
Tue, Aug 11, 2026


Volume 8, Issue 2 (4-2020)
J. Pediatr. Rev 2020, 8(2): 107-120 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Barimani Aboksari Z, Ganji J, Mousavinasab N, Rezaei M, Khani S. A Review Study on Educational Interventions Promoting Sexual Health of Children Under 12 Years. J. Pediatr. Rev 2020; 8 (2) :107-120
URL: http://jpr.mazums.ac.ir/article-1-244-en.html
URL: http://jpr.mazums.ac.ir/article-1-244-en.html



1- Student Research Committee, School of Nursing and Midwifery, Mazandaran University of Medical Sciences, Sari, Iran.
2- Sexual and Reproductive Health Research Center, Mazandaran University of Medical Sciences, Sari, Iran.
3- Health Sciences Research Center, School of Health, Mazandaran University of Medical Sciences, Sari, Iran.
4- Department of Midwifery, Gorgan Branch, Islamic Azad University, Gorgan, Iran.
5- Sexual and Reproductive Health Research Center, Mazandaran University of Medical Sciences, Sari, Iran. ,s.khani@mazums.ac.ir
2- Sexual and Reproductive Health Research Center, Mazandaran University of Medical Sciences, Sari, Iran.
3- Health Sciences Research Center, School of Health, Mazandaran University of Medical Sciences, Sari, Iran.
4- Department of Midwifery, Gorgan Branch, Islamic Azad University, Gorgan, Iran.
5- Sexual and Reproductive Health Research Center, Mazandaran University of Medical Sciences, Sari, Iran. ,
Full-Text [PDF 481 kb]
(3910 Downloads)
| Abstract (HTML) (9077 Views)




Full-Text: (5265 Views)
1. Context
Sexual health is based on people’s knowledge; physical, and mental health; economic status; and social values. However, one’s knowledge, which can be achieved by sexual training, plays the most crucial role in approaching an appropriate level of sexual health (1). Sexual training consists of instructing knowledge of reproduction, sexual issues, and attitude towards it and may be performed at schools or some other educational settings (2).
Sexual health issue comprises both genders at all age groups. However, sexual health and its importance can be defined differently in various periods of life. For instance, sexual health in children means providing a safe environment for normal sexual growth and preventing sexual abuse (1). Although sexual incentive and behavior are instinctive, it is affected by environmental factors if not guided and appropriately trained. This defect may lead to some problems and threaten the mental and physical health of the person. Therefore, parents and teachers should provide their children and students with sexual knowledge as they are growing up. Sexual training along with teaching the values, norms, and controlling skills, result in the prevention of early, High risk, and unprotected sexual activities and guarantees the individual’s health in the present and future (2-4).
Sexual education is not taught to most of the children, and this ignorance may adversely affect different dimensions of one’s sexual health. Girls may receive some information about menstruation from their mothers, while boys do not receive similar guides. Talking to children about this issue constantly but briefly can have positive effects on their relationships and sexual health (5). It should be emphasized that if children and teenagers cannot receive appropriate answers to their questions, they may refer to their peers and improper sources. Therefore, providing them with proper information and giving adequate answers to their questions is of great importance (6). Children’s knowledge about sexual issues plays a decisive role in their development, general and sexual health, and reproduction. Thus, it is necessary to provide them with sexual information. Sexual education should be considered as an individual’s right to education (7, 8).
Few people all over the world receive the necessary preparations, such as decision-making skills, refusal skills, body safety rules, and sexual abuse prevention for their sexual life. This lack of knowledge makes them vulnerable to rape, sexual abuse, unwanted pregnancy, and sexually transmitted diseases (9, 10). Child Sexual Abuse (CSA) puts children in an embarrassing situation, bringing about short-term and long-term consequences such as fear, isolation, aggression, low self-esteem, embarrassment, inappropriate sexual behaviors, depression, and suicide. Moreover, sexual abuse experience in childhood is associated with negative body image and sexual dysfunction in adulthood (11). Hence, children need care, supervision, and training throughout their sexual development (12).
Both family and school are responsible for sexual training, but a review of literature has shown that most often, the consequences are not satisfactory (7). Primary school teachers are the key service providers for sexual training to children, families, and society. However, they are worried about the parents’ attitude towards such training programs and class management considering the children’s puberty stage, knowledge, and comfort. Thus, the teachers’ relationship with parents should be encouraged, and they must receive training about children’s sexual health (13). Parents and caregivers, as the primary educators, can play an essential role in protecting children’s sexual health (14, 15). However, their efforts can be compromised by insufficient knowledge, lack of skills, and comfort (16). Formal sexual instruction at schools consisting of sexual decision-making skills and Sexually Transmitted Infection (STI) prevention can promote adolescence and youth health conditions (10). The study conducted by Gong J et al. revealed that HIV/AIDS prevention programs based on protection motivation theory (PMT-based instruction) for children and their parents had positive effects on their HIV/AIDS knowledge, sexual perception, and condom use intention (17). Martin J et al. found out that sexual instruction to the mothers of preschool children increased their knowledge and attitude score (18).
Similarly, other studies demonstrated that instructing parents in children’s sexual health affects their knowledge, performance, and self-efficacy (19, 20). Some of the sexual health interventions may decrease other unwanted health consequences such as substance abuse or behavioral disorders. Some other interventions appear to be useful, though less effective in families and children with serious problems (18). Review studies conducted on sexual health have not focused on educational intervention for children under 12 (7, 12, 21, 22). Therefore, this study aimed at reviewing different types of educational interventions related to the sexual health of children under 12 years. We hope to recognize the interventions promoting the children’s sexual health.
2. Evidence Acquisition
In this narrative review, Google Scholar, PubMed, Scopus, Science Direct, and Web of Science databases were searched using the following keywords: “sex education", “sexual education", “sexual health", “sexual training and children". Two researchers (Zahra Barimani Aboksari and Maedeh Rezaei) searched articles related to children’s sexual health up to December 2018. Articles were included based on the subject of the study (sexual health of children under 12), study design (experimental, quasi-experimental, before-after studies), and consequences of the intervention (children’s sexual health). Irrelevant studies were excluded from the review process. Data extraction was done by two researchers (Zahra Barimani Aboksari and Maedeh Rezaei).
3. Results
The relevant articles were categorized into 4 groups:
1. Children-focused interventions; 2. Parent-focused interventions; 3. Children- and parent-focused interventions; 4. The impact of culture and religion.
Those studies conducted on children were 5 articles (23-27), those done on parents included 7 articles (18-20, 28-31), and 4 studies had been conducted on both (17, 32-34). Among the 16 articles, 5 were conducted in Iran, 4 in the USA, 4 in Korea, 2 in the Bahamas, and one in England.
Children-focused interventions
Studies on 8- to 12-year-old children had investigated peer-led sex education (26), sexual abuse prevention training and appropriate touch (23, 24), body image (25), and decrease in gender-type remarks (27). These studies were carried out from 2004 to 2018 (Table 1).
Sexuality education coaching program
One study had investigated peer-led sexuality education. The children were 11 to 12 years old, and the syllabus consisted of sexual knowledge (sexual differentiation, pornography, and communication) and sexual attitude (sexual concept, relationship, physical development, sexual-psychological development, sexual health, the value of life, and sexual violence). It was taught to 21 fifth- and sixth-grade students in primary school during 10 sessions. Instruments such as activity paper, proverb card, vulgar belief card, worrying box, video, sonogram, children’s storybook, embryo album activity paper, task, sentence card, and textbook were used. The results of this study indicated that peer-led sexual education promoted sexual knowledge and attitude in children (26).
