
Mon, Jul 13, 2026


Volume 14, Issue 2 (April 2026)
J. Pediatr. Rev 2026, 14(2): 207-212 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Saleh F, Karimi Rouzbahani A, Naghmehsanj Z, Molavi M A. Isolated Unilateral Orbital Myeloid Sarcoma (an Isolated Extra Medullary Myeloid Leukemia): A Case Report. J. Pediatr. Rev 2026; 14 (2) :207-212
URL: http://jpr.mazums.ac.ir/article-1-623-en.html
URL: http://jpr.mazums.ac.ir/article-1-623-en.html



1- Department of Pediatric Hematology Oncology, Children’s Clinical Research Development Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran.
2- Department of Urology, Western Health, Melbourne, Australia. & Surgery Education and Researching Network (SERGN), Universal Scientific Education and Research Network (USERN), Khorramabad, Iran.
3- Department of Pediatrics, Pediatric Hospital, Bandar Abbas, Iran
4- Department of Pediatric Hematology Oncology, Children’s Clinical Research Development Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran ,shayanmolavi@yahoo.com
2- Department of Urology, Western Health, Melbourne, Australia. & Surgery Education and Researching Network (SERGN), Universal Scientific Education and Research Network (USERN), Khorramabad, Iran.
3- Department of Pediatrics, Pediatric Hospital, Bandar Abbas, Iran
4- Department of Pediatric Hematology Oncology, Children’s Clinical Research Development Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran ,
Full-Text [PDF 2137 kb]
(109 Downloads)
| Abstract (HTML) (233 Views)
Full-Text: (43 Views)
Introduction
Isolated extramedullary leukemia is a rare condition that can appear in various tissues, with or without involvement of the bone marrow. Two key subtypes of extramedullary leukemia are myeloid sarcoma (MS) and leukemia cutis (LC). MS, sometimes called chloroma, is identified pathologically as an extramedullary collection of blast cells that disrupts the typical architecture of tissues. It is also referred to as granulocytic sarcoma or extramedullary myeloid tumor. MS is strongly associated with chronic myeloid leukemia (CML), acute myeloid leukemia (AML), and myelodysplastic syndromes (MDS) [1, 2].
Isolated MS, characterized by no prior history of leukemia, MDS, or myeloproliferative neoplasms and a negative bone marrow biopsy, has been documented in a few case reports [3]. Up to 46% of these patients are frequently misdiagnosed as having lymphoma, most commonly non-Hodgkin lymphoma [4, 5]. MS may also manifest during relapse, with or without bone marrow involvement. The differential diagnosis for MS includes non-Hodgkin lymphoma, Ewing sarcoma, lymphoblastic leukemia, melanoma, blastic plasmacytoid dendritic cell neoplasm, and extramedullary hematopoiesis [6].
We herein introduce a child from Islamic Republic of Iran, with infiltration of myeloid blasts in the left eye as an isolated presentation of AML.
Case Presentation
History: Our patient was a 13-year-old boy from Minab-Bandar Abbas- Iran with normal growth indexes, who had been well until seven days before admission, when he developed a painless, slowly progressive left orbital proptosis.
Clinical examination: On physical examination, no nystagmus, blurred vision or eye deviation was detected, and the patient had no fever or pain. All cranial nerves were normal and there was no pallor, petechiae, ecchymosis or any hematologic findings. Abdominal examination was normal without mass or organomegaly.
Oral clinical, radiological, and histopathological examination: In orbital computed tomography (CT) scan, a left orbital mass was documented, which measured 3×2×1.5 cm (Figure 1).
