
Sat, May 4, 2024

Volume 11, Issue 2 (4-2023)
J. Pediatr. Rev 2023, 11(2): 179-186 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bhanja S, Mitra S, Krishna De J. Does the Childhood Obesity Require Special Attention? A Cross-sectional Pilot Study. J. Pediatr. Rev 2023; 11 (2) :179-186
URL: http://jpr.mazums.ac.ir/article-1-456-en.html
URL: http://jpr.mazums.ac.ir/article-1-456-en.html



1- Department of Pediatrics, Jagannath Gupta Institute of Medical Sciences, Kolkata, India. , drsushantabhanja@gmail.com
2- Department of Community Medicine, Jagannath Gupta Institute of Medical Sciences, KPC Medical College and Hospital, Kolkata, India.
3- Department of Radiology, Jagannath Gupta Institute of Medical Sciences, Kolkata, India.
2- Department of Community Medicine, Jagannath Gupta Institute of Medical Sciences, KPC Medical College and Hospital, Kolkata, India.
3- Department of Radiology, Jagannath Gupta Institute of Medical Sciences, Kolkata, India.
Keywords: Childhood obesity, Carotid intima-medial thickness, Developing countries, Cross-sectional study, Physical inactivity
Full-Text [PDF 418 kb]
(751 Downloads)
| Abstract (HTML) (1077 Views)
Full-Text: (285 Views)
Introduction
World Health Organization (WHO) defines overweight and obesity as ‘abnormal or excessive fat accumulation in fatty tissues (adipose tissue mass) that may impair health [1]. Overweight and obesity are measured by body mass index (BMI) which is calculated by body weight (kg.) divided by height squared (m2) [2]. Once upon a time, overweight and obesity were considered as a high-income country problem but currently it is 30% higher in low and middle-income countries compared to high-income ones [3] These developing nations are residents of over 30 million overweight and obese children [4]. Obesity, is itself a budding disease besides being a risk factor for several non-communicable diseases (NCD). Childhood obesity is associated with numerous health problems like asthma, early onset type 2 diabetes, and cardiovascular diseases [5]. Obese children are more likely to suffer from mental health and behavioral problems and may have long-term health consequences, as childhood obesity is a strong predictor of adult obesity, premature death, and disability in adulthood [6].
According to the national health and nutrition examination survey 2015-16, the worldwide prevalence of obesity among adolescents was 20.6%, among school-aged children 18.4%, and 13.9% among preschool-age children [7].
As a by-product of growth and development, different NCDs with their risk factors are engulfing the developing nations too and India is being grasped fast. Physical inactivity, preferences towards social media and virtual gaming, lifestyle changes especially changes in dietary habits in the form of increased consumption of canned/dried processed and junk foods, sweetened beverages, processed dairy products, and savory snacks are the main driving forces behind it. Besides, there are uncontrolled eating, binge eating, continued consumption of high-calorie foods despite the knowledge of its negative consequences, and inability to cut down despite the desire to do so [8]. Most eating disorders begin in childhood and adolescence. Night-eating syndrome is another disorder that can lead to significant weight gain among children. These lifestyle factors develop at individual as well as family levels and as the eating behavior among children is hugely contributed by peers, the community has a contagious role in the adoption of unhealthy habits [9]. According to the World Health Organization (WHO), exclusive breastfeeding can protect children against childhood obesity. Studies conducted in other countries have shown an association between these two [10-12].
Carotid intima-media thickness (CIMT) measurement can be used as a predictor of increased risk of future development of cardiovascular diseases, obesity, hypertension, and chronic kidney disease compared to the general population [13-15].
A systematic review conducted by Ranjani et al. (2012) reported that the prevalence of overweight among 5 to 19 years children, ranged between 6.1 and 25.2% while that of obesity was between 3.6 to 11.7% which is enough alarming [16]. A systematic review and meta-analysis from Bangladesh showed similar findings [17]. There are sporadic studies conducted in different parts of the country addressing childhood obesity but uniformity was not found among them in aspects like age group as study population, methods of assessment, etc. Above all, neither any national-level data are available on the prevalence of childhood obesity nor has any health program started rolling on yet addressing it. After an extensive literature search, no data have been found on the current status of this burning issue at the district level as well as the predictive potential of CIMT at the country level also.
With this backdrop, the researchers planned to conduct a pilot study to assess the prevalence of different risk variables of childhood obesity and the effects of its determinants in a fast-growing semi-urban area and hence adopt the goods and evils of urbanization.