Preventing sexual abuse
Two articles worked on sexual abuse prevention education in children. One with 492 samples was school-based, and a 50-minute interactive workshop session was presented for the second- and third-grade students, using an age-appropriate activity book on body safety and puppets for role-playing scenarios. The following key concepts were discussed during that session: private parts of the body, the difference between safe and not-safe touch, secret and surprise differences, information that bad touch may be given by familiar ones, the fact that the child should keep telling an adult, so that s/he is convinced, that the child is not supposed to be blamed for receiving bad touch, a list of what the child can do while experiencing bad touch, one who should be informed at such cases, and assertive language skills to show discomfort and talk to reliable adults for reporting bad touch. This type of education promoted the knowledge about not-safe touch in children (P<0.001) (23).
The other intervention study using lecture and active approaches such as role-playing, coping skills, group study paper, and the game was scheduled for six 40-minute sessions. Instructions such as the CSA, good and bad feelings, recognizing unsafe situations, coping skills, providing appropriate answers, and the actions to take when encountering sexual abuse were provided for 39 fifth-grade students. The results revealed that this intervention could be effective in increasing the self-protective behaviors about sexual abuse in students (24).
Body image
In an educational intervention, concepts such as valuing diversity in appearance, respecting one’s unique appearance, managing appearance-related teasing, and developing resilience to peer pressure and media about appearance were instructed. The content was presented to 9- and 10-year-old children through brainstorming, class discussion, small group work, pair work, role-playing, and watching movies during six 1-hour sessions. In this study, 74 girls and 70 boys were recruited. Sustainable improvement instructional sessions led to good body esteem in girls, especially those with lower body esteem at the beginning of the study, though they were not effective in boys. Girls had lower body esteem at the baseline, and this primary satisfaction affected the outcome of the intervention. Moreover, peer pressure may be more effective in this age group and intervention increases the knowledge of talking positively about the appearance among the girls and not the boys (25).
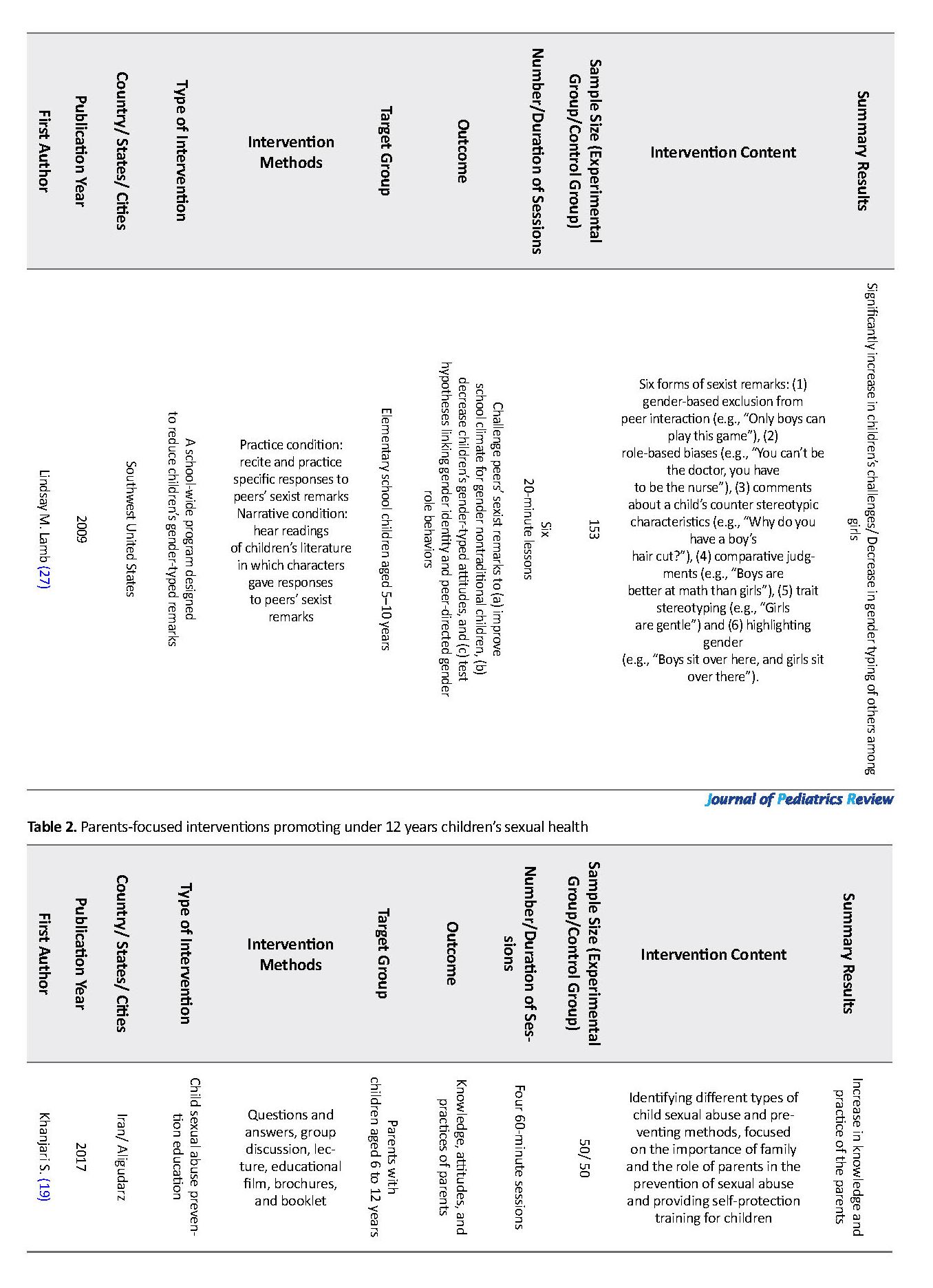
Decrease in gender-typed remarks
One study performed a school-wide program to decrease gender-typed remarks. It presented 6 concepts: 1. gender-based exclusion from peer interaction (just boys can play this game); 2. role-based biases (you cannot be a doctor; you have to be a nurse.); 3. stereotypes about appearance (why do you have boyish haircut?); 4. comparative judgment (boys outperform girls at math.); 5. trait stereotyping (girls are gentle.); and 6. highlighting gender in a neutral context (boys sit here, and girls sit there). These concepts were taught in six 20-minute sessions by narrative and practice conditions so that students could learn how to react to the gender-typed remarks of their peers. In this study, 153 students aged 5-10 years took part. The intervention enhanced the confrontation ability of the children with sexist remarks and decreased the gender-typed attitudes leading to a better atmosphere at school (27).
Parents-focused interventions
Four studies out of 7 had worked on mothers with preschool children (18, 28, 30, 31), two worked on parents with primary school-age children (19, 29), and one researched parents with 2-12-year-old children (20). In one study, instruction for preventing child sexual abuse was provided for the participants (19). The other 6 studies gave instructions on children sexual education (20), preschooler sexual education for mothers (18), children sexual care based on BASNEF model (28), sexual education program for mothers (30, 31), and a theoretical-based, client-center, multi-method program for kids (29) (Table 2).
Sexual abuse prevention
A study instructed parents with children of 6-12 years old on how to prevent CSA. Educational entities included recognizing different types of sexual abuse and prevention methods, the importance of family and the role of parents in preventing sexual abuse, and providing a self-protection instruction program for children. This program took place in four 60-minute sessions using lectures, question and answer, group discussion, educational movies, brochures, and booklet. The results revealed that the parents’ knowledge and performance improved, though it did not have any effects on their attitude, probably because of cultural issues and concerns about the consequences of sex education to children (19).