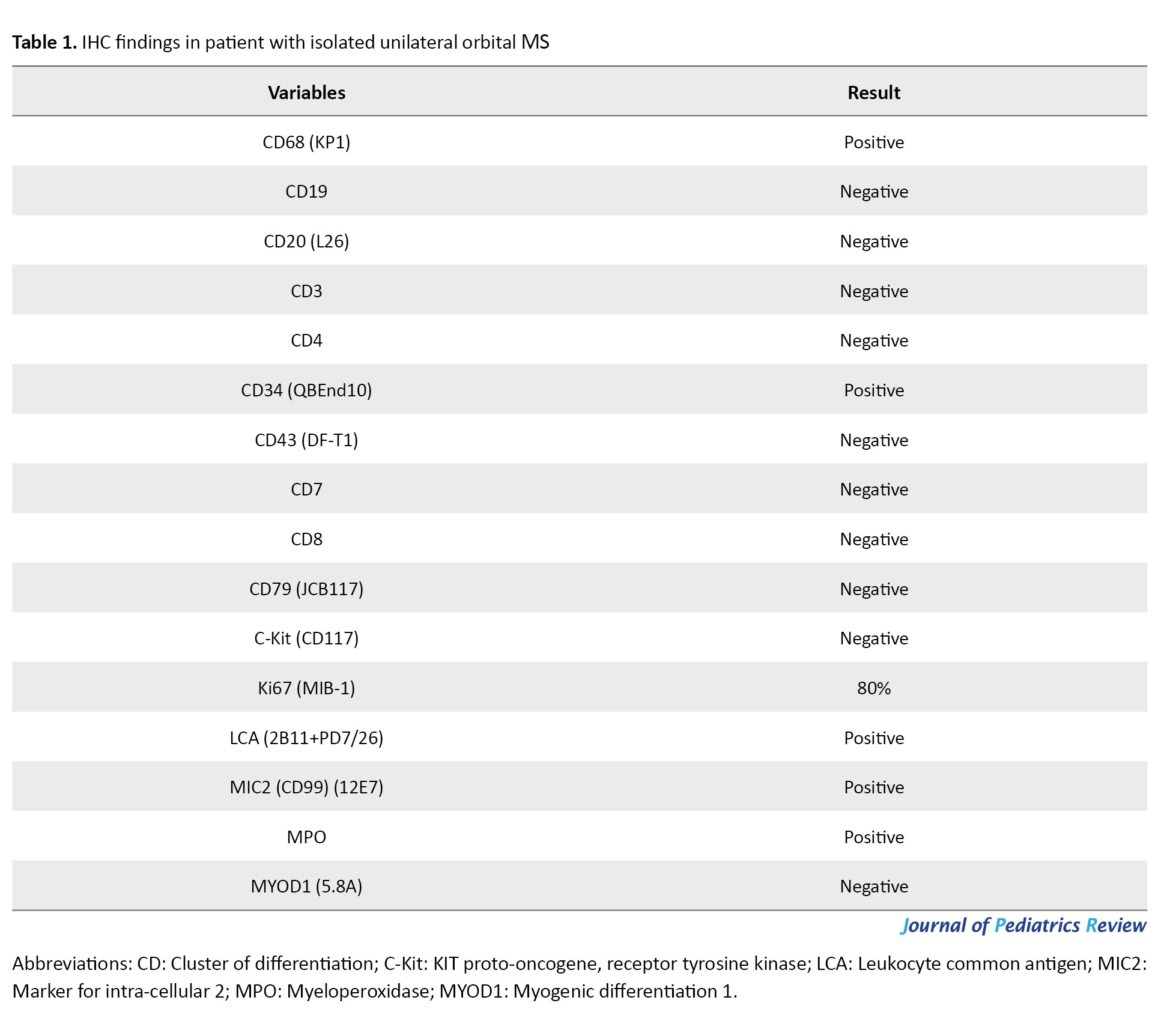
 A biopsy of the orbital mass was performed by an ophthalmologist, and histologic study showed a diffuse infiltrative population of malignant cells. Usually, the cancerous cells had enlarged nuclei and abundant cytoplasm, and were suspected myeloblasts; therefore, the tissue sample was sent for immunohistochemistry (IHC). The detailed immunohistochemical findings are presented in Table 1.
A biopsy of the orbital mass was performed by an ophthalmologist, and histologic study showed a diffuse infiltrative population of malignant cells. Usually, the cancerous cells had enlarged nuclei and abundant cytoplasm, and were suspected myeloblasts; therefore, the tissue sample was sent for immunohistochemistry (IHC). The detailed immunohistochemical findings are presented in Table 1.
