
Fri, Jul 24, 2026


Volume 12, Issue 3 (7-2024)
J. Pediatr. Rev 2024, 12(3): 243-252 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohammadi G, Ghorbani R, Khosravifar S, Babakhanian M. Medical Causes of Death in Iranian Children Aged 1-59 Months: A Systematic Review and Meta-analysis. J. Pediatr. Rev 2024; 12 (3) :243-252
URL: http://jpr.mazums.ac.ir/article-1-650-en.html
URL: http://jpr.mazums.ac.ir/article-1-650-en.html



1- Clinical Research Development Unit, Velayat Hospital, Semnan University of Medical Sciences, Semnan, Iran.
2- Department of Social Medicine, Social Determinants of Health Research Center, Faculty of Medicine, Semnan University of Medical Sciences, Semnan, Iran.
3- Department of Psychiatry, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran.
4- Social Determinants of Health Research Center, Semnan University Of Medical Sciences, Semnan, Iran. ,babakhanian.m@gmail.com
2- Department of Social Medicine, Social Determinants of Health Research Center, Faculty of Medicine, Semnan University of Medical Sciences, Semnan, Iran.
3- Department of Psychiatry, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran.
4- Social Determinants of Health Research Center, Semnan University Of Medical Sciences, Semnan, Iran. ,
Full-Text [PDF 712 kb]
(1236 Downloads)
| Abstract (HTML) (3543 Views)
Full-Text: (1212 Views)
Introduction
Child mortality rates serve as indicators of a country’s development and have been selected as a measure of progress [1]. This is crucial, as it is a significant determinant of health and human advancement, particularly for deaths that are preventable after the first weeks of life [2, 3].
According to the statistics published by the World Health Organization (WHO), there has been a decrease in the under-five mortality rate in recent years. In Iran, the rate was reported as 13.86 deaths per 1000 live births in 2018, which decreased to 13.40 deaths per 1000 live births in 2019. The 2019 disaggregated data showed mortality rates of 14.54 for boys and 13.28 for girls. The latest update from the organization states a global under-five mortality rate of 12.94 deaths per 1000 live births. According to studies, the rate of mortality of babies aged between 1 and 59 months was 80 out of 1000 births in low-income countries and six deaths per 1000 births in high-income countries [4, 5]. Some studies conducted across various regions of Iran have examined factors influencing mortality in children under five years old. The results of these studies indicate that several factors, such as parent’s education level and occupation, housing conditions, the distance of children from healthcare facilities, maternal age at marriage and childbirth, developmental indices of provinces, parental literacy rates, maternal employment, average income, life expectancy, birth weight, infant nutrition, and socio-economic status are significant determinants. Additionally, factors, such as birth order, birth spacing, birth complications, like birth injuries and pregnancy disorders, chronic and infectious diseases, and mortality due to accidents have been identified as influential contributors to this rate [6-11].
One of the most important indicators of children’s health is their mortality rate [1]. Understanding the causes of mortality is essential for implementing timely and effective preventive and therapeutic measures. Furthermore, through a more practical assessment of the risk factors contributing to children’s mortality, the current situation can be improved with appropriate planning and policymaking. Identifying the causes and determinants of mortality is highly important for ensuring the design and appropriate implementation of interventions to improve population health [12].
Therefore, aimed to systematically review the causes of death for children aged 1-59 months in recent years in Iran, in order to identify the factors contributing to child mortality to reduce mortality and improve children’s health in Iran.
Methods
This systematic review and meta-analysis was performed based on the systematic reviews and meta-analysis (PRISMA) guidelines.
Research question
What are the causes of mortality related to children aged 1-59 months in Iran?
Search process
Based on the inclusion criteria, we searched electronic databases, including EMBASE, PubMed, Scopus, Magiran and Web of Science, as well as the Google Scholar search engine up to January 2024. Other gray literature (such as conference proceedings and key journals) was also searched. The following operators were used: ([Cause] OR [cause-specific] AND [cause of death] OR [death cause] OR [death causes] OR [mortality] OR [child mortality] Or [infant mortality] OR [child mortalities] OR [mortalities, child] OR [mortality, child] AND [infant] OR [infant, newborn] OR [infant, premature] OR [infant, postmature] OR [newborn infant] OR [newborn infants] OR [newborns] OR (newborn] OR [children] OR [child] OR [child, preschool] OR [childs] AND [1–59-month] OR [2 to 5 years old] OR [1 and 23 months] AND [Iran]).
Target population
The target population included all died Iranian neonates and children aged 1–59 months.
Inclusion and exclusion criteria
The inclusion criteria were all observational studies that reported the causes of death in neonates and children aged 1-59 months, regardless of the language. The exclusion criterion was studies conducted in other countries (Table 1).
Type of exposure
Death in neonates and children aged 1-59 months.
Data extraction (selection and coding)
Full-text articles meeting the inclusion criteria were evaluated. Information such as the first author’s name, year of publication, study location, sample size, and causes of death was recorded in an Excel file. If additional information was needed from any of the articles, the corresponding author was contacted. All stages were performed independently by two individuals, and the compiled data were shared and combined.
Risk of bias assessment
The quality of studies was assessed independently by two individuals using the revised CONSORT risk of bias tool for clinical trials [17]. All studies that met the inclusion criteria were evaluated. Any discrepancies in assessments were resolved through discussion between the two individuals.
