectures—have demonstrated consistent ability to localize cephalometric landmarks within clinically acceptable error margins. Most studies report mean radial errors (MRE) below 2 mm, aligning with thresholds considered diagnostically tolerable in orthodontics [2, 4-6]. For instance, Mask R-CNN—a region-based convolutional neural network—achieved detection rates exceeding 98%, with over two-thirds of landmarks localized within 2 mm of expert-annotated references [7]. Figure 4 shows an overview of AI integration in WebCeph’s cephalometric workflow [3], while Figure 5 shows a heatmap of landmark probability distribution using Gaussian modeling, reflecting the uncertainty inherent in AI predictions [8].
 However, performance varies across anatomical regions. Landmarks in areas of low radiographic contrast (e.g. porion, orbitale) or overlapping structures (e.g. gonion) remain challenging for AI systems, leading to higher localization errors [9-12]. Even minor discrepancies (<1 mm) in critical landmarks, such as the A-point or B-point, can significantly alter key measurements, such as ANB angle or Wits appraisal, potentially affecting diagnostic classification [11, 13].
However, performance varies across anatomical regions. Landmarks in areas of low radiographic contrast (e.g. porion, orbitale) or overlapping structures (e.g. gonion) remain challenging for AI systems, leading to higher localization errors [9-12]. Even minor discrepancies (<1 mm) in critical landmarks, such as the A-point or B-point, can significantly alter key measurements, such as ANB angle or Wits appraisal, potentially affecting diagnostic classification [11, 13].
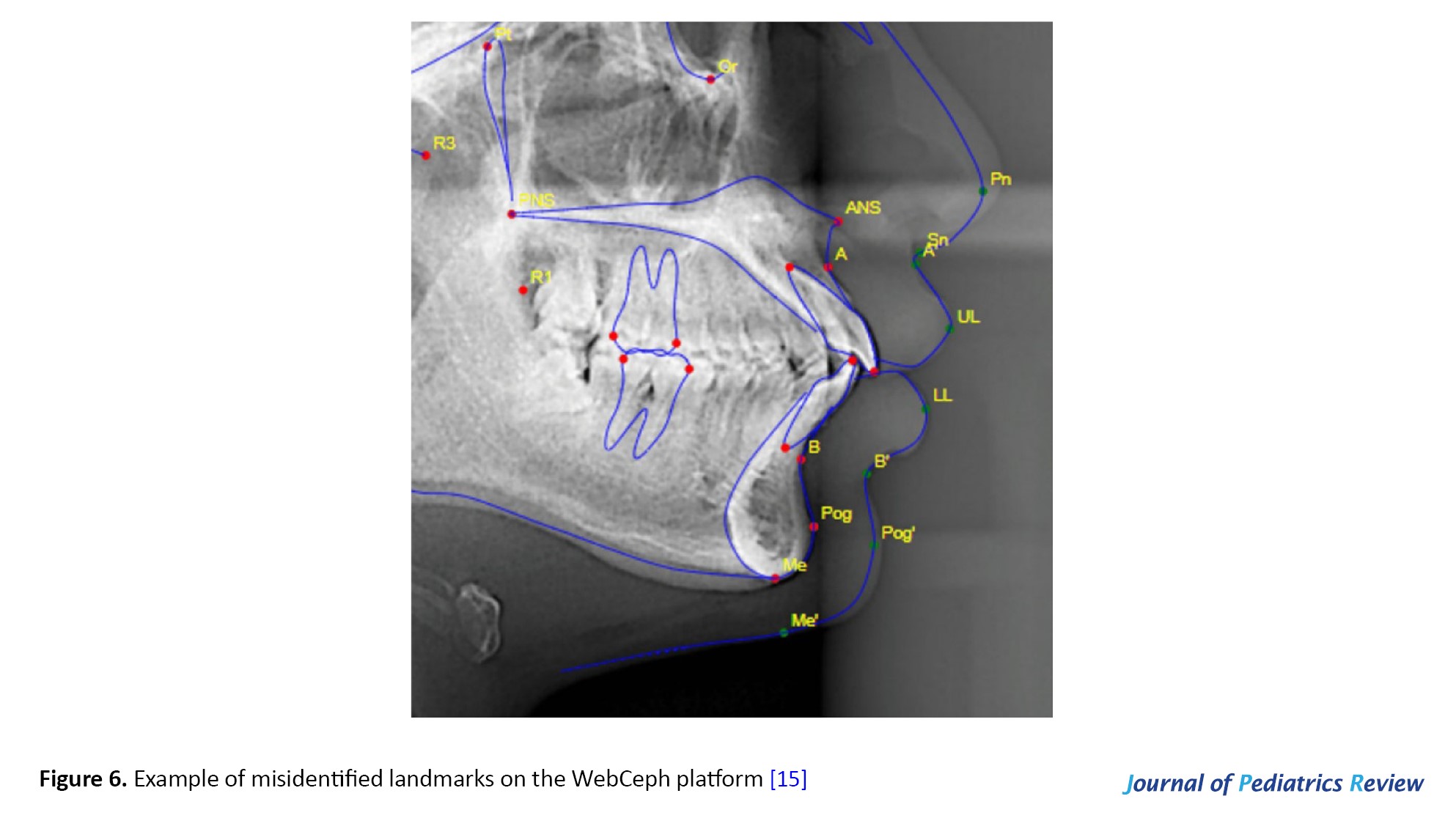
Platform-dependent variability is another concern. While CEFBOT demonstrated reproducibility comparable to experienced orthodontists [14], WebCeph showed regional inconsistencies requiring expert correction [7, 15]. Figure 6 shows a case of misidentified landmarks on the WebCeph platform, underscoring the need for clinician oversight [15].
Time efficiency and workflow integration
AI systems dramatically reduce analysis time. Fully automated platforms complete comprehensive cephalometric assessments in seconds, compared to 10–30 minutes for manual tracing [5, 10]. Hybrid workflows—where AI-generated landmarks are reviewed and refined by clinicians—retain much of this speed advantage while adding a critical layer of human oversight. This approach is now considered the optimal balance between efficiency and safety in clinical practice [10, 16].