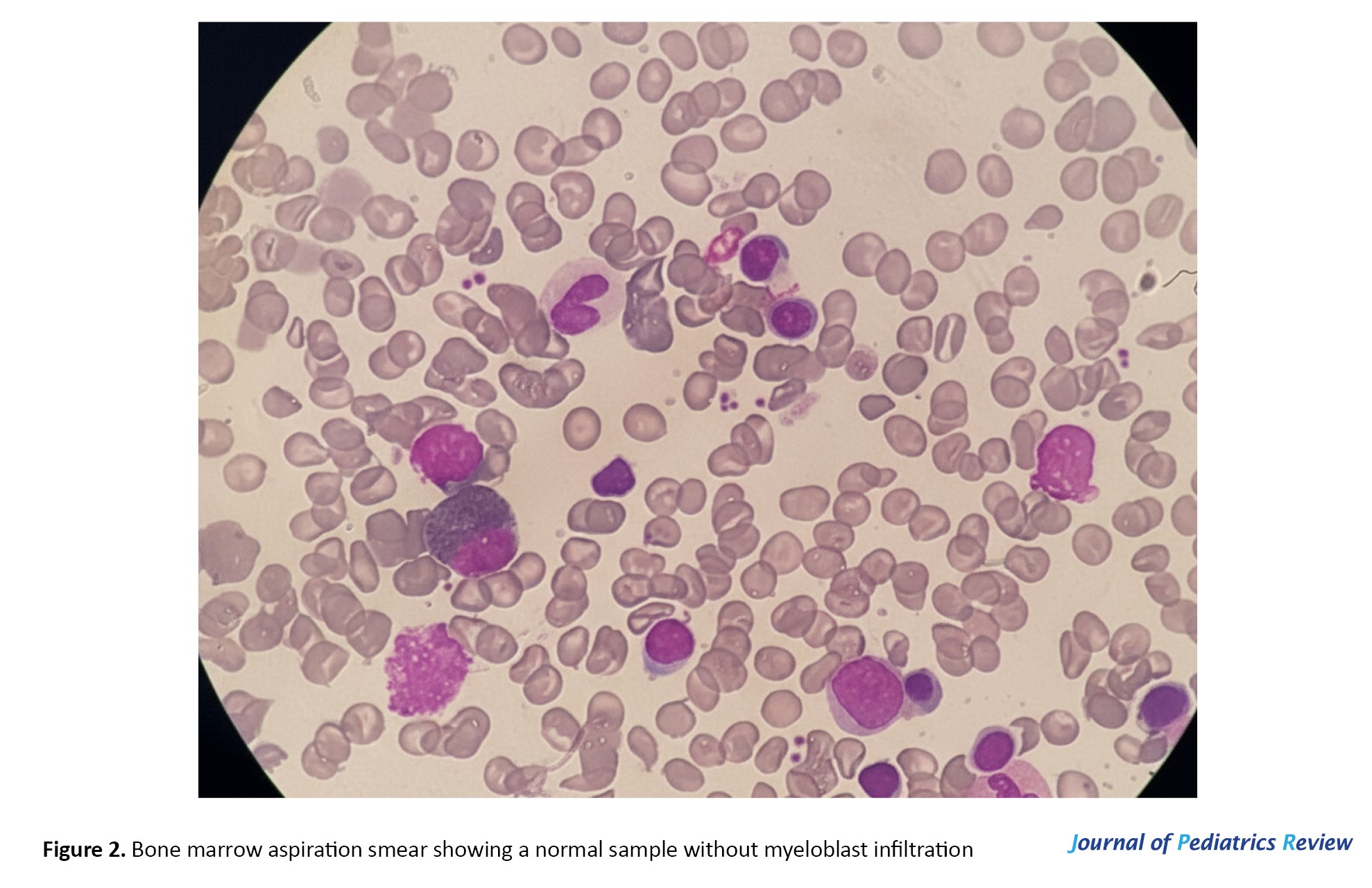
IHC confirmed blasts infiltration, and MS was diagnosed. Cerebral spinal fluid cytology was blast-free, and none marrow aspiration showed no infiltration or dysplastic findings (Figure 2).
 The patient underwent chemotherapy (BFM98), and received one year of maintenance treatment (cytarabine and thioguanine). In the last two years after completing treatment, the patient was remained under periodic follow-up with no specific complications or recurrence of the disease.
The patient underwent chemotherapy (BFM98), and received one year of maintenance treatment (cytarabine and thioguanine). In the last two years after completing treatment, the patient was remained under periodic follow-up with no specific complications or recurrence of the disease.