Methods
A descriptive observational study was conducted from February to July 2020 among children aged 5-18 years attending the outpatient department of Pediatrics of a remotely located medical college situated in the south 24 Parganas district of West Bengal. The children suffering from any kind of long-standing physical and or mental disabilities and the attendants of the children who did not give consent for participation were excluded from the study. As the prevalence of childhood overweight in West Bengal was found to be 22.57% [5], taking the allowable error to 10%, the sample size was calculated as 68. Assuming the non-response rate to be 10%, the calculated and rounded-off sample size was 75. With a pre-designed pre-tested questionnaire, the data were collected on basic demographic characteristics like as, age in completed years, gender, caste, religion, educational qualification of both the parents in terms of last examination passed, occupation of both the parents, per capita monthly income, and socioeconomic status using B.G. Prasad’s SES scale. The weight of the children at birth and vaccination status was taken, if available. physical activity questionnaire for older children (PAQ-C) and for adolescents (PAQ-A) [18] were used to assess the physical activity level (PAL) of the participants preceding one week of data collection. The participants were undergone with complete blood count, lipid profile, and liver function tests. With the help of a stadiometer, standing height was recorded, and calibrated weighing machine was used for taking weight in kgs. All CIMT measurements were done with a high-resolution B-mode Ultrasonography. Three measurements were taken and an average of these three was used for the final analysis of CIMT. The questionnaire was undergone with content validity testing by subject matter experts from the Department of Pediatrics, General Medicine, Radiodiagnosis, and Community Medicine of the study setting among those who did not have any involvement in the study itself. For the language validation, two forward and two backward translations were done in parallel by two language experts, so that the meaning and contents of the items remained unaltered as well as sentences were grammatically correct. The questionnaire was pre-tested in January 2020 among 15 children from a healthcare setting situated in the same district thereby assumed to share similar characteristics. These children and or the findings were not included in the study properly.
As all the study participants were aged less than 18 years, assent was obtained from the guardian or responsible accompanying person. From the Institutional Ethics Committee, ethical permission was taken before the commencement of the study.
Data were entered in a Microsoft Excel spreadsheet. Analysis was done with the help of SPSS software, version 22 free, Epi InfoTM version 7 free, and Microsoft Excel. The anthropometric calculation (BMI-for-age-sex) was conducted using WHO Anthro plus software, version 1.0.4. The dependent variable of the study was overweight/obesity which was based on the BMI for the age-sex of the children. “Overweight” was defined as having a BMI for age between the eighty fifth and ninety fifth percentiles, and “obesity” was defined as having the BMI-for-age at or above the ninety fifth percentile. Descriptive statistics were expressed by Mean±SD, and proportion. The relationship between socio-demographic factors and outcome was established by using inferential statistics like Chi-square tests and a P<0.05 was considered significant at 95% of a confidence interval. Binary logistic regression was used to test the association of the educational status of parents, socio-economic factors, and different laboratory parameters. The internal consistency of PAQ-C and PAQ-A was shown by Cronbach’s α. The association of PAQ-C and PAQ-A with influencing factors was done by non-parametric tests like the Kruskal-Wallis ANOVA test.
Results
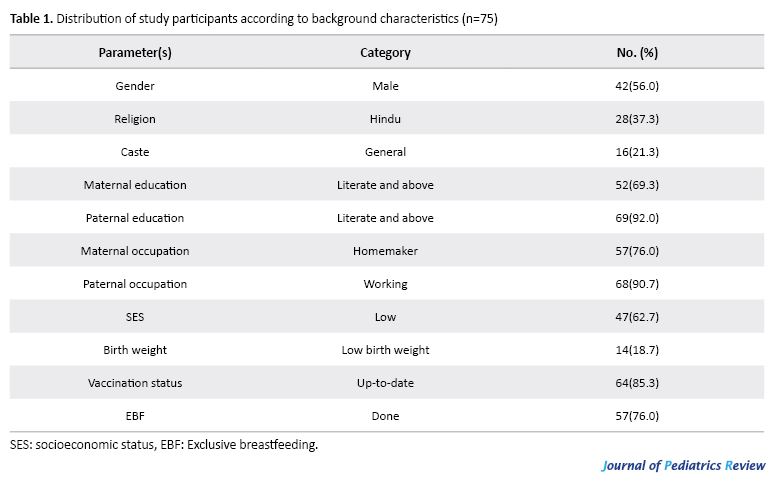
Childhood obesity is a multidimensional state evolving through non-linear interaction and a combination of factors namely, parental education, socioeconomic factors, exclusive breastfeeding different laboratory parameters, physical activity level, and pattern, to prove experiential or empirical evidence. Among the total participants, the majority, 42(56.0%) were male and 33(44.0%) were females. A bit more than one-third was Hindu by faith and belief and nearly one-fifth belonged general caste. Nearly one-third of the mothers of the children were found never to attend school and this is 10% for fathers of the participants. Among the mothers, 24% were found to work outside the side and most of them are involved in unorganized sectors mainly as daily-based laborers. The majority of the fathers of the children under study were found to work and be involved in rickshaw pulling, daily labor, domestic servant, carpentry, mechanic/electrician and vendor, etc. More than fifty percent of the participants were from low socio-economic strata. More than 75% of the children claimed to receive exclusive breastfeeding (Table 1).
Regarding parental education as a determinant, more childhood obesity was found among those born to parents educated up to the primary level and the difference to illiterate mothers was significant. Regarding the occupation of the parents, the majority of the homemaker mothers’ children were overweight and obese. Out of 18 children who were not breastfed exclusively, 12(66.7%) were overweight and obese but it was not found to be statistically significant [not displayed].