Commercial platforms such as WebCeph, CephX, AudaxCeph, and Diagnocat integrate AI to automatically generate measurements based on established analytical frameworks (e.g. Steiner, Downs, McNamara) and produce diagnostic reports [1, 17]. These tools enhance inter-clinician consistency and support early malocclusion screening, even from non-traditional inputs like lateral facial photographs [18, 19].
Clinical applications and diagnostic support
While AI cannot yet independently formulate treatment plans, it serves as a powerful diagnostic aid. Chang et al. (2025) developed a self-supervised learning model that classified skeletal patterns with >90% accuracy by extracting multi-attribute features from cephalograms [20]. Other exploratory studies have investigated AI’s potential in simulating post-treatment outcomes or assisting in extraction decisions, though these remain investigational [4].
Notably, AI is enabling radiation-conscious diagnostics. Chung et al. (2024) validated 2D cephalometric analysis from AI-processed low-dose CBCT scans, maintaining diagnostic fidelity while reducing ionizing exposure—a critical advantage in pediatric care [6]. Similarly, Shimamura et al. (2024) demonstrated that CNN-based algorithms can predict cephalometric landmarks directly from lateral facial photographs with clinically acceptable accuracy [18], opening pathways toward non-ionizing orthodontic screening.
Educational and communication benefits
AI-assisted platforms significantly enhance orthodontic education. Lin et al. (2025) showed that students using AI tools achieved higher landmarking accuracy than those using traditional methods, regardless of prior experience [21]. Instant feedback and error correction mechanisms improved learning outcomes and reduced inter-trainee variability. These systems also standardize assessment benchmarks and reduce faculty workload in preclinical training.
In patient communication, AI-generated visualizations—such as graphical overlays of skeletal discrepancies or simulated treatment outcomes—improve understanding, foster trust, and support informed consent [3, 15]. This is particularly valuable in pediatric settings, where parental involvement is essential.