Analysis methods
Using Stata software, version 17 (Stata Corp LLC, College Station, Texas), the I² statistic was employed as the criterion for evaluating heterogeneity based on the quality of studies for subgroup analysis. The Begg test was used to assess publication bias. P<0.05 were considered significant in statistical tests.
Results
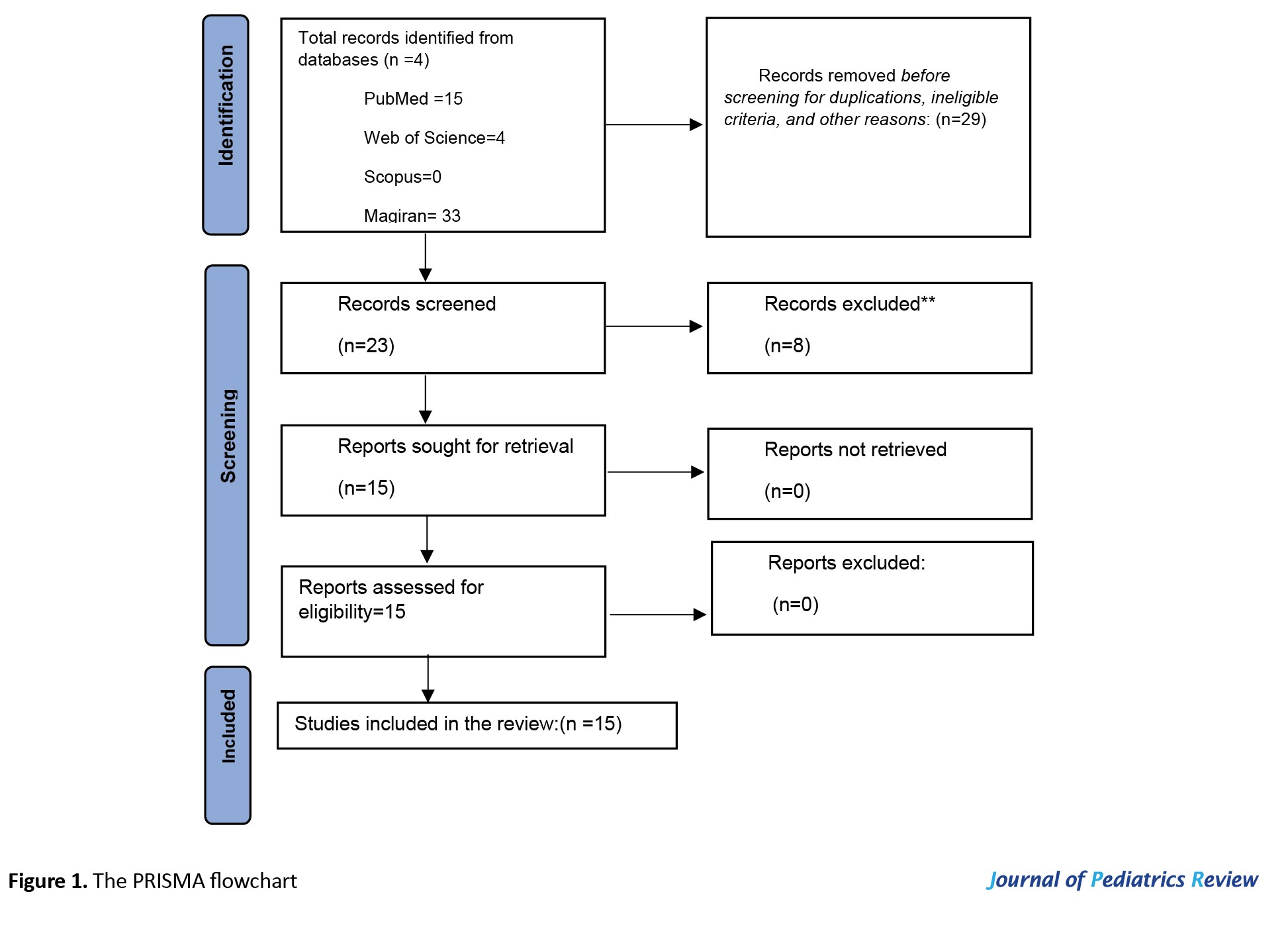
During the years under study (1999-2020), 15 studies were registered in Iran. Figure 1 shows the number of articles included in the study.