Upbringing and children sexual health
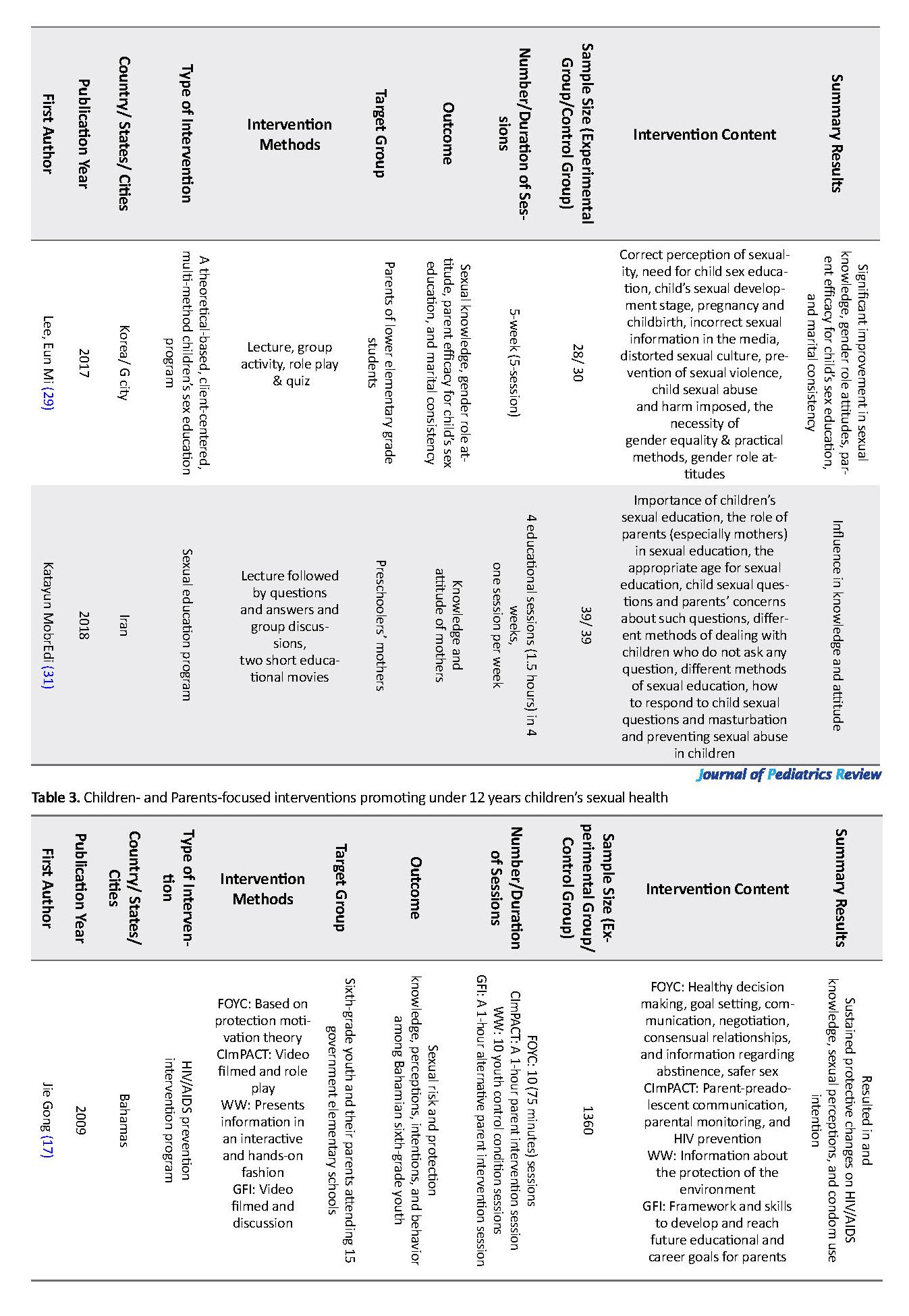
Six studies instructed upbringing and children’s sexual health to parents. The average sample size of these studies was 71.16 participants. The instructed concepts included the proper meaning of sexuality, the importance of the parents’ knowledge about sexual education and their role in this respect, children sexual growth and development, hygiene and function of genital organs, sexual behaviors in different stages of childhood, gender role development and stereotypes, attitudes towards gender role, gender equity, the necessity of sexual education to children and the appropriate age of education, providing answer to the children’s sexual questions, biological sex, sexual identity, sexual deviation, treatment programs (promoting the child’s self-esteem, self-management, safety rules, behavioral outcomes), destructive sexual culture, improper sexual information in media, unethical and inappropriate instruments, sexual violence, privacy, child abuse prevention, maturity, reproduction and birth, and masturbation in children.
These concepts were taught during 2 to 7 sessions of 90 to 120 minutes. The teaching methods contained question and answer, group discussion, short instructional film, group activity, examination, role-playing, smartphones, picture book, pictures, and exam sheets (18, 20, 28-31). The results revealed that interventions were effective in improving sexual knowledge and attitude (18, 20, 29-31), sexual attitude (18, 28, 30, 31), attitude towards gender role (29), mental norms, behavioral intention, behavior related to sexual care of children (28), and parents’ competence in giving sexual instruction to children (20, 29).
Children- and parents-focused interventions
The target groups of 4 studies were the fourth-, fifth-, and sixth-grade students, along with their parents. Three of the studies had worked on preventive instruction and decreasing the risk of HIV/AIDS (17, 32, 34) and one study dealt with saving sex for later (33) (Table 3).
Prevention and decreasing the risk of HIV/AIDS
Out of three studies dealing with teaching prevention and decreasing the risk of HIV/AIDS program, two had worked on 1360 (17, 32) and one on 639 (34) students and their parents. Educational concepts included decision-making skill, goal-setting, communication, negotiation, consensual relationship, knowledge, and skill related to abstinence, safe sex, parent-child communication about sexual activity, parental monitoring, HIV prevention, demonstrating and practicing condom use, self-protection rules, talking about puberty and preparing children for adolescence (17, 32, 34).
Instructional sessions in one study took place in ten 75-minute sessions and one 1-hour session (14). In the other two studies, interventions were held in eight (32) and twelve 90-minute sessions (34). Instructions were presented in video films, role-playing, consensual discussion, games, workgroups, and scheduled activities. Instructions led to preventive changes in HIV/AIDS knowledge, sexual perception, intention to use a condom, family key variables, including decision-making skills, family relationships, and ease of communication about sensitive issues. Moreover, there was an increase in the ability to use condom and self-efficiency in adolescence (17, 32, 34).
Saving sex for later
In one study, saving sex for later in a parent education program was presented to 846 families, both students, and their parents. This intervention included key messages about the importance of positive and continuous parental practices and the introduction of physical, emotional, and social changes of growth in audio CDs. These CDs were sent to the families in 3 phases with 12-week intervals for 6 months. The results indicated that saving sex for later was a promising intervention for sexual abstinence during adolescence (33).
The Impact of culture and religion
Because of diverse cultures and religions, sexual education programs vary across countries. For example, sexual education is provided in primary or secondary schools in the Netherlands, Austria, Brazil, and the United States (35-37), whereas in Spain and Portugal, the first formal education on sexual issues takes place before pregnancy. Though the incidence of teenage pregnancy and STDs (sexually transmitted diseases) are high in these countries (38). In some societies, childhood sexual issues are ignored, and it is believed that child education is not necessary because of the innocence of children (39). For example, there is no formal education program in India and the source of sexual information for teens is the Internet, books, and peers (40).