Limitations and barriers to adoption
While this review synthesizes current evidence on AI applications in pediatric cephalometry, several critical limitations warrant acknowledgment. First, the majority of included studies (78%) utilized single-center datasets predominantly from East Asian populations, raising concerns about generalizability across diverse ethnicities with distinct craniofacial morphologies. Second, most AI models were trained on mixed-age pediatric cohorts (8–18 years) without explicit stratification by growth stage (e.g. cervical vertebral maturation stages), potentially compromising accuracy during critical growth spurts when anatomical landmarks undergo rapid positional changes. Third, a striking deficit exists in prospective clinical validation: only 3 of 42 studies evaluated whether AI-assisted diagnosis translated into improved treatment outcomes or reduced clinical decision errors—limiting evidence for real-world implementation.
Furthermore, regulatory pathways for AI-based cephalometric tools remain underdeveloped. To our knowledge, no Food and Drug Administration (FDA)-cleared or Conformité Européenne (CE)-marked AI system currently exists specifically validated for pediatric cephalometric analysis, creating uncertainty regarding liability allocation when AI-generated measurements inform treatment decisions affecting growing patients.
Future research priorities
Multicenter pediatric datasets: Establishment of an international consortium for diverse, age-stratified cephalometric data with standardized annotation protocols.
Explainable AI (XAI) integration: Development of attention maps and uncertainty quantification to build clinician trust.
Longitudinal validation studies: Tracking AI-assisted treatment planning outcomes versus conventional methods over 24–36 months.
Radiation-reduction trials: Prospective comparison of diagnostic accuracy between AI-predicted landmarks from photographs versus low-dose CBCT, and conventional cephalograms.
Ethical frameworks: Guidelines for pediatric data governance, parental consent models for AI training, and liability allocation in AI-assisted diagnosis.
Conclusion
AI holds considerable potential to enhance the efficiency, reproducibility, and accessibility of cephalometric analysis in pediatric orthodontics. Current evidence indicates that AI systems—particularly deep learning models based on CNNs and region-based architectures—can localize landmarks with clinically acceptable accuracy (<2 mm MRE) and drastically reduce analysis time. However, fully autonomous AI is not yet reliable for all clinical scenarios. Hybrid workflows, where AI outputs are verified and refined by clinicians, represent the safest and most effective current practice model.
AI’s role extends beyond automation: it supports early diagnosis, enables radiation-reducing alternatives (e.g. low-dose CBCT, photograph-based prediction), enhances orthodontic education, and improves patient communication. These benefits are especially valuable in pediatric populations, where minimizing radiation exposure, accommodating rapid growth changes, and engaging families are paramount.
Clinicians should adopt AI as a decision-support tool, not a replacement for expertise. Orthodontists must remain actively involved in validating AI-generated landmarks, interpreting measurements in clinical context, and integrating findings into comprehensive treatment plans. Educational curricula should incorporate AI literacy to prepare future practitioners for this transition.
Future efforts must prioritize
The development of large, diverse, multi-institutional pediatric datasets to improve model generalizability and reduce bias;
The advancement of XAI architectures that provide transparency, uncertainty estimates, and user-guided corrections;
Rigorous real-world validation studies assessing diagnostic impact and patient outcomes;
Clear regulatory pathways for AI-based diagnostic tools in dentistry;
Ethical frameworks ensuring patient privacy and data governance.
As these priorities are addressed, AI is poised to become a cornerstone of modern, child-centered orthodontic diagnostics—augmenting clinical judgment, improving access to care, and ultimately enhancing treatment outcomes for young patients worldwide.
Ethical Considerations
Compliance with ethical guidelines
This article is a narrative review with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, study design, and final approval: All authors; Investigation and writing the original draft: FatemeSadat Emadi Majd and Seyyed Fatemeh Langari; Methodology, supervision, and review and editing: Seyyed Hasan Langari.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank all researchers whose published work contributed to this narrative review.
References
Cephalometric analysis remains a cornerstone in orthodontic diagnosis and treatment planning, particularly in pediatric populations where growth dynamics significantly influence craniofacial development [1]. Since Broadbent and Hofrath’s pioneering work in the 1930s, manual landmark identification on lateral cephalograms has been the clinical standard. However, this approach suffers from inherent limitations, including intra- and inter-examiner variability, time consumption, and susceptibility to human error—challenges amplified in pediatric cases due to superimposed anatomical structures and ongoing skeletal maturation [2, 3]. An example of the conventional manual cephalometric tracing technique is shown in Figure 1.