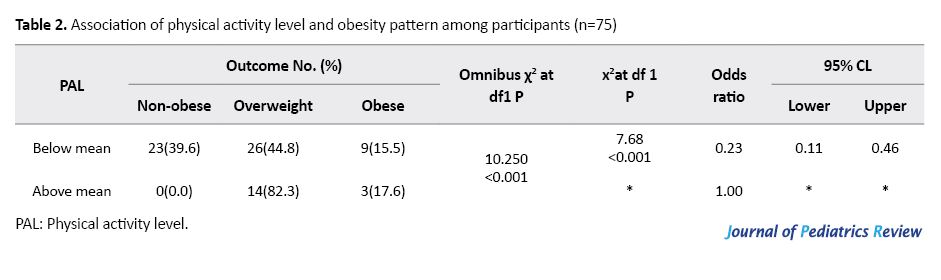
Physical activity level (PAL) among both the older children as well as adolescents was Mean±SD 21.87±9.11. Only 17(22.7%) had PAL above the mean for the preceding seven days of data collection. Omnibus x2 at df 3 shows a significant P with the help of Epi info (version 7) in reference to non-obese. The table revealed that compared to the non-obese, those who were overweight and obese were 0.23 times (CL 0.11-0.46) more likely to have low physical activity levels. The difference was statistically significant (P<0.05). In the table stars are for reference values. (Table 2).
In the chi-square test, overweight and obesity were found to be more among male children, those belonging to low socio-economic status, and low physical activity levels, and these were found to be statistically significant (Table 3).

Children who were found overweight and obese, on in-depth interviewing were found to have preferences for street foods, junk foods, sweets and sugar, intake of food in-between meals, and beverages. Many of the parents of small children stated that they cannot keep sugar, milk powder, sweets, etc. within reach of the children. One of the working mothers told, “If I don’t bring either of the street foods while coming back home, my adolescent boy creates a huge mess evening beating his younger sister out of anger……”
Binary logistic regression revealed that a statistically significant association (P<0.05 between of childhood overweight and obesity were observed by birth weight (AOR 1.45, 95% CL 1.34-11.64), exclusive breastfeeding (AOR 3.12, 95% CL 2.75-12.42), high lipid profile (AOR 5.11, 95% CL 2.17-11.58), high liver function tests (AOR 3.40, 95% CL 1.49-12.86), high fasting blood sugar (AOR 5.02, 95% CL 1.34-16.56), low physical activity level (AOR 3.70, 95% CL 1.34-7.79), and high CIMT value (AOR 4.11, 95% CL 1.11-12.09); while male gender and high SES was not significant. The Hosmer and Lameshow test (x2= 9.278, df=4, P=0.934) proved the regression model fit of the data well. In the table stars are for reference values. (Table 4).

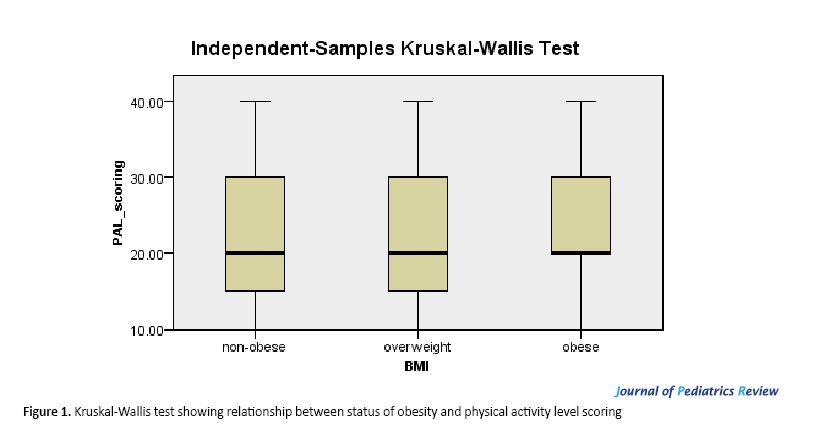
In the Kruskal-Wallis ANOVA test, the PAL score for non-obese showed a mean score of 39.93, for overweight 36.38, and obese children 33.71 and these were significant for overweight (P=0.04) and obesity (P=0.002) (Figure 1).
Discussion
Childhood obesity is a recognized precursor for various non-communicable diseases and related complications increasing overall disease burden and out-of-pocket expenditure at its present level and during adulthood. The majority of the nutrition-related national health programs are concentrated on undernutrition and people are still in belief of obesity as a sign of good health especially for children.