Similarly, in Malaysia, little attention is paid to sexual education in schools (41). Sexual and reproductive health is sensitive both politically and culturally in most countries in the Middle East and North Africa. The majority of adolescents lack access to reproductive health information and services. However, in a few countries, such as Tunisia, Morocco, Yemen, and Turkey, gender and fertility issues are being addressed (42). In Iran, there is no formal sex education program for children and limited studies have been conducted in this area (3). Only one interventional study entitled: “The effect of children’s sexual health educational program on knowledge and attitudes of primary school health care providers” was conducted by Barimani et al. in the school setting in 2019. The results of this study showed that the native educational protocol promoted the knowledge and attitudes of school health care providers. Thus, despite all limitations, appropriate intervention can be useful in improving outcomes.
Sexual health is based on people’s knowledge; physical, and mental health; economic status; and social values. However, one’s knowledge, which can be achieved by sexual training, plays the most crucial role in approaching an appropriate level of sexual health (1). Sexual training consists of instructing knowledge of reproduction, sexual issues, and attitude towards it and may be performed at schools or some other educational settings (2).
Sexual health issue comprises both genders at all age groups. However, sexual health and its importance can be defined differently in various periods of life. For instance, sexual health in children means providing a safe environment for normal sexual growth and preventing sexual abuse (1). Although sexual incentive and behavior are instinctive, it is affected by environmental factors if not guided and appropriately trained. This defect may lead to some problems and threaten the mental and physical health of the person. Therefore, parents and teachers should provide their children and students with sexual knowledge as they are growing up. Sexual training along with teaching the values, norms, and controlling skills, result in the prevention of early, High risk, and unprotected sexual activities and guarantees the individual’s health in the present and future (2-4).
Sexual education is not taught to most of the children, and this ignorance may adversely affect different dimensions of one’s sexual health. Girls may receive some information about menstruation from their mothers, while boys do not receive similar guides. Talking to children about this issue constantly but briefly can have positive effects on their relationships and sexual health (5). It should be emphasized that if children and teenagers cannot receive appropriate answers to their questions, they may refer to their peers and improper sources. Therefore, providing them with proper information and giving adequate answers to their questions is of great importance (6). Children’s knowledge about sexual issues plays a decisive role in their development, general and sexual health, and reproduction. Thus, it is necessary to provide them with sexual information. Sexual education should be considered as an individual’s right to education (7, 8).
Few people all over the world receive the necessary preparations, such as decision-making skills, refusal skills, body safety rules, and sexual abuse prevention for their sexual life. This lack of knowledge makes them vulnerable to rape, sexual abuse, unwanted pregnancy, and sexually transmitted diseases (9, 10). Child Sexual Abuse (CSA) puts children in an embarrassing situation, bringing about short-term and long-term consequences such as fear, isolation, aggression, low self-esteem, embarrassment, inappropriate sexual behaviors, depression, and suicide. Moreover, sexual abuse experience in childhood is associated with negative body image and sexual dysfunction in adulthood (11). Hence, children need care, supervision, and training throughout their sexual development (12).
Both family and school are responsible for sexual training, but a review of literature has shown that most often, the consequences are not satisfactory (7). Primary school teachers are the key service providers for sexual training to children, families, and society. However, they are worried about the parents’ attitude towards such training programs and class management considering the children’s puberty stage, knowledge, and comfort. Thus, the teachers’ relationship with parents should be encouraged, and they must receive training about children’s sexual health (13). Parents and caregivers, as the primary educators, can play an essential role in protecting children’s sexual health (14, 15). However, their efforts can be compromised by insufficient knowledge, lack of skills, and comfort (16). Formal sexual instruction at schools consisting of sexual decision-making skills and Sexually Transmitted Infection (STI) prevention can promote adolescence and youth health conditions (10). The study conducted by Gong J et al. revealed that HIV/AIDS prevention programs based on protection motivation theory (PMT-based instruction) for children and their parents had positive effects on their HIV/AIDS knowledge, sexual perception, and condom use intention (17). Martin J et al. found out that sexual instruction to the mothers of preschool children increased their knowledge and attitude score (18).
Similarly, other studies demonstrated that instructing parents in children’s sexual health affects their knowledge, performance, and self-efficacy (19, 20). Some of the sexual health interventions may decrease other unwanted health consequences such as substance abuse or behavioral disorders. Some other interventions appear to be useful, though less effective in families and children with serious problems (18). Review studies conducted on sexual health have not focused on educational intervention for children under 12 (7, 12, 21, 22). Therefore, this study aimed at reviewing different types of educational interventions related to the sexual health of children under 12 years. We hope to recognize the interventions promoting the children’s sexual health.
2. Evidence Acquisition
In this narrative review, Google Scholar, PubMed, Scopus, Science Direct, and Web of Science databases were searched using the following keywords: “sex education", “sexual education", “sexual health", “sexual training and children". Two researchers (Zahra Barimani Aboksari and Maedeh Rezaei) searched articles related to children’s sexual health up to December 2018. Articles were included based on the subject of the study (sexual health of children under 12), study design (experimental, quasi-experimental, before-after studies), and consequences of the intervention (children’s sexual health). Irrelevant studies were excluded from the review process. Data extraction was done by two researchers (Zahra Barimani Aboksari and Maedeh Rezaei).
3. Results
The relevant articles were categorized into 4 groups:
1. Children-focused interventions; 2. Parent-focused interventions; 3. Children- and parent-focused interventions; 4. The impact of culture and religion.
Those studies conducted on children were 5 articles (23-27), those done on parents included 7 articles (18-20, 28-31), and 4 studies had been conducted on both (17, 32-34). Among the 16 articles, 5 were conducted in Iran, 4 in the USA, 4 in Korea, 2 in the Bahamas, and one in England.
Children-focused interventions
Studies on 8- to 12-year-old children had investigated peer-led sex education (26), sexual abuse prevention training and appropriate touch (23, 24), body image (25), and decrease in gender-type remarks (27). These studies were carried out from 2004 to 2018 (Table 1).
Sexuality education coaching program
One study had investigated peer-led sexuality education. The children were 11 to 12 years old, and the syllabus consisted of sexual knowledge (sexual differentiation, pornography, and communication) and sexual attitude (sexual concept, relationship, physical development, sexual-psychological development, sexual health, the value of life, and sexual violence). It was taught to 21 fifth- and sixth-grade students in primary school during 10 sessions. Instruments such as activity paper, proverb card, vulgar belief card, worrying box, video, sonogram, children’s storybook, embryo album activity paper, task, sentence card, and textbook were used. The results of this study indicated that peer-led sexual education promoted sexual knowledge and attitude in children (26).
Preventing sexual abuse
Two articles worked on sexual abuse prevention education in children. One with 492 samples was school-based, and a 50-minute interactive workshop session was presented for the second- and third-grade students, using an age-appropriate activity book on body safety and puppets for role-playing scenarios. The following key concepts were discussed during that session: private parts of the body, the difference between safe and not-safe touch, secret and surprise differences, information that bad touch may be given by familiar ones, the fact that the child should keep telling an adult, so that s/he is convinced, that the child is not supposed to be blamed for receiving bad touch, a list of what the child can do while experiencing bad touch, one who should be informed at such cases, and assertive language skills to show discomfort and talk to reliable adults for reporting bad touch. This type of education promoted the knowledge about not-safe touch in children (P<0.001) (23).
The other intervention study using lecture and active approaches such as role-playing, coping skills, group study paper, and the game was scheduled for six 40-minute sessions. Instructions such as the CSA, good and bad feelings, recognizing unsafe situations, coping skills, providing appropriate answers, and the actions to take when encountering sexual abuse were provided for 39 fifth-grade students. The results revealed that this intervention could be effective in increasing the self-protective behaviors about sexual abuse in students (24).