Characteristics of the included studies
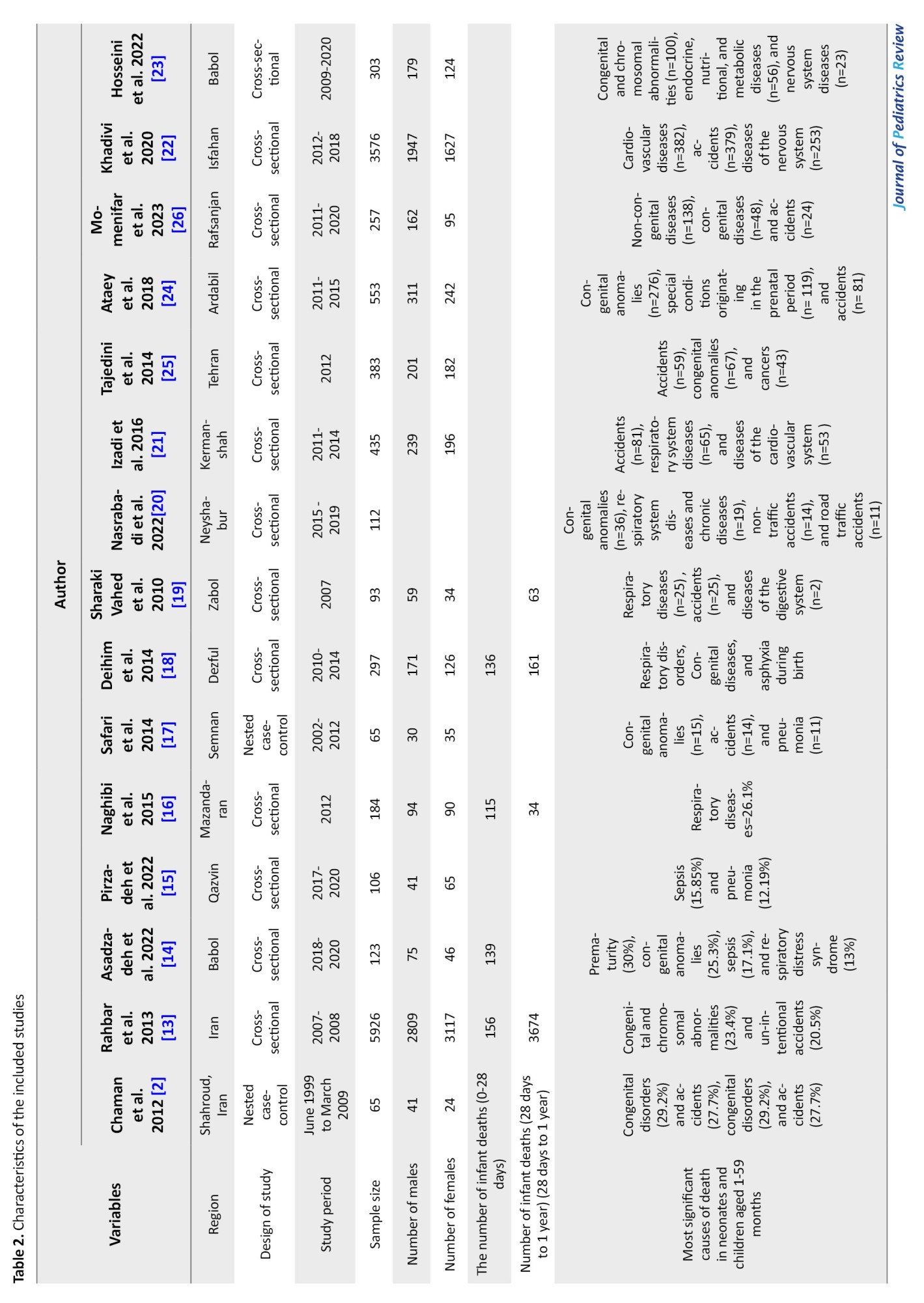
After initial evaluations, a total of 15 studies were included in the systematic review [2, 13-26]. The publication period of the articles ranged from 2010 to January 1, 2024 and the sample size of the studies varied from 65 to 3,576 patients (Table 2).
Quality assessment
About 31.2% of the studies had a low risk of bias, and 56.2% had a moderate risk. Two articles had a high risk of bias. In most studies, there was no explicit mention of the questions, “Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed?” and “For the analyses in this paper, were the exposures of interest measured before the outcomes?” This lack of clarity represented the biggest weakness in the quality of the evaluated studies (Table 3).

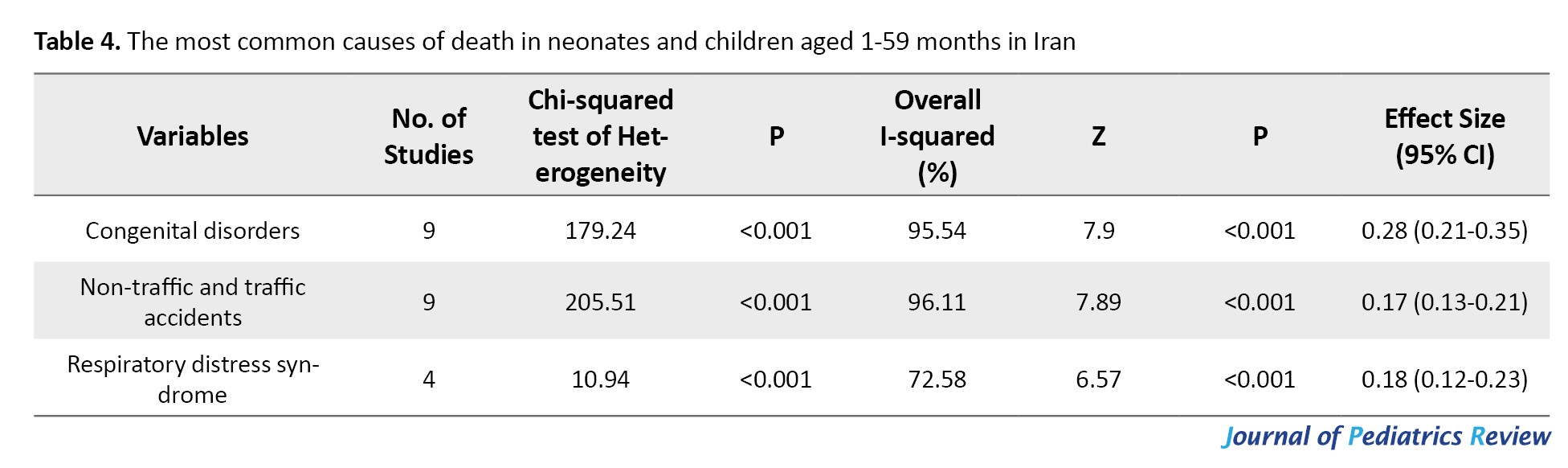