Discussion
Compared to older children and adults, newborns are more likely to have MS. Typically myeloperoxidase (MPO)-positive or cluster of differentiation (CD)163-positive, the blast cells display CD33, CD13, and CD117. For lesions with monocytic differentiation, they may also express CD14, CD11C, and CD68. AML with mixed‑lineage leukemia (MLL) rearrangement, as well as those with nucleophosmin 1 (NPM1) mutations are associated with the presence of MS [7]. Approximately 10% of children with AML have MS. The skin and orbit are the most frequently affected areas in children. Additional typical sites of involvement include the gastrointestinal tract, bone, lymph nodes, and central nervous system [8].
In this study, the tumor tissue exhibited positive staining for MPO and CD68, which are commonly recognized markers of myeloid differentiation, highlighting the significant value of IHC in identifying antigens linked to the myeloid lineage, including CD13, CD33, CD43, CD117, MPO, and CD68 [9-11]. IHC analysis of myeloid antigen expression (CD68, MPO and/or lysozyme) in undifferentiated neoplasms and high-grade non-Hodgkin lymphomas serves as an essential method for excluding MS, given the overlapping characteristics between MS and high-grade lymphomas.
Specific genetic alterations may be associated with different sites of involvement. The Runt‑related transcription factor 1-RUNX1 translocation partner 1 (RUNX1-RUNX1T1) fusions are common in paediatric MS and frequently involve the orbit [12]. The lysine methyltransferase 2A (KMT2A) translocation is often associated with cutaneous localization, and myosin heavy chain 11-core‑binding factor subunit beta (MYH11-CBFB) is associated with MS located in the intestine [13].
There is limited extensive research examining prognostic variables in MS patients because of its rarity. However, individuals who present with isolated MS appear to have a different prognosis than those who present simultaneously with or at an AML relapse. It was once thought that a leukemic patient’s diagnosis of MS was a sign of a poor clinical result and a shorter survival time [14]. 92 patients who presented with either MS alone or MS with a concomitant myeloid tumor were examined by Pileri and associates. They found that the patients’ clinical presentation (isolated MS, MS concurrent with or after AML), age, gender, and anatomic location), morphological classification, immunophenotype, and cytogenetic findings had no bearing on the course of the disease or the response to treatment [15]. In several investigations, the management of isolated orbital MS via systemic chemotherapy yielded positive survival rates [13, 14].
There is no demonstrated role for radiation in conjunction with systemic chemotherapy. When comparing MS patients (alone or after receiving an AML diagnosis) treated with radiation therapy in addition to chemotherapy to those treated with chemotherapy alone, Lan and colleagues observed no difference in survival (P=0.56) [14]. Only chemotherapy, akin to that used for AML without radiotherapy, is employed in our practice.
Conclusion
Compared to AML patients with or without MS, people with isolated MS receiving AML‑type chemotherapy may have a better prognosis.
Ethical Considerations
Compliance with ethical guidelines
Written informed consent was obtained from the patient’s parents/legal guardians for publication of this case report and any accompanying images. Ethical principles were observed in accordance with the Declaration of Helsinki.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, inter-ception of the results and drafting of the manuscript. Each author approved the final version of the manu-script for submission.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank all those who contributed to the patient’s care.
References
Isolated extramedullary leukemia is a rare condition that can appear in various tissues, with or without involvement of the bone marrow. Two key subtypes of extramedullary leukemia are myeloid sarcoma (MS) and leukemia cutis (LC). MS, sometimes called chloroma, is identified pathologically as an extramedullary collection of blast cells that disrupts the typical architecture of tissues. It is also referred to as granulocytic sarcoma or extramedullary myeloid tumor. MS is strongly associated with chronic myeloid leukemia (CML), acute myeloid leukemia (AML), and myelodysplastic syndromes (MDS) [1, 2].
Isolated MS, characterized by no prior history of leukemia, MDS, or myeloproliferative neoplasms and a negative bone marrow biopsy, has been documented in a few case reports [3]. Up to 46% of these patients are frequently misdiagnosed as having lymphoma, most commonly non-Hodgkin lymphoma [4, 5]. MS may also manifest during relapse, with or without bone marrow involvement. The differential diagnosis for MS includes non-Hodgkin lymphoma, Ewing sarcoma, lymphoblastic leukemia, melanoma, blastic plasmacytoid dendritic cell neoplasm, and extramedullary hematopoiesis [6].
We herein introduce a child from Islamic Republic of Iran, with infiltration of myeloid blasts in the left eye as an isolated presentation of AML.
Case Presentation
History: Our patient was a 13-year-old boy from Minab-Bandar Abbas- Iran with normal growth indexes, who had been well until seven days before admission, when he developed a painless, slowly progressive left orbital proptosis.