Body image
In an educational intervention, concepts such as valuing diversity in appearance, respecting one’s unique appearance, managing appearance-related teasing, and developing resilience to peer pressure and media about appearance were instructed. The content was presented to 9- and 10-year-old children through brainstorming, class discussion, small group work, pair work, role-playing, and watching movies during six 1-hour sessions. In this study, 74 girls and 70 boys were recruited. Sustainable improvement instructional sessions led to good body esteem in girls, especially those with lower body esteem at the beginning of the study, though they were not effective in boys. Girls had lower body esteem at the baseline, and this primary satisfaction affected the outcome of the intervention. Moreover, peer pressure may be more effective in this age group and intervention increases the knowledge of talking positively about the appearance among the girls and not the boys (25).
Decrease in gender-typed remarks
One study performed a school-wide program to decrease gender-typed remarks. It presented 6 concepts: 1. gender-based exclusion from peer interaction (just boys can play this game); 2. role-based biases (you cannot be a doctor; you have to be a nurse.); 3. stereotypes about appearance (why do you have boyish haircut?); 4. comparative judgment (boys outperform girls at math.); 5. trait stereotyping (girls are gentle.); and 6. highlighting gender in a neutral context (boys sit here, and girls sit there). These concepts were taught in six 20-minute sessions by narrative and practice conditions so that students could learn how to react to the gender-typed remarks of their peers. In this study, 153 students aged 5-10 years took part. The intervention enhanced the confrontation ability of the children with sexist remarks and decreased the gender-typed attitudes leading to a better atmosphere at school (27).
Parents-focused interventions
Four studies out of 7 had worked on mothers with preschool children (18, 28, 30, 31), two worked on parents with primary school-age children (19, 29), and one researched parents with 2-12-year-old children (20). In one study, instruction for preventing child sexual abuse was provided for the participants (19). The other 6 studies gave instructions on children sexual education (20), preschooler sexual education for mothers (18), children sexual care based on BASNEF model (28), sexual education program for mothers (30, 31), and a theoretical-based, client-center, multi-method program for kids (29) (Table 2).
Sexual abuse prevention
A study instructed parents with children of 6-12 years old on how to prevent CSA. Educational entities included recognizing different types of sexual abuse and prevention methods, the importance of family and the role of parents in preventing sexual abuse, and providing a self-protection instruction program for children. This program took place in four 60-minute sessions using lectures, question and answer, group discussion, educational movies, brochures, and booklet. The results revealed that the parents’ knowledge and performance improved, though it did not have any effects on their attitude, probably because of cultural issues and concerns about the consequences of sex education to children (19).
Upbringing and children sexual health
Six studies instructed upbringing and children’s sexual health to parents. The average sample size of these studies was 71.16 participants. The instructed concepts included the proper meaning of sexuality, the importance of the parents’ knowledge about sexual education and their role in this respect, children sexual growth and development, hygiene and function of genital organs, sexual behaviors in different stages of childhood, gender role development and stereotypes, attitudes towards gender role, gender equity, the necessity of sexual education to children and the appropriate age of education, providing answer to the children’s sexual questions, biological sex, sexual identity, sexual deviation, treatment programs (promoting the child’s self-esteem, self-management, safety rules, behavioral outcomes), destructive sexual culture, improper sexual information in media, unethical and inappropriate instruments, sexual violence, privacy, child abuse prevention, maturity, reproduction and birth, and masturbation in children.
These concepts were taught during 2 to 7 sessions of 90 to 120 minutes. The teaching methods contained question and answer, group discussion, short instructional film, group activity, examination, role-playing, smartphones, picture book, pictures, and exam sheets (18, 20, 28-31). The results revealed that interventions were effective in improving sexual knowledge and attitude (18, 20, 29-31), sexual attitude (18, 28, 30, 31), attitude towards gender role (29), mental norms, behavioral intention, behavior related to sexual care of children (28), and parents’ competence in giving sexual instruction to children (20, 29).
Children- and parents-focused interventions
The target groups of 4 studies were the fourth-, fifth-, and sixth-grade students, along with their parents. Three of the studies had worked on preventive instruction and decreasing the risk of HIV/AIDS (17, 32, 34) and one study dealt with saving sex for later (33) (Table 3).
Prevention and decreasing the risk of HIV/AIDS
Out of three studies dealing with teaching prevention and decreasing the risk of HIV/AIDS program, two had worked on 1360 (17, 32) and one on 639 (34) students and their parents. Educational concepts included decision-making skill, goal-setting, communication, negotiation, consensual relationship, knowledge, and skill related to abstinence, safe sex, parent-child communication about sexual activity, parental monitoring, HIV prevention, demonstrating and practicing condom use, self-protection rules, talking about puberty and preparing children for adolescence (17, 32, 34).
Instructional sessions in one study took place in ten 75-minute sessions and one 1-hour session (14). In the other two studies, interventions were held in eight (32) and twelve 90-minute sessions (34). Instructions were presented in video films, role-playing, consensual discussion, games, workgroups, and scheduled activities. Instructions led to preventive changes in HIV/AIDS knowledge, sexual perception, intention to use a condom, family key variables, including decision-making skills, family relationships, and ease of communication about sensitive issues. Moreover, there was an increase in the ability to use condom and self-efficiency in adolescence (17, 32, 34).
Saving sex for later
In one study, saving sex for later in a parent education program was presented to 846 families, both students, and their parents. This intervention included key messages about the importance of positive and continuous parental practices and the introduction of physical, emotional, and social changes of growth in audio CDs. These CDs were sent to the families in 3 phases with 12-week intervals for 6 months. The results indicated that saving sex for later was a promising intervention for sexual abstinence during adolescence (33).
The Impact of culture and religion
Because of diverse cultures and religions, sexual education programs vary across countries. For example, sexual education is provided in primary or secondary schools in the Netherlands, Austria, Brazil, and the United States (35-37), whereas in Spain and Portugal, the first formal education on sexual issues takes place before pregnancy. Though the incidence of teenage pregnancy and STDs (sexually transmitted diseases) are high in these countries (38). In some societies, childhood sexual issues are ignored, and it is believed that child education is not necessary because of the innocence of children (39). For example, there is no formal education program in India and the source of sexual information for teens is the Internet, books, and peers (40).
Similarly, in Malaysia, little attention is paid to sexual education in schools (41). Sexual and reproductive health is sensitive both politically and culturally in most countries in the Middle East and North Africa. The majority of adolescents lack access to reproductive health information and services. However, in a few countries, such as Tunisia, Morocco, Yemen, and Turkey, gender and fertility issues are being addressed (42). In Iran, there is no formal sex education program for children and limited studies have been conducted in this area (3). Only one interventional study entitled: “The effect of children’s sexual health educational program on knowledge and attitudes of primary school health care providers” was conducted by Barimani et al. in the school setting in 2019. The results of this study showed that the native educational protocol promoted the knowledge and attitudes of school health care providers. Thus, despite all limitations, appropriate intervention can be useful in improving outcomes.
Conclusions
Intervention in the domain of children’s sexual health leads to improvement in knowledge, attitude, and behavior of both children and parents. Since children can learn the related concepts and skills and parents, as the first instructors, play an essential role in this regard, enabling both groups is of great importance in providing and promoting children’s sexual health. On the other hand, sexual health in childhood can guarantee the sexual health of the coming years of life; therefore, it is worthwhile to pay attention to this issue and set plans and policies based on these interventions in familial and social aspects.
Intervention in the domain of children’s sexual health leads to improvement in knowledge, attitude, and behavior of both children and parents. Since children can learn the related concepts and skills and parents, as the first instructors, play an essential role in this regard, enabling both groups is of great importance in providing and promoting children’s sexual health. On the other hand, sexual health in childhood can guarantee the sexual health of the coming years of life; therefore, it is worthwhile to pay attention to this issue and set plans and policies based on these interventions in familial and social aspects.