The proportion of children found to be overweight and obese in the current study area, itself being a non-privileged one is quite worrisome. A study conducted in Rajasthan by Jain et al. found nearly 40% of study children to be overweight and obese [9], a Telengana-based study revealed more than 2/3rd of the study participants to have weight far above the normal [19], and similar findings were obtained from a population-based study conducted in Pakistan [20]. These findings point toward the burden of childhood obesity in these developing nations too. The male preponderance of childhood overweight and obesity had similarities with a study conducted among primary school children in urban Nepal [21]. But a study from Delhi by Kaur, [22] in South Africa by Armstrong [23], Song from China [24], and Ahmed from Pakistan [25] showed female propensity of childhood obesity in their respective study areas. In contrast to the current study findings, parents with higher education, especially mothers were not protected in studies from urban Nepal [21], rural South India [4]. It can be presumed that among the study population higher education was responsible for awareness generation among parents. Mothers who were found as homemakers had more obese children in the present study; this might be because of the conventional belief of obesity as a marker of good health and proper child care. But these findings were not in accordance with other studies [21, 22]. The protective role of exclusive breastfeeding against obesity as found in the current study has supportive evidence from NFHS-III. One of the most alarming findings in the current study is that a higher proportion of children from low SES are overweight and obese which is somewhat similar to the study from Rajasthan [9] but evidence from urban Nepal was different [21]. There are dubious findings regarding this matter from different parts of the world [3, 8].
Regarding the physical activity level and types, in accordance with the current study, the protective role was established by studies by Jain [9] Prashanth et al. [26], Goyal et al. [27], and Keerthan et al. [28]. The pattern of physical activity level as found in the present study for the previous one week was also supported by Goyal et al. [27] and also from a study conducted in North India in 2009. A study conducted in urban Nepal [21] had no significant association in this regard contrary to others including the current study which may have been caused by mean rank on the non-parametric statistical tests. The CIMT measurement of the study was found to have supporting evidence from Baroncini et al. [13], Brady et al. [29], Mehta et al. [30] and from Maharashtra, India. As in logistic regression findings of the current study considering the effects of confounders, those showing significance in the univariate analysis except FBS and birth weight, being the researcher’s choices, the findings were corroborative to that form Karki [21], Azagba et al. [31].
Conclusion
Childhood obesity is on the rise and is the momentum to be the pandemic of the 21st century. In the study area with semi-urban background, the cross-section of the population showed alarming evidence for it. Factors showing a significant positive impact on it like exclusive breastfeeding, lipid profile, blood sugar level, liver function tests, physical activity level, and carotid intima-media thickness are modifiable risk factors and hence the definite role of primordial and primary preventive measures can be taken for their control.
Limitations
This study was conducted on a pilot basis and hence the studied population was low in number. Dietary history in detail was not taken into account. A future prospective study preferably with a mixed-methods approach with non-participant observation for especially dietary and lifestyle factors to explore in-depth and follow-up of CIMT for the development of non-communicable diseases and providing interventions is recommended.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted with approval of Jagannath Gupta Institute of Medical Sciences and Hospital. Informed consent was obtained from the legal guardians (father-mother) of each patient (younger children) included in the study
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors contributions
All authors equally contributed to preparing this article.
Conflicts of interest
The authors declared no conflicts of interest.
Acknowledgements
The authors are very grateful to all hospital authorities for their permission to conduct this study and for all kinds of cooperation.
References
World Health Organization (WHO) defines overweight and obesity as ‘abnormal or excessive fat accumulation in fatty tissues (adipose tissue mass) that may impair health [1]. Overweight and obesity are measured by body mass index (BMI) which is calculated by body weight (kg.) divided by height squared (m2) [2]. Once upon a time, overweight and obesity were considered as a high-income country problem but currently it is 30% higher in low and middle-income countries compared to high-income ones [3] These developing nations are residents of over 30 million overweight and obese children [4]. Obesity, is itself a budding disease besides being a risk factor for several non-communicable diseases (NCD). Childhood obesity is associated with numerous health problems like asthma, early onset type 2 diabetes, and cardiovascular diseases [5]. Obese children are more likely to suffer from mental health and behavioral problems and may have long-term health consequences, as childhood obesity is a strong predictor of adult obesity, premature death, and disability in adulthood [6].
According to the national health and nutrition examination survey 2015-16, the worldwide prevalence of obesity among adolescents was 20.6%, among school-aged children 18.4%, and 13.9% among preschool-age children [7].
As a by-product of growth and development, different NCDs with their risk factors are engulfing the developing nations too and India is being grasped fast. Physical inactivity, preferences towards social media and virtual gaming, lifestyle changes especially changes in dietary habits in the form of increased consumption of canned/dried processed and junk foods, sweetened beverages, processed dairy products, and savory snacks are the main driving forces behind it. Besides, there are uncontrolled eating, binge eating, continued consumption of high-calorie foods despite the knowledge of its negative consequences, and inability to cut down despite the desire to do so [8]. Most eating disorders begin in childhood and adolescence. Night-eating syndrome is another disorder that can lead to significant weight gain among children. These lifestyle factors develop at individual as well as family levels and as the eating behavior among children is hugely contributed by peers, the community has a contagious role in the adoption of unhealthy habits [9]. According to the World Health Organization (WHO), exclusive breastfeeding can protect children against childhood obesity. Studies conducted in other countries have shown an association between these two [10-12].