Clinical examination: On physical examination, no nystagmus, blurred vision or eye deviation was detected, and the patient had no fever or pain. All cranial nerves were normal and there was no pallor, petechiae, ecchymosis or any hematologic findings. Abdominal examination was normal without mass or organomegaly.
Oral clinical, radiological, and histopathological examination: In orbital computed tomography (CT) scan, a left orbital mass was documented, which measured 3×2×1.5 cm (Figure 1).
IHC confirmed blasts infiltration, and MS was diagnosed. Cerebral spinal fluid cytology was blast-free, and none marrow aspiration showed no infiltration or dysplastic findings (Figure 2).
Discussion
Compared to older children and adults, newborns are more likely to have MS. Typically myeloperoxidase (MPO)-positive or cluster of differentiation (CD)163-positive, the blast cells display CD33, CD13, and CD117. For lesions with monocytic differentiation, they may also express CD14, CD11C, and CD68. AML with mixed‑lineage leukemia (MLL) rearrangement, as well as those with nucleophosmin 1 (NPM1) mutations are associated with the presence of MS [7]. Approximately 10% of children with AML have MS. The skin and orbit are the most frequently affected areas in children. Additional typical sites of involvement include the gastrointestinal tract, bone, lymph nodes, and central nervous system [8].
In this study, the tumor tissue exhibited positive staining for MPO and CD68, which are commonly recognized markers of myeloid differentiation, highlighting the significant value of IHC in identifying antigens linked to the myeloid lineage, including CD13, CD33, CD43, CD117, MPO, and CD68 [9-11]. IHC analysis of myeloid antigen expression (CD68, MPO and/or lysozyme) in undifferentiated neoplasms and high-grade non-Hodgkin lymphomas serves as an essential method for excluding MS, given the overlapping characteristics between MS and high-grade lymphomas.
Specific genetic alterations may be associated with different sites of involvement. The Runt‑related transcription factor 1-RUNX1 translocation partner 1 (RUNX1-RUNX1T1) fusions are common in paediatric MS and frequently involve the orbit [12]. The lysine methyltransferase 2A (KMT2A) translocation is often associated with cutaneous localization, and myosin heavy chain 11-core‑binding factor subunit beta (MYH11-CBFB) is associated with MS located in the intestine [13].
There is limited extensive research examining prognostic variables in MS patients because of its rarity. However, individuals who present with isolated MS appear to have a different prognosis than those who present simultaneously with or at an AML relapse. It was once thought that a leukemic patient’s diagnosis of MS was a sign of a poor clinical result and a shorter survival time [14]. 92 patients who presented with either MS alone or MS with a concomitant myeloid tumor were examined by Pileri and associates. They found that the patients’ clinical presentation (isolated MS, MS concurrent with or after AML), age, gender, and anatomic location), morphological classification, immunophenotype, and cytogenetic findings had no bearing on the course of the disease or the response to treatment [15]. In several investigations, the management of isolated orbital MS via systemic chemotherapy yielded positive survival rates [13, 14].
There is no demonstrated role for radiation in conjunction with systemic chemotherapy. When comparing MS patients (alone or after receiving an AML diagnosis) treated with radiation therapy in addition to chemotherapy to those treated with chemotherapy alone, Lan and colleagues observed no difference in survival (P=0.56) [14]. Only chemotherapy, akin to that used for AML without radiotherapy, is employed in our practice.
Conclusion
Compared to AML patients with or without MS, people with isolated MS receiving AML‑type chemotherapy may have a better prognosis.
Ethical Considerations
Compliance with ethical guidelines
Written informed consent was obtained from the patient’s parents/legal guardians for publication of this case report and any accompanying images. Ethical principles were observed in accordance with the Declaration of Helsinki.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, inter-ception of the results and drafting of the manuscript. Each author approved the final version of the manu-script for submission.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank all those who contributed to the patient’s care.