The strength of this study was the exploration of different types of educational interventions related to the sexual health of children under 12 years, while previous studies did not consider it. On the other hand, the limitation of this study was the lack of searching the humanities and psychiatric databases.
The findings of this study help provide counseling and education by pediatricians, psychiatrists, psychologists, and counselors. The results can also be used to design and implement educational programs for families, teachers, and health care providers.
Ethical Considerations
Compliance with ethical guidelines
The authors fully respected the ethical considerations and general standards for publication, including avoiding plagiarism, fabrication, data construction, data falsification, and the simultaneous subdivision of an article in several journals. This study was approved by the Research Council and Ethics Committee of Mazandaran University of Medical Sciences (Code: IR.MAZUMS.REC.1398.5199).
Funding
This study was supported by the Student Research Committee of Mazandaran University of Medical Sciences.
Authors contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
We sincerely appreciate Mazandaran University of Medical Sciences and the Student Research Committee for funding this project.
References
Rashidi BH, Kiyani K, Haghollahi F, Sighaldeh SS. [Sexual health definition from the perspective of Iranian experts and description its components (Persian)]. Tehran University Medical Journal. 2015; 73(3):210-20.
Faghihi AN, Shokoohi Yekta M, Parand A. [Sexual education of children and adolescents based on Islamic view and psychological studies (Persian)]. Islamic Education. 2009; 3(7):51-80.
Abolghasemi N, Merghati Khoei E, Taghdissi H. [Teachers’ perceptions of sex education of primary school children (Persian)]. Journal of School of Public Health and Institute of Public Health Research. 2010; 8(2):27-39.
Abedini E, Tabibi Z, Ziaee P, Zarezade Kheibari S. A qualitative study on mothers’ experiences from sex education to female adolescents underlining cultural factors. Journal of Fundamentals of Mental Health. 2016; 18(4):202-11.
Walsh J. Talk soon, Talk often: A guide for parents talking to their kids about sex. Perth: Government of Western Australia, Department of Health; 2012.
Kalantary S, Ghana S, Sanagoo A, Jouybari L. [Puberty and sex education to girls: Experiences of Gorganians’ mothers (Persian)]. Journal of Health Promotion Management. 2013; 2(3):74-90.
Pop MV, Rusu AS. The role of parents in shaping and improving the sexual health of children-lines of developing parental sexuality education programs. Procedia-Social and Behavioral Sciences. 2015; 209:395-401. [DOI:10.1016/j.sbspro.2015.11.210]
Gursimsek I. Sexual education and teacher candidates’ attitudes towards sexuality. Journal of Psychologists and Counsellors in Schools. 2010; 20(1):81-90. [DOI:10.1375/ajgc.20.1.81]
Latif Nejad R, Nouri MJ, Hasanpour M, Hazaveyi SMM, Taghipour A. [The necessity of sexual-health education for Iranian female adolescents: A qualitative study (Persian)]. The Iranian Journal of Obstetrics, Gynecology and Infertility. 2012; 15(12):7-17.
Breuner CC, Mattson G, Child CoPAo, Health F. Sexuality education for children and adolescents. Pediatrics. 2016; 138(2):e20161348. [DOI:10.1542/peds.2016-1348] [PMID]
Firuzi H, Amiri F, Saadati N, Rostami M. [The effects of childhood abuse on women’s body image and sexual function (Persian)]. Journal of Fundamentals of Mental Health. 2016; 18(6):313-20.
Ganji J, Emamian MH, Maasoumi R, Keramat A, Khoei EM. [The existing approaches to sexuality education targeting children: A review article (Persian)]. Iranian Journal of Public Health. 2017; 46(7):890-8.
Milton J. Primary school sex education programs: Views and experiences of teachers in four primary schools in Sydney, Australia. Sex Education. 2003; 3(3):241-56. [DOI:10.1080/1468181032000119122]
Ganji J, Emamian MH, Maasoumi R, Keramat A, Khoei EM. [Sexual health education at home: Attitude and practice of Iranian parents (Persian)]. Iranian Journal of Public Health. 2018; 47(1):146-7.
Ganji J, Emamian MH, Maasoumi R, Keramat A, Merghati-Khoei E. [Qualitative needs assessment: Iranian parents’ perspectives in sexuality education of their children (Persian)]. Journal of Nursing and Midwifery Sciences. 2018; 5(4):140-6.
Barimani Aboksari Z, Ganji J, Mousavinasab N, khani S. [Factors influencing children’s sexual health education: A review study (Persian)]. Clinical Excellence. 2018; 8(1):5-6.
Gong J, Stanton B, Lunn S, Deveaux L, Li X, Marshall S, et al. Effects through 24 months of an HIV/AIDS prevention intervention program based on protection motivation theory among preadolescents in the Bahamas. Pediatrics. 2009; 123(5):e917-28. [DOI:10.1542/peds.2008-2363] [PMID] [PMCID]
Martin J, Riazi H, Firoozi A, Nasiri M. A sex education program for mothers in Iran: Does preschool children’s sex education influence mothers’ knowledge and attitudes? Sex Education. 2018; 18(2):219-30. [DOI:10.1080/14681811.2018.1428547]
Khanjari S, Modabber M, Rahmati M, Haghani H. Knowledge, attitudes and practices among parents of school-age children after child sexual abuse prevention education. Iran Journal of Nursing. 2017; 29(104):17-27. [DOI:10.29252/ijn.29.104.17]
Rashid K, Hosseini Nazarlou M. [Investigating the effect of sex education on enhancing parents’ sexual knowledge and their sense of competence (Persian)]. Journal of Instruction and Evaluation. 2017; 10(37):143-62.
Wight D, Fullerton D. A review of interventions with parents to promote the sexual health of their children. Journal of Adolescent Health. 2013; 52(1):4-27. [DOI:10.1016/j.jadohealth.2012.04.014] [PMID]
Kirby DB, Laris B, Rolleri LA. Sex and HIV education programs: Their impact on sexual behaviors of young people throughout the world. Journal of Adolescent Health. 2007; 40(3):206-17. [DOI:10.1016/j.jadohealth.2006.11.143] [PMID]
Pulido ML, Dauber S, Tully BA, Hamilton P, Smith MJ, Freeman K. Knowledge gains following a child sexual abuse prevention program among urban students: A cluster-randomized evaluation. American Journal of Public Health. 2015; 105(7):1344-50. [DOI:10.2105/AJPH.2015.302594] [PMID] [PMCID]
Kim SJ, Kang KA. Effects of the Child Sexual Abuse Prevention Education (C-SAPE) program on South Korean fifth-grade students’ competence in terms of knowledge and self-protective behaviors. The Journal of School Nursing. 2017; 33(2):123-32. [DOI:10.1177/1059840516664182] [PMID]
Halliwell E, Yager Z, Paraskeva N, Diedrichs PC, Smith H, White P. Body image in primary schools: A pilot evaluation of a primary school intervention program designed by teachers to improve children’s body satisfaction. Body Image. 2016; 19:133-41. [DOI:10.1016/j.bodyim.2016.09.002] [PMID]
Im Yl, Min PK. Effects of sexuality education coaching program on sex-related knowledge and attitude among elementary school students. Journal of Korean Academy of Nursing. 2014; 44(1):p31-40. [DOI:10.4040/jkan.2014.44.1.31] [PMID]
Lamb LM, Bigler RS, Liben LS, Green VA. Teaching children to confront peers’ sexist remarks: Implications for theories of gender development and educational practice. Sex Roles. 2009; 61(5-6):361-82. [DOI:10.1007/s11199-009-9634-4]
Hashemi Bakhshi S, Jalili Z, Mahmoudi M. [The effect of theory-based educational intervention on mothers’ skill about sexual care of their children (Persian)]. Journal of School of Public Health and Institute of Public Health Research. 2018; 16(1):87-98.