Carotid intima-media thickness (CIMT) measurement can be used as a predictor of increased risk of future development of cardiovascular diseases, obesity, hypertension, and chronic kidney disease compared to the general population [13-15].
A systematic review conducted by Ranjani et al. (2012) reported that the prevalence of overweight among 5 to 19 years children, ranged between 6.1 and 25.2% while that of obesity was between 3.6 to 11.7% which is enough alarming [16]. A systematic review and meta-analysis from Bangladesh showed similar findings [17]. There are sporadic studies conducted in different parts of the country addressing childhood obesity but uniformity was not found among them in aspects like age group as study population, methods of assessment, etc. Above all, neither any national-level data are available on the prevalence of childhood obesity nor has any health program started rolling on yet addressing it. After an extensive literature search, no data have been found on the current status of this burning issue at the district level as well as the predictive potential of CIMT at the country level also.
With this backdrop, the researchers planned to conduct a pilot study to assess the prevalence of different risk variables of childhood obesity and the effects of its determinants in a fast-growing semi-urban area and hence adopt the goods and evils of urbanization.
Methods
A descriptive observational study was conducted from February to July 2020 among children aged 5-18 years attending the outpatient department of Pediatrics of a remotely located medical college situated in the south 24 Parganas district of West Bengal. The children suffering from any kind of long-standing physical and or mental disabilities and the attendants of the children who did not give consent for participation were excluded from the study. As the prevalence of childhood overweight in West Bengal was found to be 22.57% [5], taking the allowable error to 10%, the sample size was calculated as 68. Assuming the non-response rate to be 10%, the calculated and rounded-off sample size was 75. With a pre-designed pre-tested questionnaire, the data were collected on basic demographic characteristics like as, age in completed years, gender, caste, religion, educational qualification of both the parents in terms of last examination passed, occupation of both the parents, per capita monthly income, and socioeconomic status using B.G. Prasad’s SES scale. The weight of the children at birth and vaccination status was taken, if available. physical activity questionnaire for older children (PAQ-C) and for adolescents (PAQ-A) [18] were used to assess the physical activity level (PAL) of the participants preceding one week of data collection. The participants were undergone with complete blood count, lipid profile, and liver function tests. With the help of a stadiometer, standing height was recorded, and calibrated weighing machine was used for taking weight in kgs. All CIMT measurements were done with a high-resolution B-mode Ultrasonography. Three measurements were taken and an average of these three was used for the final analysis of CIMT. The questionnaire was undergone with content validity testing by subject matter experts from the Department of Pediatrics, General Medicine, Radiodiagnosis, and Community Medicine of the study setting among those who did not have any involvement in the study itself. For the language validation, two forward and two backward translations were done in parallel by two language experts, so that the meaning and contents of the items remained unaltered as well as sentences were grammatically correct. The questionnaire was pre-tested in January 2020 among 15 children from a healthcare setting situated in the same district thereby assumed to share similar characteristics. These children and or the findings were not included in the study properly.
As all the study participants were aged less than 18 years, assent was obtained from the guardian or responsible accompanying person. From the Institutional Ethics Committee, ethical permission was taken before the commencement of the study.
Data were entered in a Microsoft Excel spreadsheet. Analysis was done with the help of SPSS software, version 22 free, Epi InfoTM version 7 free, and Microsoft Excel. The anthropometric calculation (BMI-for-age-sex) was conducted using WHO Anthro plus software, version 1.0.4. The dependent variable of the study was overweight/obesity which was based on the BMI for the age-sex of the children. “Overweight” was defined as having a BMI for age between the eighty fifth and ninety fifth percentiles, and “obesity” was defined as having the BMI-for-age at or above the ninety fifth percentile. Descriptive statistics were expressed by Mean±SD, and proportion. The relationship between socio-demographic factors and outcome was established by using inferential statistics like Chi-square tests and a P<0.05 was considered significant at 95% of a confidence interval. Binary logistic regression was used to test the association of the educational status of parents, socio-economic factors, and different laboratory parameters. The internal consistency of PAQ-C and PAQ-A was shown by Cronbach’s α. The association of PAQ-C and PAQ-A with influencing factors was done by non-parametric tests like the Kruskal-Wallis ANOVA test.
Results
Childhood obesity is a multidimensional state evolving through non-linear interaction and a combination of factors namely, parental education, socioeconomic factors, exclusive breastfeeding different laboratory parameters, physical activity level, and pattern, to prove experiential or empirical evidence. Among the total participants, the majority, 42(56.0%) were male and 33(44.0%) were females. A bit more than one-third was Hindu by faith and belief and nearly one-fifth belonged general caste. Nearly one-third of the mothers of the children were found never to attend school and this is 10% for fathers of the participants. Among the mothers, 24% were found to work outside the side and most of them are involved in unorganized sectors mainly as daily-based laborers. The majority of the fathers of the children under study were found to work and be involved in rickshaw pulling, daily labor, domestic servant, carpentry, mechanic/electrician and vendor, etc. More than fifty percent of the participants were from low socio-economic strata. More than 75% of the children claimed to receive exclusive breastfeeding (Table 1).