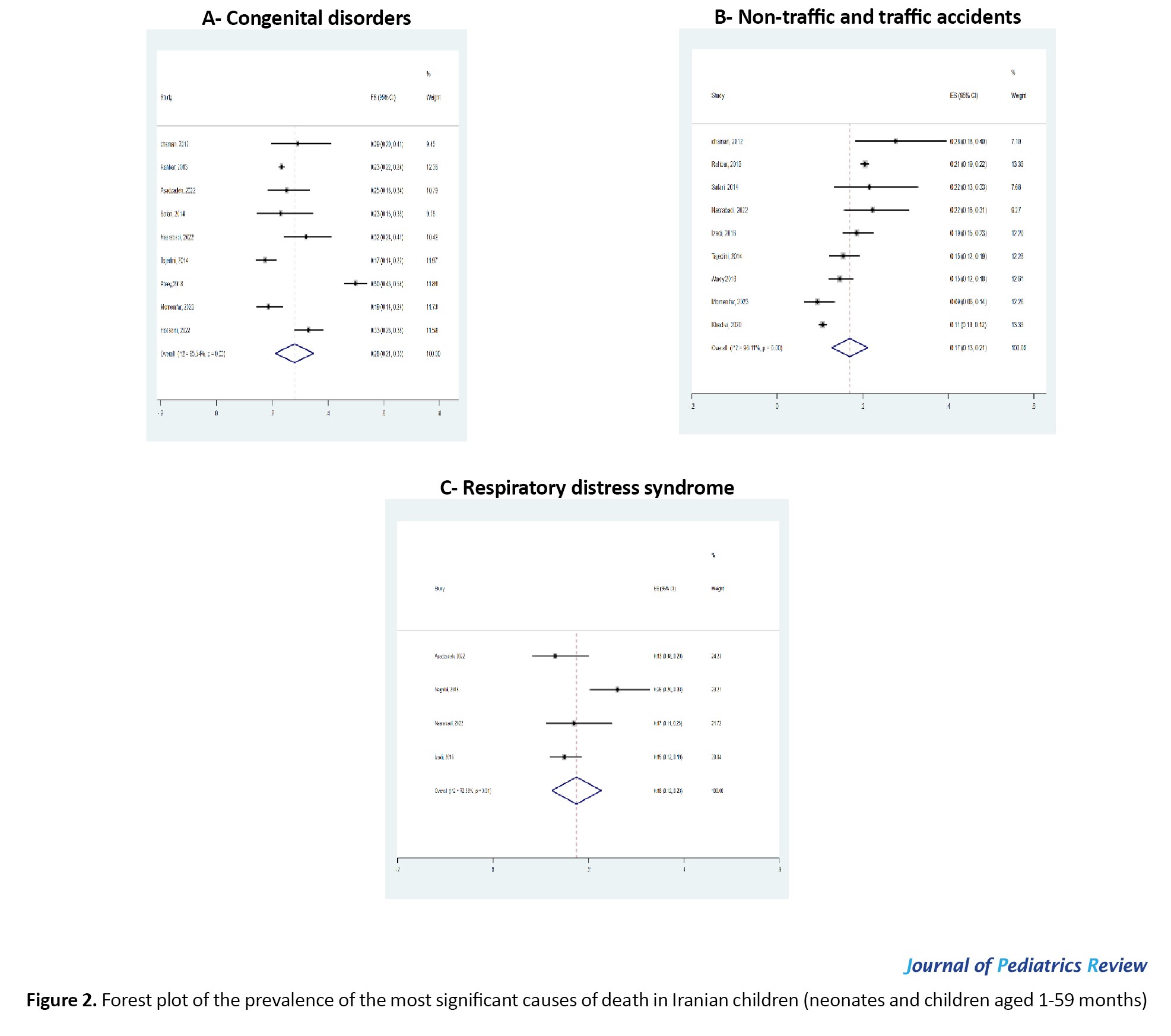
The main outcome of interest in this study, the prevalence of congenital disorders, was analyzed in nine studies. The results of the data analysis in this study indicated that the highest frequency of mortality occurs in boys. The three most significant causes of death among Iranian neonates and children aged 1-59 months, respectively, are congenital disorders (28%), respiratory distress syndrome (18%) and non-traffic and traffic accidents (17%).
In this random-effects model, the mean score of this cause was calculated as effect size (EF)=0.28 [95% CI, 0.21%, 0.35%]. Other important causes of mortality in Iranian children aged 1-59 months include respiratory distress syndrome EF=0.18 [95% CI, 0.12%, 0.23%] and non-traffic and traffic accidents EF=0.17 [95% CI, 0.13%, 0.21%] (Table 4 and Figure 2).