Lee EM, Kim H. Development and effects of a children’s sex education program for the parents of lower elementary grade students. Journal of Korean Academy of Nursing. 2017; 47(2):222-32. [DOI:10.4040/jkan.2017.47.2.222] [PMID]
Lee EM, Kweon YR. Effects of a maternal sexuality education program for mothers of preschoolers. Journal of Korean Academy of Nursing. 2013; 43(3):370-8. [DOI:10.4040/jkan.2013.43.3.370] [PMID]
Mobredi K, Azin SA, Haghani H, Farahani LA. Effect of the sexual education program on the knowledge and attitude of preschoolers’ mothers. Journal of Clinical & Diagnostic Research. 2018; 12(6):6-9. [DOI:10.7860/JCDR/2018/32702.11616]
Stanton B, Dinaj-Koci V, Wang B, Deveaux L, Lunn S, Li X, et al. Adolescent HIV risk reduction in the bahamas: Results from two randomized controlled intervention trials spanning elementary school through high school. AIDS and Behavior. 2016; 20(6):1182-96. [DOI:10.1007/s10461-015-1225-5] [PMID] [PMCID]
O’Donnell L, Stueve A, Agronick G, Wilson‐Simmons R, Duran R, Jeanbaptiste V. Saving sex for later: An evaluation of a parent education intervention. Perspectives on Sexual and Reproductive Health. 2005; 37(4):166-73. [DOI:10.1363/3716605] [PMID]
McKay MM, Chasse KT, Paikoff R, McKinney LD, Baptiste D, Coleman D, et al. Family‐level impact of the CHAMP Family Program: A community collaborative effort to support urban families and reduce youth HIV risk exposure. Family Process. 2004; 43(1):79-93. [DOI:10.1111/j.1545-5300.2004.04301007.x] [PMID]
Walker JL. A qualitative study of parents’ experiences of providing sex education for their children: The implications for health education. Health Education Journal. 2001; 60(2):132-46. [DOI:10.1177/001789690106000205]
Depauli C, Plaute W. Parents’ and teachers’ attitudes, objections and expectations towards sexuality education in primary schools in Austria. Sex Education. 2018; 18(5):511-26. [DOI:10.1080/14681811.2018.1433650]
da Silva DQ, Guerra OU, Sperling C. Sex education in the eyes of primary school teachers in Novo Hamburgo, Rio Grande do Sul, Brazil. Reproductive Health Matters. 2013; 21(41):114-23. [DOI:10.1016/S0968-8080(13)41692-0]
Villar ME, Concha M. Sex education and cultural values: Experiences and attitudes of Latina immigrant women. Sex Education. 2012; 12(5):545-54. [DOI:10.1080/14681811.2011.627733]
Merghati-khoei E, Abolghasemi N, Taghdissi M. [Sexual health of children: A qualitative study on the views of parents (Persian)]. Scientific Journal of School of Public Health. 2013; 11(2):65-74.
Mahajan P, Sharma N. Parent’s attitude towards imparting sex education to their adolescent girls. The Anthropologist. 2005; 7(3):197-9. [DOI:10.1080/09720073.2005.11890907]
Mazidi M, Khedmatiyan M. [Presenting a model for sexual education based on the views of Muslim thinkers (Persian)]. Islamic Education. 2017; 12(25):161-83.
Alquaiz AM, Almuneef MA, Minhas HR. Knowledge, attitudes, and resources of sex education among female adolescents in public and private schools in Central Saudi Arabia. Saudi Medical Journal. 2012; 33(9):1001-9. [PMID]
The findings of this study help provide counseling and education by pediatricians, psychiatrists, psychologists, and counselors. The results can also be used to design and implement educational programs for families, teachers, and health care providers.
Ethical Considerations
Compliance with ethical guidelines
The authors fully respected the ethical considerations and general standards for publication, including avoiding plagiarism, fabrication, data construction, data falsification, and the simultaneous subdivision of an article in several journals. This study was approved by the Research Council and Ethics Committee of Mazandaran University of Medical Sciences (Code: IR.MAZUMS.REC.1398.5199).
Funding
This study was supported by the Student Research Committee of Mazandaran University of Medical Sciences.
Authors contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
We sincerely appreciate Mazandaran University of Medical Sciences and the Student Research Committee for funding this project.
References
Rashidi BH, Kiyani K, Haghollahi F, Sighaldeh SS. [Sexual health definition from the perspective of Iranian experts and description its components (Persian)]. Tehran University Medical Journal. 2015; 73(3):210-20.
Faghihi AN, Shokoohi Yekta M, Parand A. [Sexual education of children and adolescents based on Islamic view and psychological studies (Persian)]. Islamic Education. 2009; 3(7):51-80.
Abolghasemi N, Merghati Khoei E, Taghdissi H. [Teachers’ perceptions of sex education of primary school children (Persian)]. Journal of School of Public Health and Institute of Public Health Research. 2010; 8(2):27-39.
Abedini E, Tabibi Z, Ziaee P, Zarezade Kheibari S. A qualitative study on mothers’ experiences from sex education to female adolescents underlining cultural factors. Journal of Fundamentals of Mental Health. 2016; 18(4):202-11.
Walsh J. Talk soon, Talk often: A guide for parents talking to their kids about sex. Perth: Government of Western Australia, Department of Health; 2012.
Kalantary S, Ghana S, Sanagoo A, Jouybari L. [Puberty and sex education to girls: Experiences of Gorganians’ mothers (Persian)]. Journal of Health Promotion Management. 2013; 2(3):74-90.
Pop MV, Rusu AS. The role of parents in shaping and improving the sexual health of children-lines of developing parental sexuality education programs. Procedia-Social and Behavioral Sciences. 2015; 209:395-401. [DOI:10.1016/j.sbspro.2015.11.210]
Gursimsek I. Sexual education and teacher candidates’ attitudes towards sexuality. Journal of Psychologists and Counsellors in Schools. 2010; 20(1):81-90. [DOI:10.1375/ajgc.20.1.81]
Latif Nejad R, Nouri MJ, Hasanpour M, Hazaveyi SMM, Taghipour A. [The necessity of sexual-health education for Iranian female adolescents: A qualitative study (Persian)]. The Iranian Journal of Obstetrics, Gynecology and Infertility. 2012; 15(12):7-17.
Breuner CC, Mattson G, Child CoPAo, Health F. Sexuality education for children and adolescents. Pediatrics. 2016; 138(2):e20161348. [DOI:10.1542/peds.2016-1348] [PMID]
Firuzi H, Amiri F, Saadati N, Rostami M. [The effects of childhood abuse on women’s body image and sexual function (Persian)]. Journal of Fundamentals of Mental Health. 2016; 18(6):313-20.
Ganji J, Emamian MH, Maasoumi R, Keramat A, Khoei EM. [The existing approaches to sexuality education targeting children: A review article (Persian)]. Iranian Journal of Public Health. 2017; 46(7):890-8.
Milton J. Primary school sex education programs: Views and experiences of teachers in four primary schools in Sydney, Australia. Sex Education. 2003; 3(3):241-56. [DOI:10.1080/1468181032000119122]
Ganji J, Emamian MH, Maasoumi R, Keramat A, Khoei EM. [Sexual health education at home: Attitude and practice of Iranian parents (Persian)]. Iranian Journal of Public Health. 2018; 47(1):146-7.