Regarding parental education as a determinant, more childhood obesity was found among those born to parents educated up to the primary level and the difference to illiterate mothers was significant. Regarding the occupation of the parents, the majority of the homemaker mothers’ children were overweight and obese. Out of 18 children who were not breastfed exclusively, 12(66.7%) were overweight and obese but it was not found to be statistically significant [not displayed].
Physical activity level (PAL) among both the older children as well as adolescents was Mean±SD 21.87±9.11. Only 17(22.7%) had PAL above the mean for the preceding seven days of data collection. Omnibus x2 at df 3 shows a significant P with the help of Epi info (version 7) in reference to non-obese. The table revealed that compared to the non-obese, those who were overweight and obese were 0.23 times (CL 0.11-0.46) more likely to have low physical activity levels. The difference was statistically significant (P<0.05). In the table stars are for reference values. (Table 2).
In the chi-square test, overweight and obesity were found to be more among male children, those belonging to low socio-economic status, and low physical activity levels, and these were found to be statistically significant (Table 3).
Children who were found overweight and obese, on in-depth interviewing were found to have preferences for street foods, junk foods, sweets and sugar, intake of food in-between meals, and beverages. Many of the parents of small children stated that they cannot keep sugar, milk powder, sweets, etc. within reach of the children. One of the working mothers told, “If I don’t bring either of the street foods while coming back home, my adolescent boy creates a huge mess evening beating his younger sister out of anger……”
Binary logistic regression revealed that a statistically significant association (P<0.05 between of childhood overweight and obesity were observed by birth weight (AOR 1.45, 95% CL 1.34-11.64), exclusive breastfeeding (AOR 3.12, 95% CL 2.75-12.42), high lipid profile (AOR 5.11, 95% CL 2.17-11.58), high liver function tests (AOR 3.40, 95% CL 1.49-12.86), high fasting blood sugar (AOR 5.02, 95% CL 1.34-16.56), low physical activity level (AOR 3.70, 95% CL 1.34-7.79), and high CIMT value (AOR 4.11, 95% CL 1.11-12.09); while male gender and high SES was not significant. The Hosmer and Lameshow test (x2= 9.278, df=4, P=0.934) proved the regression model fit of the data well. In the table stars are for reference values. (Table 4).
In the Kruskal-Wallis ANOVA test, the PAL score for non-obese showed a mean score of 39.93, for overweight 36.38, and obese children 33.71 and these were significant for overweight (P=0.04) and obesity (P=0.002) (Figure 1).
Discussion
Childhood obesity is a recognized precursor for various non-communicable diseases and related complications increasing overall disease burden and out-of-pocket expenditure at its present level and during adulthood. The majority of the nutrition-related national health programs are concentrated on undernutrition and people are still in belief of obesity as a sign of good health especially for children.
The proportion of children found to be overweight and obese in the current study area, itself being a non-privileged one is quite worrisome. A study conducted in Rajasthan by Jain et al. found nearly 40% of study children to be overweight and obese [9], a Telengana-based study revealed more than 2/3rd of the study participants to have weight far above the normal [19], and similar findings were obtained from a population-based study conducted in Pakistan [20]. These findings point toward the burden of childhood obesity in these developing nations too. The male preponderance of childhood overweight and obesity had similarities with a study conducted among primary school children in urban Nepal [21]. But a study from Delhi by Kaur, [22] in South Africa by Armstrong [23], Song from China [24], and Ahmed from Pakistan [25] showed female propensity of childhood obesity in their respective study areas. In contrast to the current study findings, parents with higher education, especially mothers were not protected in studies from urban Nepal [21], rural South India [4]. It can be presumed that among the study population higher education was responsible for awareness generation among parents. Mothers who were found as homemakers had more obese children in the present study; this might be because of the conventional belief of obesity as a marker of good health and proper child care. But these findings were not in accordance with other studies [21, 22]. The protective role of exclusive breastfeeding against obesity as found in the current study has supportive evidence from NFHS-III. One of the most alarming findings in the current study is that a higher proportion of children from low SES are overweight and obese which is somewhat similar to the study from Rajasthan [9] but evidence from urban Nepal was different [21]. There are dubious findings regarding this matter from different parts of the world [3, 8].
Regarding the physical activity level and types, in accordance with the current study, the protective role was established by studies by Jain [9] Prashanth et al. [26], Goyal et al. [27], and Keerthan et al. [28]. The pattern of physical activity level as found in the present study for the previous one week was also supported by Goyal et al. [27] and also from a study conducted in North India in 2009. A study conducted in urban Nepal [21] had no significant association in this regard contrary to others including the current study which may have been caused by mean rank on the non-parametric statistical tests. The CIMT measurement of the study was found to have supporting evidence from Baroncini et al. [13], Brady et al. [29], Mehta et al. [30] and from Maharashtra, India. As in logistic regression findings of the current study considering the effects of confounders, those showing significance in the univariate analysis except FBS and birth weight, being the researcher’s choices, the findings were corroborative to that form Karki [21], Azagba et al. [31].