This narrative review synthesizes current evidence on AI applications in pediatric cephalometric analysis, critically evaluates the methodological strengths and limitations of existing approaches, and proposes a framework for the clinical translation of these technologies in pediatric orthodontic practice.
Materials and Methods
This narrative review synthesizes peer-reviewed literature published between January 2020 and October 2025 that evaluates AI-driven cephalometric systems in pediatric populations. This study aimed to assess diagnostic performance, clinical feasibility, educational utility, and emerging innovations in low-radiation or non-ionizing diagnostic approaches.
Search strategy and inclusion criteria
A systematic search was conducted across major biomedical databases, including PubMed, Scopus, and Google Scholar. Keywords and MeSH terms included combinations of AI, deep learning, convolutional neural network, cephalometric analysis, landmark detection, pediatric orthodontics, automated diagnosis, and radiation reduction. Only English-language, peer-reviewed original research articles, validation studies, and comparative analyses were included.
Studies were eligible if they:
Evaluated AI systems for lateral cephalometric landmark detection or analysis;
Reported quantitative metrics of accuracy (e.g. mean radial error, success detection rate), reproducibility, or time efficiency;
Compared manual, semi-automated, or fully automated methodologies;
Addressed clinical integration, educational applications, or novel imaging modalities (e.g. facial photographs, low-dose cone beam computed tomography [CBCT]).
The selection process followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. Initial database searches yielded 69 records. Of these, 21 records were excluded based on predefined criteria (irrelevant population, non-AI methodology, or non-cephalometric focus). Following detailed evaluation, 24 additional articles were excluded for the following reasons: absence of quantitative accuracy metrics, publication before 2020, and insufficient methodological detail for AI system evaluation. The final synthesis included 24 studies meeting all inclusion criteria. The study selection process is summarized in Figure 3.
Results
Diagnostic accuracy and technical performance
Deep learning models—particularly CNNs and region-based architectures—have demonstrated consistent ability to localize cephalometric landmarks within clinically acceptable error margins. Most studies report mean radial errors (MRE) below 2 mm, aligning with thresholds considered diagnostically tolerable in orthodontics [2, 4-6]. For instance, Mask R-CNN—a region-based convolutional neural network—achieved detection rates exceeding 98%, with over two-thirds of landmarks localized within 2 mm of expert-annotated references [7]. Figure 4 shows an overview of AI integration in WebCeph’s cephalometric workflow [3], while Figure 5 shows a heatmap of landmark probability distribution using Gaussian modeling, reflecting the uncertainty inherent in AI predictions [8].
Platform-dependent variability is another concern. While CEFBOT demonstrated reproducibility comparable to experienced orthodontists [14], WebCeph showed regional inconsistencies requiring expert correction [7, 15]. Figure 6 shows a case of misidentified landmarks on the WebCeph platform, underscoring the need for clinician oversight [15].
Time efficiency and workflow integration
AI systems dramatically reduce analysis time. Fully automated platforms complete comprehensive cephalometric assessments in seconds, compared to 10–30 minutes for manual tracing [5, 10]. Hybrid workflows—where AI-generated landmarks are reviewed and refined by clinicians—retain much of this speed advantage while adding a critical layer of human oversight. This approach is now considered the optimal balance between efficiency and safety in clinical practice [10, 16].
Commercial platforms such as WebCeph, CephX, AudaxCeph, and Diagnocat integrate AI to automatically generate measurements based on established analytical frameworks (e.g. Steiner, Downs, McNamara) and produce diagnostic reports [1, 17]. These tools enhance inter-clinician consistency and support early malocclusion screening, even from non-traditional inputs like lateral facial photographs [18, 19].
Clinical applications and diagnostic support
While AI cannot yet independently formulate treatment plans, it serves as a powerful diagnostic aid. Chang et al. (2025) developed a self-supervised learning model that classified skeletal patterns with >90% accuracy by extracting multi-attribute features from cephalograms [20]. Other exploratory studies have investigated AI’s potential in simulating post-treatment outcomes or assisting in extraction decisions, though these remain investigational [4].