Publication bias
The Begg’s test was used to assess publication bias in this outcome. It examines the effect of small studies and shows a P=0.000. Since this value is significant, it indicates that there is no publication bias (adj. Kendall’s score (P-Q)=1, SD=1.000, z=0.000, and Pr>|z|=1.000).
Discussion
The results indicated that the highest frequency of mortality occurs in boys. The three most significant causes of death among Iranian neonates and children aged 1-59 months, respectively, are congenital disorders (28%), respiratory distress syndrome (18%) and non-traffic and traffic accidents (17%).
The mortality of infants and children is a public health concern. Congenital abnormalities increase the risk of mortality during infancy and childhood, accounting for 26% of infant deaths and over 10% of deaths in children under ten years old in Europe [27].
Our results also indicated that the primary cause of mortality among children under five years old, with a prevalence of 28%, is congenital disorders. This finding is consistent with the results of other studies conducted in various countries [27-29].
It is crucial to implement primary and secondary preventive strategies, such as early referrals to specialized centers for high-risk pregnancies and prenatal care. These strategies considerably reduce the death rate from congenital anomalies in children and adolescents [28, 29].
One of the weaknesses identified in the studies was the lack of precise registration of the types of congenital disorders and abnormalities. This oversight could have hindered efforts in primary and secondary prevention over time and impeded more accurate international comparisons. Globally, unintentional injuries and deaths resulting from external factors, such as accidents, being struck by objects at home, swallowing foreign objects, and various poisonings, including methadone poisoning or other toxic substances, are among the leading causes of death in children. These factors account for 30% of deaths in children aged 1 to 3 years, 40% of deaths in 4-year-old children, and 50% to 60% of deaths in children aged 5 to 17 years [30-32].
Since a significant percentage of these external causes of mortality are largely preventable but often overlooked, there is a critical need for effective education on injury prevention. This requires a multi-faceted approach [33]. In addition, conducting education programs on traffic safety is crucially important. In the event of such accidents, it is essential to promptly refer the child to the hospital. Rapid diagnosis and the initiation of treatment significantly increase the chances of a favorable outcome [32].
Our study findings revealed that the third leading cause of death among Iranian children under five years old is related to respiratory infections. Patients succumbed to severe viral or bacterial infections (such as sepsis, pneumonia, and COVID-19) despite receiving treatment, with little chance of survival. The COVID-19 pandemic has also impacted the causes of child mortality and altered their distribution. Most deceased children had an underlying condition, such as congenital abnormalities [32, 34]. The results of this analysis should be discussed, and the conclusions drawn should positively impact the quality of childcare. Similar studies in other countries confirm that in both high and low-income countries, the leading cause of mortality among children under five years old is often respiratory infections and sepsis. This underscores the importance of addressing these issues to improve child health outcomes globally [35, 36]. Low levels of literacy among women may contribute to higher rates of neonatal infections. Consequently, illiterate mothers may struggle to recognize signs of danger and infection-related symptoms in infants, necessitating urgent medical care [36].
Study limitations: If autopsies are not conducted to determine the primary cause of death in deceased individuals, there is essentially no other definitive standard that clearly indicates the actual cause of death in a child. This lack of clarity is evident in studies. Additionally, in most studies, the age of deceased individuals was not categorized into neonatal deaths (0–27 days), post-neonatal deaths (28–364 days), or child deaths (over 365 days). Furthermore, none of the causes of death were recorded using international classification of diseases 10th revision (ICD-10) or ICD-9 coding.
Conclusion
The most common reasons for mortality in children aged 1-59 months in Iran are congenital abnormalities, unintentional injuries, and deaths due to external factors and respiratory infections. However, without accurate recording of causes of death using ICD-10 coding, without conducting autopsies or registering more detailed age categories for children under five years old, it is not possible to adequately analyze extensive patterns of mortality in the country. Consequently, related public health planning may suffer, leading to reduced effectiveness in health interventions.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Semnan University of Medical Sciences (Code: IR.SEMUMS.REC.1400.10).
Funding
The present article was extracted from the general medical practitioner thesis of Zahra Khorsi, approved by the Faculty of Medicine, Semnan University of Medical Sciences. This study was financially supported by Semnan University of Medical Sciences.
Authors contributions
Conceptualization, project administration and funding acquisition: Gholamreza Mohammadi; Methodology and supervision: Masoudeh Babakhanian and Gholamreza Mohammadi; Software: Masoudeh Babakhanian; Validation: Gholamreza Mohammadi and Raheb Ghorbani; Formal analysis, investigation and writing the original draft: Masoudeh Babakhanian; Resources and data curation: Shaqayeq Khosravifar; Review and editing: Masoudeh Babakhanian, Gholamreza Mohammadi and Raheb Ghorbani; Visualization: Raheb Ghorbani.
Conflicts of interest
The authors declared no conflict of interest.
References
Child mortality rates serve as indicators of a country’s development and have been selected as a measure of progress [1]. This is crucial, as it is a significant determinant of health and human advancement, particularly for deaths that are preventable after the first weeks of life [2, 3].