Conclusion
Childhood obesity is on the rise and is the momentum to be the pandemic of the 21st century. In the study area with semi-urban background, the cross-section of the population showed alarming evidence for it. Factors showing a significant positive impact on it like exclusive breastfeeding, lipid profile, blood sugar level, liver function tests, physical activity level, and carotid intima-media thickness are modifiable risk factors and hence the definite role of primordial and primary preventive measures can be taken for their control.
Limitations
This study was conducted on a pilot basis and hence the studied population was low in number. Dietary history in detail was not taken into account. A future prospective study preferably with a mixed-methods approach with non-participant observation for especially dietary and lifestyle factors to explore in-depth and follow-up of CIMT for the development of non-communicable diseases and providing interventions is recommended.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted with approval of Jagannath Gupta Institute of Medical Sciences and Hospital. Informed consent was obtained from the legal guardians (father-mother) of each patient (younger children) included in the study
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors contributions
All authors equally contributed to preparing this article.
Conflicts of interest
The authors declared no conflicts of interest.
Acknowledgements
The authors are very grateful to all hospital authorities for their permission to conduct this study and for all kinds of cooperation.
References
- World Health Organization. Obesity and overweight, Fact sheet No. 311. Geneva: WHO; 2014. [Link]
- Park K. Park’s Textbook of Preventive and Social Medicine. Madhya Pradesh: Banarasidas Bhanot; 2017. [Link]
- Arteaga SS, Esposito L, Osganian SK, Pratt CA, Reedy J, Young-Hyman D. Childhood obesity research at the NIH: Efforts, gaps, and opportunities. Transl Behav Med. 2018; 8(6):962-7. [DOI:10.1093/tbm/iby090] [PMID] [PMCID]
- Jagadesan S, Harish R, Miranda P, Unnikrishnan R, Anjana RM, Mohan V. Prevalence of overweight and obesity among school children and adolescents in Chennai. Indian Pediatr. 2014; 51(7):544-9. [DOI:10.1007/s13312-014-0444-6] [PMID]
- Chakraborty P, Dey S, Pal R, Kar S, Zaman FA, Pal S. Obesity in Kolkata children: Magnitude in relationship to hypertension. J Natural Sci Bio Med. 2011; 2(1):101-6. [PMID] [PMCID]
- Shah B, Anand K, Joshi P, Mahanta J, Mohan V, Thankappan K. Report of the Surveillance of Risk Factors of Non-communicable Diseases (STEPS 1 and 2) from five centers in India - WHO India - ICMR initiative. New Delhi: WHO India; 2004. [Link]
- Centers for Disease Control and Prevention. National health and nutrition examination survey 2015-2016. [Internet]. 2017 [Updated 2017 October 13]. Available from: [Link]
- Reddy SP, Resnicow K, James S, Kambaran N, Omardien R, Mbewu AD. Underweight, overweight and obesity among South African adolescents: Results of the 2002 National Youth Risk Behaviour Survey. Public Health Nutr. 2008; 12(2):203-7. [DOI:10.1017/S1368980008002656] [PMID]
- Jain A, Jain A, Pankaj JP, Sharma BN, Paliwal A. The study of obesity among children aged 5-18 years in Jaipur, Rajasthan. Muller J Med Sci Res. 2016; 7(2):123-30. [DOI:10.4103/0975-9727.185013]
- World Health Organization. Population-based approaches to childhood obesity prevention. Geneva: WHO; 2012. [Link]
- Agho KE, Dibley MJ, Odiase JI, Ogbonmwan SM. Determinants of exclusive breastfeeding in Nigeria. BMC Pregnancy Childbirth. 2011; 11:2. [DOI:10.1186/1471-2393-11-2] [PMID] [PMCID]
- Tan KL. Factors associated with exclusive breastfeeding among infants under six months of age in peninsular Malaysia. Int Breastfeed J. 2011; 6(1):2. [DOI:10.1186/1746-4358-6-2] [PMID] [PMCID]
- Baroncini LA, Sylvestre Lde C, Pecoits Filho R. Assessment of intima-media thickness in healthy children aged 1 to 15 years. Arq Bras Cardiol. 2016; 106(4):327-32. [DOI:10.5935/abc.20160030] [PMID] [PMCID]
- Baroncini LAV, Sylvestre LC, Baroncini CV, Pecoits R Filho. Assessment of carotid intima-media thickness as an early marker of vascular damage in hypertensive children. Arq Bras Cardiol. 2017; 108(5):452-7. [DOI:10.5935/abc.20170043] [PMID] [PMCID]