Ganji J, Emamian MH, Maasoumi R, Keramat A, Merghati-Khoei E. [Qualitative needs assessment: Iranian parents’ perspectives in sexuality education of their children (Persian)]. Journal of Nursing and Midwifery Sciences. 2018; 5(4):140-6.
Barimani Aboksari Z, Ganji J, Mousavinasab N, khani S. [Factors influencing children’s sexual health education: A review study (Persian)]. Clinical Excellence. 2018; 8(1):5-6.
Gong J, Stanton B, Lunn S, Deveaux L, Li X, Marshall S, et al. Effects through 24 months of an HIV/AIDS prevention intervention program based on protection motivation theory among preadolescents in the Bahamas. Pediatrics. 2009; 123(5):e917-28. [DOI:10.1542/peds.2008-2363] [PMID] [PMCID]
Martin J, Riazi H, Firoozi A, Nasiri M. A sex education program for mothers in Iran: Does preschool children’s sex education influence mothers’ knowledge and attitudes? Sex Education. 2018; 18(2):219-30. [DOI:10.1080/14681811.2018.1428547]
Khanjari S, Modabber M, Rahmati M, Haghani H. Knowledge, attitudes and practices among parents of school-age children after child sexual abuse prevention education. Iran Journal of Nursing. 2017; 29(104):17-27. [DOI:10.29252/ijn.29.104.17]
Rashid K, Hosseini Nazarlou M. [Investigating the effect of sex education on enhancing parents’ sexual knowledge and their sense of competence (Persian)]. Journal of Instruction and Evaluation. 2017; 10(37):143-62.
Wight D, Fullerton D. A review of interventions with parents to promote the sexual health of their children. Journal of Adolescent Health. 2013; 52(1):4-27. [DOI:10.1016/j.jadohealth.2012.04.014] [PMID]
Kirby DB, Laris B, Rolleri LA. Sex and HIV education programs: Their impact on sexual behaviors of young people throughout the world. Journal of Adolescent Health. 2007; 40(3):206-17. [DOI:10.1016/j.jadohealth.2006.11.143] [PMID]
Pulido ML, Dauber S, Tully BA, Hamilton P, Smith MJ, Freeman K. Knowledge gains following a child sexual abuse prevention program among urban students: A cluster-randomized evaluation. American Journal of Public Health. 2015; 105(7):1344-50. [DOI:10.2105/AJPH.2015.302594] [PMID] [PMCID]
Kim SJ, Kang KA. Effects of the Child Sexual Abuse Prevention Education (C-SAPE) program on South Korean fifth-grade students’ competence in terms of knowledge and self-protective behaviors. The Journal of School Nursing. 2017; 33(2):123-32. [DOI:10.1177/1059840516664182] [PMID]
Halliwell E, Yager Z, Paraskeva N, Diedrichs PC, Smith H, White P. Body image in primary schools: A pilot evaluation of a primary school intervention program designed by teachers to improve children’s body satisfaction. Body Image. 2016; 19:133-41. [DOI:10.1016/j.bodyim.2016.09.002] [PMID]
Im Yl, Min PK. Effects of sexuality education coaching program on sex-related knowledge and attitude among elementary school students. Journal of Korean Academy of Nursing. 2014; 44(1):p31-40. [DOI:10.4040/jkan.2014.44.1.31] [PMID]
Lamb LM, Bigler RS, Liben LS, Green VA. Teaching children to confront peers’ sexist remarks: Implications for theories of gender development and educational practice. Sex Roles. 2009; 61(5-6):361-82. [DOI:10.1007/s11199-009-9634-4]
Hashemi Bakhshi S, Jalili Z, Mahmoudi M. [The effect of theory-based educational intervention on mothers’ skill about sexual care of their children (Persian)]. Journal of School of Public Health and Institute of Public Health Research. 2018; 16(1):87-98.
Lee EM, Kim H. Development and effects of a children’s sex education program for the parents of lower elementary grade students. Journal of Korean Academy of Nursing. 2017; 47(2):222-32. [DOI:10.4040/jkan.2017.47.2.222] [PMID]
Lee EM, Kweon YR. Effects of a maternal sexuality education program for mothers of preschoolers. Journal of Korean Academy of Nursing. 2013; 43(3):370-8. [DOI:10.4040/jkan.2013.43.3.370] [PMID]
Mobredi K, Azin SA, Haghani H, Farahani LA. Effect of the sexual education program on the knowledge and attitude of preschoolers’ mothers. Journal of Clinical & Diagnostic Research. 2018; 12(6):6-9. [DOI:10.7860/JCDR/2018/32702.11616]
Stanton B, Dinaj-Koci V, Wang B, Deveaux L, Lunn S, Li X, et al. Adolescent HIV risk reduction in the bahamas: Results from two randomized controlled intervention trials spanning elementary school through high school. AIDS and Behavior. 2016; 20(6):1182-96. [DOI:10.1007/s10461-015-1225-5] [PMID] [PMCID]
O’Donnell L, Stueve A, Agronick G, Wilson‐Simmons R, Duran R, Jeanbaptiste V. Saving sex for later: An evaluation of a parent education intervention. Perspectives on Sexual and Reproductive Health. 2005; 37(4):166-73. [DOI:10.1363/3716605] [PMID]
McKay MM, Chasse KT, Paikoff R, McKinney LD, Baptiste D, Coleman D, et al. Family‐level impact of the CHAMP Family Program: A community collaborative effort to support urban families and reduce youth HIV risk exposure. Family Process. 2004; 43(1):79-93. [DOI:10.1111/j.1545-5300.2004.04301007.x] [PMID]
Walker JL. A qualitative study of parents’ experiences of providing sex education for their children: The implications for health education. Health Education Journal. 2001; 60(2):132-46. [DOI:10.1177/001789690106000205]
Depauli C, Plaute W. Parents’ and teachers’ attitudes, objections and expectations towards sexuality education in primary schools in Austria. Sex Education. 2018; 18(5):511-26. [DOI:10.1080/14681811.2018.1433650]
da Silva DQ, Guerra OU, Sperling C. Sex education in the eyes of primary school teachers in Novo Hamburgo, Rio Grande do Sul, Brazil. Reproductive Health Matters. 2013; 21(41):114-23. [DOI:10.1016/S0968-8080(13)41692-0]
Villar ME, Concha M. Sex education and cultural values: Experiences and attitudes of Latina immigrant women. Sex Education. 2012; 12(5):545-54. [DOI:10.1080/14681811.2011.627733]
Merghati-khoei E, Abolghasemi N, Taghdissi M. [Sexual health of children: A qualitative study on the views of parents (Persian)]. Scientific Journal of School of Public Health. 2013; 11(2):65-74.
Mahajan P, Sharma N. Parent’s attitude towards imparting sex education to their adolescent girls. The Anthropologist. 2005; 7(3):197-9. [DOI:10.1080/09720073.2005.11890907]
Mazidi M, Khedmatiyan M. [Presenting a model for sexual education based on the views of Muslim thinkers (Persian)]. Islamic Education. 2017; 12(25):161-83.
Alquaiz AM, Almuneef MA, Minhas HR. Knowledge, attitudes, and resources of sex education among female adolescents in public and private schools in Central Saudi Arabia. Saudi Medical Journal. 2012; 33(9):1001-9. [PMID]
Type of Study: Narrative Review |
Subject:
Gynecology and Obstetrics
Received: 2019/06/11 | Accepted: 2019/10/7 | Published: 2020/04/1
Received: 2019/06/11 | Accepted: 2019/10/7 | Published: 2020/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