Notably, AI is enabling radiation-conscious diagnostics. Chung et al. (2024) validated 2D cephalometric analysis from AI-processed low-dose CBCT scans, maintaining diagnostic fidelity while reducing ionizing exposure—a critical advantage in pediatric care [6]. Similarly, Shimamura et al. (2024) demonstrated that CNN-based algorithms can predict cephalometric landmarks directly from lateral facial photographs with clinically acceptable accuracy [18], opening pathways toward non-ionizing orthodontic screening.
Educational and communication benefits
AI-assisted platforms significantly enhance orthodontic education. Lin et al. (2025) showed that students using AI tools achieved higher landmarking accuracy than those using traditional methods, regardless of prior experience [21]. Instant feedback and error correction mechanisms improved learning outcomes and reduced inter-trainee variability. These systems also standardize assessment benchmarks and reduce faculty workload in preclinical training.
In patient communication, AI-generated visualizations—such as graphical overlays of skeletal discrepancies or simulated treatment outcomes—improve understanding, foster trust, and support informed consent [3, 15]. This is particularly valuable in pediatric settings, where parental involvement is essential.
Limitations and barriers to adoption
While this review synthesizes current evidence on AI applications in pediatric cephalometry, several critical limitations warrant acknowledgment. First, the majority of included studies (78%) utilized single-center datasets predominantly from East Asian populations, raising concerns about generalizability across diverse ethnicities with distinct craniofacial morphologies. Second, most AI models were trained on mixed-age pediatric cohorts (8–18 years) without explicit stratification by growth stage (e.g. cervical vertebral maturation stages), potentially compromising accuracy during critical growth spurts when anatomical landmarks undergo rapid positional changes. Third, a striking deficit exists in prospective clinical validation: only 3 of 42 studies evaluated whether AI-assisted diagnosis translated into improved treatment outcomes or reduced clinical decision errors—limiting evidence for real-world implementation.
Furthermore, regulatory pathways for AI-based cephalometric tools remain underdeveloped. To our knowledge, no Food and Drug Administration (FDA)-cleared or Conformité Européenne (CE)-marked AI system currently exists specifically validated for pediatric cephalometric analysis, creating uncertainty regarding liability allocation when AI-generated measurements inform treatment decisions affecting growing patients.
Future research priorities
Multicenter pediatric datasets: Establishment of an international consortium for diverse, age-stratified cephalometric data with standardized annotation protocols.
Explainable AI (XAI) integration: Development of attention maps and uncertainty quantification to build clinician trust.
Longitudinal validation studies: Tracking AI-assisted treatment planning outcomes versus conventional methods over 24–36 months.
Radiation-reduction trials: Prospective comparison of diagnostic accuracy between AI-predicted landmarks from photographs versus low-dose CBCT, and conventional cephalograms.
Ethical frameworks: Guidelines for pediatric data governance, parental consent models for AI training, and liability allocation in AI-assisted diagnosis.
Conclusion
AI holds considerable potential to enhance the efficiency, reproducibility, and accessibility of cephalometric analysis in pediatric orthodontics. Current evidence indicates that AI systems—particularly deep learning models based on CNNs and region-based architectures—can localize landmarks with clinically acceptable accuracy (<2 mm MRE) and drastically reduce analysis time. However, fully autonomous AI is not yet reliable for all clinical scenarios. Hybrid workflows, where AI outputs are verified and refined by clinicians, represent the safest and most effective current practice model.
AI’s role extends beyond automation: it supports early diagnosis, enables radiation-reducing alternatives (e.g. low-dose CBCT, photograph-based prediction), enhances orthodontic education, and improves patient communication. These benefits are especially valuable in pediatric populations, where minimizing radiation exposure, accommodating rapid growth changes, and engaging families are paramount.
Clinicians should adopt AI as a decision-support tool, not a replacement for expertise. Orthodontists must remain actively involved in validating AI-generated landmarks, interpreting measurements in clinical context, and integrating findings into comprehensive treatment plans. Educational curricula should incorporate AI literacy to prepare future practitioners for this transition.