- Ravani A, Werba JP, Frigerio B, Sansaro D, Amato M, Tremoli E, et al. Assessment and relevance of Carotid Intima-Media Thickness (C-IMT) in primary and secondary cardiovascular prevention. Curr Pharm Des. 2015; 21( 9):1164-71. [DOI:10.2174/1381612820666141013121545] [PMID] [PMCID]
- Ranjani H, Mehreen TS, Pradeepa R, Anjana RM, Garg R, Anand K, et al. Epidemiology of childhood overweight & obesity in India: A systematic review. Indian J Med Res. 2016; 143(2):160-74. [PMID] [PMCID]
- Biswas T, Islam A, Islam MS, Pervin S, Rawal LB. Overweight and obesity among children and adolescents in Bangladesh: A systematic review and meta-analysis. Public Health. 2017; 142:94-101. [DOI:10.1016/j.puhe.2016.10.010] [PMID]
- Kowalski KC, Crocker PRE, Donen RM. The Physical Activity Questionnaire for Older Children (PAQ-C) and Adolescents (PAQ-A) Manual. Saskatoon: University of Saskatchewan; 2004. [Link]
- Chandra N, Anne B, Venkatesh K, Teja GD, Katkam SK. Prevalence of childhood obesity in an Affluent School in Telangana using the recent IAP growth chart: A pilot study. Indian J Endocrinol Metab. 2019; 23(4):428-32. [DOI:10.4103/ijem.IJEM_151_19] [PMID] [PMCID]
- Tanzil S, Jamali T. Obesity, an emerging epidemic in Pakistan: A review of evidence. J Ayub Med Coll Abbottabad. 2016; 28(3):597. [Link]
- Karki A, Sreashtha A, Subedi N. Prevalence and associated factors of childhood overweight/obesity among primary school children in urban Nepal. BMC Public Health. 2019; 19(1):1055. [DOI:10.1186/s12889-019-7406-9] [PMID] [PMCID]
- Kaur S, Kapil U, Singh P. Pattern of chronic diseases amongst adolescent obese children in developing countries. Curr Sci. 2005; 88(7):1052-6. [Link]
- Armstrong ME, Lambert MI, Sharwood KA, Lambert EV. Obesity and overweight in South African primary school children: The Health of the Nation Study. S Afr Med J. 2006; 96(5):439-44. [DOI:10.1080/22201009.2006.10872144] [PMID]
- Song Y, Wang H, Ma J, Wang Z. Secular trends of obesity prevalence in urban Chinese children from 1985 to 2010: Gender disparity. Plos One. 2013; 8(1):e53069. [DOI:10.1371/journal.pone.0053069] [PMID] [PMCID]
- Ahmed J, Laghari A, Naseer M, Mehraj V. Prevalence of and factors associated with obesity among Pakistani schoolchildren: A school-based, cross-sectional study. East Mediterr Health J. 2013; 19(3):242-7. [DOI:10.26719/2013.19.3.242] [PMID]
- Prashanth K, Baby KE, Rao KR, Kumarkrishna B, Hegde K, Kumar M, et al. Prevalence of obesity among high school children in Dakshina Kannada and Udupi districts. J Health Allied Sci. 2011; 1:16-20. [DOI:10.1055/s-0040-1703533]
- Goyal JP, Kumar N, Parmar I, Shah VB, Patel B. Determinants of overweight and obesity in affluent adolescent in Surat City, South Gujarat Region, India. Indian J Community Med. 2011; 36(4):296-300. [PMID] [PMCID]
- Keerthan Kumar M, Prashanth K, Baby KE, Rao KR, Kumarkrishna B, Hegde K, et al. Prevalence of obesity among high school children Dakshina Kannada and Udupi District. Nitte Univ J Heal Sci. 2011; 4:16-20. [Link]
- Brady TM, Schneider MF, Flynn JT, Cox C, Samuels J, Saland J, et al. Carotid intima-media thickness in children with CKD: Results From the CKiD study. Clin J Am Soc Nephrol. 2012; 7(12):1930-7. [DOI:10.2215/CJN.03130312] [PMID] [PMCID]
- Mehta A, Mishra S, Ahmad K, Tiwari HC, Singh V, Singh A. Carotid intima media thickness in children with nephrotic syndrome: An observational case-control study. Sudan J Paediatr. 2019; 19(2):110-6. [DOI:10.24911/SJP.106-1535804613] [PMID] [PMCID]
- Azagba S, Sharaf MF. Fruit and vegetable consumption and body mass index: A quantile regression approach. J Prim Care Community Health. 2012; 3(3):210-20. [DOI:10.1177/2150131911434206] [PMID]
Type of Study: Original Article |
Subject:
Pediatrics
Received: 2022/02/10 | Accepted: 2022/05/9 | Published: 2023/04/1
Received: 2022/02/10 | Accepted: 2022/05/9 | Published: 2023/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Articles Copyright © The Author(s).
Owned by Mazandaran University of Medical Sciences.
Published by Negah Institute for Scientific Communication.
Journal of Pediatrics Review (JPR)
Bou Ali Sina Hospital, Pasdaran Boulevard, Sari, Iran.
Journal Tel: +98 - 1133342331
Publisher Tel: +9821 8603 6497-
+9821 8603 7228 (EXT: 104)
Website: http://jpr.mazums.ac.ir/
E-mail: jpr.mazums@gmail.com,
jpr@mazums.ac.ir