According to the statistics published by the World Health Organization (WHO), there has been a decrease in the under-five mortality rate in recent years. In Iran, the rate was reported as 13.86 deaths per 1000 live births in 2018, which decreased to 13.40 deaths per 1000 live births in 2019. The 2019 disaggregated data showed mortality rates of 14.54 for boys and 13.28 for girls. The latest update from the organization states a global under-five mortality rate of 12.94 deaths per 1000 live births. According to studies, the rate of mortality of babies aged between 1 and 59 months was 80 out of 1000 births in low-income countries and six deaths per 1000 births in high-income countries [4, 5]. Some studies conducted across various regions of Iran have examined factors influencing mortality in children under five years old. The results of these studies indicate that several factors, such as parent’s education level and occupation, housing conditions, the distance of children from healthcare facilities, maternal age at marriage and childbirth, developmental indices of provinces, parental literacy rates, maternal employment, average income, life expectancy, birth weight, infant nutrition, and socio-economic status are significant determinants. Additionally, factors, such as birth order, birth spacing, birth complications, like birth injuries and pregnancy disorders, chronic and infectious diseases, and mortality due to accidents have been identified as influential contributors to this rate [6-11].
One of the most important indicators of children’s health is their mortality rate [1]. Understanding the causes of mortality is essential for implementing timely and effective preventive and therapeutic measures. Furthermore, through a more practical assessment of the risk factors contributing to children’s mortality, the current situation can be improved with appropriate planning and policymaking. Identifying the causes and determinants of mortality is highly important for ensuring the design and appropriate implementation of interventions to improve population health [12].
Therefore, aimed to systematically review the causes of death for children aged 1-59 months in recent years in Iran, in order to identify the factors contributing to child mortality to reduce mortality and improve children’s health in Iran.
Methods
This systematic review and meta-analysis was performed based on the systematic reviews and meta-analysis (PRISMA) guidelines.
Research question
What are the causes of mortality related to children aged 1-59 months in Iran?
Search process
Based on the inclusion criteria, we searched electronic databases, including EMBASE, PubMed, Scopus, Magiran and Web of Science, as well as the Google Scholar search engine up to January 2024. Other gray literature (such as conference proceedings and key journals) was also searched. The following operators were used: ([Cause] OR [cause-specific] AND [cause of death] OR [death cause] OR [death causes] OR [mortality] OR [child mortality] Or [infant mortality] OR [child mortalities] OR [mortalities, child] OR [mortality, child] AND [infant] OR [infant, newborn] OR [infant, premature] OR [infant, postmature] OR [newborn infant] OR [newborn infants] OR [newborns] OR (newborn] OR [children] OR [child] OR [child, preschool] OR [childs] AND [1–59-month] OR [2 to 5 years old] OR [1 and 23 months] AND [Iran]).
Target population
The target population included all died Iranian neonates and children aged 1–59 months.
Inclusion and exclusion criteria
The inclusion criteria were all observational studies that reported the causes of death in neonates and children aged 1-59 months, regardless of the language. The exclusion criterion was studies conducted in other countries (Table 1).
Type of exposure
Death in neonates and children aged 1-59 months.
Data extraction (selection and coding)
Full-text articles meeting the inclusion criteria were evaluated. Information such as the first author’s name, year of publication, study location, sample size, and causes of death was recorded in an Excel file. If additional information was needed from any of the articles, the corresponding author was contacted. All stages were performed independently by two individuals, and the compiled data were shared and combined.
Risk of bias assessment
The quality of studies was assessed independently by two individuals using the revised CONSORT risk of bias tool for clinical trials [17]. All studies that met the inclusion criteria were evaluated. Any discrepancies in assessments were resolved through discussion between the two individuals.
Analysis methods
Using Stata software, version 17 (Stata Corp LLC, College Station, Texas), the I² statistic was employed as the criterion for evaluating heterogeneity based on the quality of studies for subgroup analysis. The Begg test was used to assess publication bias. P<0.05 were considered significant in statistical tests.
Results
During the years under study (1999-2020), 15 studies were registered in Iran. Figure 1 shows the number of articles included in the study.
Characteristics of the included studies
After initial evaluations, a total of 15 studies were included in the systematic review [2, 13-26]. The publication period of the articles ranged from 2010 to January 1, 2024 and the sample size of the studies varied from 65 to 3,576 patients (Table 2).
Quality assessment
About 31.2% of the studies had a low risk of bias, and 56.2% had a moderate risk. Two articles had a high risk of bias. In most studies, there was no explicit mention of the questions, “Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed?” and “For the analyses in this paper, were the exposures of interest measured before the outcomes?” This lack of clarity represented the biggest weakness in the quality of the evaluated studies (Table 3).
The main outcome of interest in this study, the prevalence of congenital disorders, was analyzed in nine studies. The results of the data analysis in this study indicated that the highest frequency of mortality occurs in boys. The three most significant causes of death among Iranian neonates and children aged 1-59 months, respectively, are congenital disorders (28%), respiratory distress syndrome (18%) and non-traffic and traffic accidents (17%).
In this random-effects model, the mean score of this cause was calculated as effect size (EF)=0.28 [95% CI, 0.21%, 0.35%]. Other important causes of mortality in Iranian children aged 1-59 months include respiratory distress syndrome EF=0.18 [95% CI, 0.12%, 0.23%] and non-traffic and traffic accidents EF=0.17 [95% CI, 0.13%, 0.21%] (Table 4 and Figure 2).
Publication bias
The Begg’s test was used to assess publication bias in this outcome. It examines the effect of small studies and shows a P=0.000. Since this value is significant, it indicates that there is no publication bias (adj. Kendall’s score (P-Q)=1, SD=1.000, z=0.000, and Pr>|z|=1.000).