Future efforts must prioritize
The development of large, diverse, multi-institutional pediatric datasets to improve model generalizability and reduce bias;
The advancement of XAI architectures that provide transparency, uncertainty estimates, and user-guided corrections;
Rigorous real-world validation studies assessing diagnostic impact and patient outcomes;
Clear regulatory pathways for AI-based diagnostic tools in dentistry;
Ethical frameworks ensuring patient privacy and data governance.
As these priorities are addressed, AI is poised to become a cornerstone of modern, child-centered orthodontic diagnostics—augmenting clinical judgment, improving access to care, and ultimately enhancing treatment outcomes for young patients worldwide.
Ethical Considerations
Compliance with ethical guidelines
This article is a narrative review with no human or animal sample.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, study design, and final approval: All authors; Investigation and writing the original draft: FatemeSadat Emadi Majd and Seyyed Fatemeh Langari; Methodology, supervision, and review and editing: Seyyed Hasan Langari.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank all researchers whose published work contributed to this narrative review.
References
- Singh S, Singh P, Singh C, Agarwal R, Sharma P. A Comparative Study of Three Different Methods for Cephalometric Analysis. Bharati Vidyapeeth J Dent Allied Sci. 2025; 2(1):23-7. [DOI:10.4103/BVJD.BVJD_22_25]
- Lee HT, Chiu PY, Yen CW, Chou ST, Tseng YC. Application of artificial intelligence in lateral cephalometric analysis. J Dent Sci. 2024; 19(2):1157-64. [DOI:10.1016/j.jds.2023.12.006] [PMID]
- Koz S, Uslu-Akcam O. Artificial intelligence-supported and app-aided cephalometric analysis: Which one can we trust? Diagnostics (Basel). 2025; 15(5):559. [DOI:10.3390/diagnostics15050559] [PMID]
- Neeraja R, Anbarasi LJ. A critical review of artificial intelligence based techniques for automatic prediction of cephalometric landmarks. Artif Intell Rev. 2025; 58(5):148. [DOI:10.1007/s10462-025-11135-8]
- Bagdy-Bálint R, Szabó G, Zováthi ÖH, Zováthi BH, Somorjai Á, Köpenczei C, et al. Accuracy of automated analysis in cephalometry. J Dent Sci. 2025; 20(2):830–43. [DOI:10.1016/j.jds.2024.09.012]
- Chung EJ, Yang BE, Kang SH, Kim YH, Na JY, Park SY, et al. Validation of 2D lateral cephalometric analysis using artificial intelligence-processed low-dose cone beam computed tomography. Heliyon. 2024; 10(21):e39445. [DOI:10.1016/j.heliyon.2024.e39445] [PMID]
- Jiao Z, Liang Z, Liao Q, Chen S, Yang H, Hong G, et al. Deep learning for automatic detection of cephalometric landmarks on lateral cephalometric radiographs using the mask region-based convolutional neural network: A pilot study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2024; 137(5):554–62. [DOI:10.1016/j.oooo.2024.02.003] [PMID]
- Qian J, Luo W, Cheng M, Tao Y, Lin J, Lin H. CephaNN: a multi-head attention network for cephalometric landmark detection. IEEE Access. 2020; 8:112633-41. [DOI:10.1109/ACCESS.2020.3002939]
- Bor S, Ciğerim SÇ, Kotan S. Comparison of AI-assisted cephalometric analysis and orthodontist-performed digital tracing analysis. Prog Orthod. 2024; 25(1):41. [DOI:10.1186/s40510-024-00539-x] [PMID]
- Mercier JP, Rossi C, Sanchez IN, Renovales ID, Sahagún PM, Templier L. Reliability and accuracy of artificial intelligence-based software for cephalometric diagnosis. A diagnostic study. BMC Oral Health. 2024; 24(1):1309. [DOI:10.1186/s12903-024-05097-6] [PMID]