References
- Roth MJ, Medeiros LJ, Elenitoba-Johnson K, Kuchnio M, Jaffe ES, Stetler-Stevenson M. Extramedullary myeloid cell tumors. An immunohistochemical study of 29 cases using routinely fixed and processed paraffin-embedded tissue sections. Arch Pathol Lab Med. 1995; 119(9):790-8. [PMID]
- Molavi M A, Tahmasebi Ghorabi S, Saleh F, Nazemi Qeshmi A, Mazloumi S S, Mahmoudi M et al. Incidence rate of various types of leukemia in children at Bandar Abbas children’s hospital: A brief report of half a decade. CJP 2024; 10 (1):e1. [DOI: 10.22088/CJP.BUMS.10.1.14]
- Eshghabadi M, Shojania AM, Carr I. Isolated granulocytic sarcoma: report of a case and review of the literature. J Clin Oncol. 1986; 4(6):912-7. [DOI:10.1200/JCO.1986.4.6.912] [PMID]
- Meis JM, Butler JJ, Osborne BM, Manning JT. Granulocytic sarcoma in nonleukemic patients. Cancer. 1986; 58(12):2697-709. [DOI:10.1002/1097-0142(19861215)58:123.0.CO;2-R] [PMID]
- Byrd JC, Edenfield WJ, Shields DJ, Dawson NA. Extramedullary myeloid cell tumors in acute nonlymphocytic leukemia: a clinical review. J Clin Oncol. 1995; 13(7):1800-16.[DOI:10.1200/JCO.1995.13.7.1800] [PMID]
- Audouin J, Comperat E, Le Tourneau A, Camilleri-Broët S, Adida C, Molina T, et al. Myeloid sarcoma: clinical and morphologic criteria useful for diagnosis. Int J Surg Pathol. 2003; 11(4):271-82. [DOI:10.1177/10668969030110040] [PMID]
- Aplenc R, Elgarten CW, Choi JK, Meshinchi S. Acute myeloid leukemia and myelodysplastic syndromes. In: Blaney SM, Adamson PC, Helman LJ, editors. Pizzo & Poplack's Pediatric oncology. 8th ed. Philadelphia: Wolters Kluwer; 2021.
- Kobayashi R, Tawa A, Hanada R, Horibe K, Tsuchida M, Tsukimoto I, et al. Extramedullary infiltration at diagnosis and prognosis in children with acute myelogenous leukemia. Pediatr Blood Cancer. 2007; 48(4):393-8. [DOI:10.1002/pbc.20824] [PMID]
- Campidelli C, Agostinelli C, Stitson R, Pileri SA. Myeloid sarcom: Extramedullary manifestation of myeloid disorders. Am J Clin Pathol. 2009; 132(3):426-37. [DOI:10.1309/AJCP1ZA7HYZKAZHS] [PMID]
- Bakst RL, Tallman MS, Douer D, Yahalom J. How I treat extramedullary acute myeloid leukemia. Blood. 2011; 118(14):3785-93. [DOI:10.1182/blood-2011-04-347229] [PMID]
- Rocha Filho FD, Ferreira FV, Lima GG, Lima MG, Figueiredo AA. Apresentação incomum de sarcoma granulocítico mamário. Rev Bras Hematol Hemoter. 2009; 31(4):295-8. [DOI:10.1590/S1516-84842009005000063]
- Wilson CS, Medeiros LJ. Extramedullary manifestation of myeloid neoplasms. Am J Clin Pathol. 2015; 144(2):219-39. [DOI:10.1309/AJCPO58YWIBUBESX] [PMID]
- Johnston DL, Alonzo TA, Gerbing RB, Lange BJ, Woods WG. Superior outcome of pediatric acute myeloid leukemia patients with orbital and CNS myeloid sarcoma: A report from the children's oncology group. Pediatr Blood Cancer. 2012; 58(4):519-24. [DOI:10.1002/pbc.23201] [PMID]
- Lan TY, Lin DT, Tien HF, Yang RS, Chen CY, Wu K. Prognostic factors of treatment outcomes in patients with granulocytic sarcoma. Acta Haematol. 2009; 122(4):238-46.[DOI:10.1159/000253592] [PMID]
- Pileri SA, Ascani S, Cox MC, Campidelli C, Bacci F, Piccioli M, et al. Myeloid sarcoma: Clinico-pathologic, phenotypic and cytogenetic analysis of 92 adult patients. Leukemia. 2007; 21(2):340-50. [DOI:10.1038/sj.leu.2404491] [PMID]
Type of Study: Case Report and Review of Literature |
Subject:
Pediatrics
Received: 2024/04/20 | Accepted: 2025/12/7 | Published: 2026/04/3
Received: 2024/04/20 | Accepted: 2025/12/7 | Published: 2026/04/3
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