Discussion
The results indicated that the highest frequency of mortality occurs in boys. The three most significant causes of death among Iranian neonates and children aged 1-59 months, respectively, are congenital disorders (28%), respiratory distress syndrome (18%) and non-traffic and traffic accidents (17%).
The mortality of infants and children is a public health concern. Congenital abnormalities increase the risk of mortality during infancy and childhood, accounting for 26% of infant deaths and over 10% of deaths in children under ten years old in Europe [27].
Our results also indicated that the primary cause of mortality among children under five years old, with a prevalence of 28%, is congenital disorders. This finding is consistent with the results of other studies conducted in various countries [27-29].
It is crucial to implement primary and secondary preventive strategies, such as early referrals to specialized centers for high-risk pregnancies and prenatal care. These strategies considerably reduce the death rate from congenital anomalies in children and adolescents [28, 29].
One of the weaknesses identified in the studies was the lack of precise registration of the types of congenital disorders and abnormalities. This oversight could have hindered efforts in primary and secondary prevention over time and impeded more accurate international comparisons. Globally, unintentional injuries and deaths resulting from external factors, such as accidents, being struck by objects at home, swallowing foreign objects, and various poisonings, including methadone poisoning or other toxic substances, are among the leading causes of death in children. These factors account for 30% of deaths in children aged 1 to 3 years, 40% of deaths in 4-year-old children, and 50% to 60% of deaths in children aged 5 to 17 years [30-32].
Since a significant percentage of these external causes of mortality are largely preventable but often overlooked, there is a critical need for effective education on injury prevention. This requires a multi-faceted approach [33]. In addition, conducting education programs on traffic safety is crucially important. In the event of such accidents, it is essential to promptly refer the child to the hospital. Rapid diagnosis and the initiation of treatment significantly increase the chances of a favorable outcome [32].
Our study findings revealed that the third leading cause of death among Iranian children under five years old is related to respiratory infections. Patients succumbed to severe viral or bacterial infections (such as sepsis, pneumonia, and COVID-19) despite receiving treatment, with little chance of survival. The COVID-19 pandemic has also impacted the causes of child mortality and altered their distribution. Most deceased children had an underlying condition, such as congenital abnormalities [32, 34]. The results of this analysis should be discussed, and the conclusions drawn should positively impact the quality of childcare. Similar studies in other countries confirm that in both high and low-income countries, the leading cause of mortality among children under five years old is often respiratory infections and sepsis. This underscores the importance of addressing these issues to improve child health outcomes globally [35, 36]. Low levels of literacy among women may contribute to higher rates of neonatal infections. Consequently, illiterate mothers may struggle to recognize signs of danger and infection-related symptoms in infants, necessitating urgent medical care [36].
Study limitations: If autopsies are not conducted to determine the primary cause of death in deceased individuals, there is essentially no other definitive standard that clearly indicates the actual cause of death in a child. This lack of clarity is evident in studies. Additionally, in most studies, the age of deceased individuals was not categorized into neonatal deaths (0–27 days), post-neonatal deaths (28–364 days), or child deaths (over 365 days). Furthermore, none of the causes of death were recorded using international classification of diseases 10th revision (ICD-10) or ICD-9 coding.
Conclusion
The most common reasons for mortality in children aged 1-59 months in Iran are congenital abnormalities, unintentional injuries, and deaths due to external factors and respiratory infections. However, without accurate recording of causes of death using ICD-10 coding, without conducting autopsies or registering more detailed age categories for children under five years old, it is not possible to adequately analyze extensive patterns of mortality in the country. Consequently, related public health planning may suffer, leading to reduced effectiveness in health interventions.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Semnan University of Medical Sciences (Code: IR.SEMUMS.REC.1400.10).
Funding
The present article was extracted from the general medical practitioner thesis of Zahra Khorsi, approved by the Faculty of Medicine, Semnan University of Medical Sciences. This study was financially supported by Semnan University of Medical Sciences.
Authors contributions
Conceptualization, project administration and funding acquisition: Gholamreza Mohammadi; Methodology and supervision: Masoudeh Babakhanian and Gholamreza Mohammadi; Software: Masoudeh Babakhanian; Validation: Gholamreza Mohammadi and Raheb Ghorbani; Formal analysis, investigation and writing the original draft: Masoudeh Babakhanian; Resources and data curation: Shaqayeq Khosravifar; Review and editing: Masoudeh Babakhanian, Gholamreza Mohammadi and Raheb Ghorbani; Visualization: Raheb Ghorbani.
Conflicts of interest
The authors declared no conflict of interest.