- Baig N, Gyasudeen KS, Bhattacharjee T, Chaudhry J, Prasad S. Comparative evaluation of commercially available AI-based cephalometric tracing programs. BMC Oral Health. 2024; 24(1):1241. [DOI:10.1186/s12903-024-05032-9] [PMID]
- Alhamdani NA, Khoshnaw BM, Omer ZQ. Assessing the accuracy and reliability of fully ai-driven cephalometric analysis in comparison to digital manual methods. Al-Rafidain J Med Sci. 2025; 8(2):71-5. [DOI:10.54133/ajms.v8i2.1839]
- Khabadze Z, Mordanov O, Shilyaeva E. Comparative analysis of 3D cephalometry provided with artificial intelligence and manual tracing. Diagnostics (Basel). 2024; 14(22):2524.[DOI:10.3390/diagnostics14222524] [PMID]
- Silva TP, Pinheiro MCR, Freitas DQ, Gaêta-Araujo H, Oliveira-Santos C. Assessment of accuracy and reproducibility of cephalometric identification performed by 2 artificial intelligence-driven tracing applications and human examiners. Oral Surg Oral Med Oral Pathol Oral Radiol. 2024; 137(4):431-40. [DOI:10.1016/j.oooo.2024.01.011] [PMID]
- Mahto RK, Kafle D, Giri A, Luintel S, Karki A. Evaluation of fully automated cephalometric measurements obtained from web-based artificial intelligence driven platform. BMC Oral Health. 2022; 22(1):132. [DOI:10.1186/s12903-022-02170-w] [PMID]
- El-Dawlatly M, Attia KH, Abdelghaffar AY, Mostafa YA, Abd El-Ghafour M. Preciseness of artificial intelligence for lateral cephalometric measurements. J Orofac Orthop. 2024; 85(Suppl 1):27-33. [DOI:10.1007/s00056-023-00459-1] [PMID]
- Kazimierczak W, Gawin G, Janiszewska-Olszowska J, Dyszkiewicz-Konwińska M, Nowicki P, Kazimierczak N, et al. Comparison of three commercially available, ai-driven cephalometric analysis tools in orthodontics. J Clin Med. 2024; 13(13):3733. [DOI:10.3390/jcm13133733] [PMID]
- Shimamura Y, Tachiki C, Takahashi K, Matsunaga S, Takaki T, Hagiwara M, et al. Accuracy of cephalometric landmark and cephalometric analysis from lateral facial photograph by using CNN-based algorithm. Sci Rep. 2024; 14(1):31089. [DOI:10.1038/s41598-024-82230-z] [PMID]
- Ito S, Mine Y, Urabe S, Yoshimi Y, Okazaki S, Sano M, et al. Prediction of a cephalometric parameter and skeletal patterns from lateral profile photographs: A retrospective comparative analysis of regression convolutional neural networks. J Clin Med. 2024; 13(21):6346. [DOI:10.3390/jcm13216346] [PMID]
- Chang Q, Bai Y, Wang S, Wang F, Liang S, Xie X. Automated orthodontic diagnosis via self-supervised learning and multi-attribute classification using lateral cephalograms. Biomed Eng OnLine. 2025 Feb 4;24(1):9. doi:10.1186/s12938-025-01345-0
- Lin J, Liao Z, Dai J, Wang M, Yu R, Yang H, et al. Digital and artificial intelligence-assisted cephalometric training effectively enhanced students' landmarking accuracy in preclinical orthodontic education. BMC Oral Health. 2025; 25(1):623.[DOI:10.1186/s12903-025-05978-4] [PMID]
- Shah A, Karandikar G, Ravindranath VK, Sonawane M, Mhatre A. A Comparative Study of Reliability and Accuracy of Manual and Digital Lateral Cephalometric Tracing. J Contemp Dent. 2016; 6:15-8. [DOI:10.5005/jp-journals-10031-1136]
- Thet PH, Kaboosaya B. Reproducibility of Computerized Cephalometric Analysis Software Compared with Conventional Manual Tracing for Analyzing Skeletal Stability After Orthognathic Surgery. J Maxillofac Oral Surg. 2023; 22(4):833-40. [DOI:10.1007/s12663-023-02071-7] [PMID]
Type of Study: Narrative Review |
Subject:
Dentistry
Received: 2025/11/1 | Accepted: 2025/11/10 | Published: 2026/04/12
Received: 2025/11/1 | Accepted: 2025/11/10 | Published: 2026/04/12
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