References
- Sharaki A, Mardani M, Arab M, Firoozkoohi Z. [Infant under 1-59 month mortality causes in Zabol (Persian)]. IJNR. 2010; 5 (17):6-13. [Link]
- Chaman R, Alami A, Emamian MH, Naieni KH, Mirmohammadkhani M, Ahmadnezhad E, et al. Important risk factors of mortality among children aged 1-59 months in rural areas of Shahroud, Iran: A community-based Nested Case-Control Study. Int J Prevent Med. 2012; 3(12):875. [DOI:10.4103/2008-7802.104859][PMID]
- Chaman R, Naieni KH, Golestan B, Nabavizadeh H, Yunesian M. Neonatal mortality risk factors in a rural part of Iran: A nested case-control study. Iran J Public Health. 2009; 38(1):48-52. [Link]
- Behnampoor M, Havasian MR, Sargolzaei N, Mahmoodi Z, Salarzaei M, Mohamadi J. Investigating the mortality causes of 1-59 months babies of village from 2012 to 2015, Zahedan, Iran. Indo Am J Pharm Sci. 2017; 4(5):1079-84. [DOI:10.5281/zenodo.580837]
- World Health Organization (WHO). Under-five mortality rate (per 1000 live births) (SDG 3.2.1) [Internet]. 2024 [Updated 2024 November 16]. Available from: [Link]
- Nojomi M, Naserbakhat M, Ramezany M, Anbary K. Under-5 year mortality: Result of in-hospital study, Tehran, Iran. Acta Med Iran. 2009; 47(4):319-24. [Link]
- Farrahi F, Karami K, Hosseinzadeh H, Cheraghi M. [A study of social and economic factors affectingunder-5 children mortality as in rural area of Ahwaz In 2009 (Persian)]. Jundishapur J Health Sci. 2012; 4(2):1-11. [Link]
- Mohseni R, Pakzad H. [Effect of sociol-economical conditions on mortality rate of under 5 years children, Khuzestan-Iran (2009) (Persian)]. J Gorgan Univ Medical Sci. 2012; 14(3):121-8. [Link]
- Mohseni M. [Causes socio-economic and demography determinates in child mortality in Kashmar (Persian)] [master thesis]. Tehran: Tehran Univercity; 2000. [Link]
- Mirzai M,Alamdarey F. [Survey effect caseses child mortality in mianeh (Persian)]. Popul Hamun Season. 2006; 55(56):1-28. [Link]
- Hardelid P, Davey J, Dattani N, Gilbert R, Working Group of the Research and Policy Directorate of the Royal College of Paediatrics and Child Health. Child deaths due to injury in the four UK countries: A time trends study from 1980 to 2010. Plos One. 2013; 8(7):e68323. [DOI:10.1371/journal.pone.0068323]
- Zarghami M, Babakhanian M, Khavari A, Alipour A, Khosravi A, Saberi M. Drug-related death low registration in iran: a mixed method approach for causes, recommendations to solve this problem and geographical evaluation of an intervention. Addict Health. 2022; 14(2):138. [DOI:10.22122/AHJ.2022.196156.1266] [PMID]
- Rahbar M, Ahmadi M, Lornejad H, Habibelahi A, Sanaei-Shoar T, Mesdeaghinia A. Mortality causes in children 1-59 months in iran. Iran J Public Health. 2013; 42(Supple1):93-7. [PMID]
- Asadzadeh M, Pasha YZ, Aziznejadroshan P, Khafri S. Causes of infant mortality in Babol, Northern Iran. J Babol Univ Med Sci. 2022; 24(1):391. [DOI:10.22088/jbums.24.1.391]
- Pirzadeh Z, Jamshidi M, Arad B. Epidemiology of Diseases and Mortality in a Pediatric Intensive Care Unit in Qazvin, Iran. J Compr Pediatr. 2022; 13(2):e122885. [DOI:10.5812/compreped-122885]
- Naghibi SA, Moosazadeh M, Shojaee J. [Epidemiological features of under 5 year children mortality in Mazandaran (Persian)]. J Health Res Commun. 2015; 1(1):11-9. [Link]
- Safari H, Nooripour S, Emadi Z, Shakeri R, Jandaghi J, Mirmohammadkhani M. Associated factors of mortality of children aged 1 to 59 months in rural areas of Semnan: A nested case-control study based on 10 years of surveillance data. Koomesh. 2014; 15(3):282-88. [Link]
- Deihim Z, Aghababaeian H. [Evaluation of factors associated with mortality in neonate’s and children aged 1-59 months in Dezful City (2009-2014) (Persian)]. J Pediatr Nurs. 2015; 2(1):61-9. [Link]
- Sharaki Vahed A, Hamule MM, Arab M, Firuzkuhi Z. Infant under 1-59 month mortality causes in Zabol. Iran J Nurs Res. 2010; 5(17):6-13. [Link]
- Nasrabadi M, Hoseini S, Taghiyabadi E, Bozhabadi F, Borji S, Ghodsi H. [Causes of death in children aged 1-59 months in Neyshabur city from 2015 to 2019 (Persian)]. Mil Caring Sci. 2022; 9(3):289-98. [Link]
- Izadi N, Shetabi HR, Bakhtiari S, Janatalmakan M, Parabi M, Ahmadi K. [The rate and causes of infant mortaliry in the hospitals of Kermanshah Province during 2011-2014 (Persian)]. J Rafsanjan Univ Med Sci. 2016; 15(2):129-38. [Link]
- Khadivi R, Mirnasiry MS, Fazelian S, Aghababayi-Badi M. [The rate and the causes of under-5-year-old children mortality in Isfahan Province, Iran, during the years 2012-2018 (Persian)]. J Isfahan Med Sch. 2020; 38(582):469-76. [DOI:10.22122/jims.v38i582.12798]
- Hosseini S, Zahedpasha Y, Jahani M, Bijani A, Salmanian T. [The mortality rate in children aged 1-59 months in affiliated healthcare centers of babol university of medical sciences based on ICD10 (Persian)]. J Babol Univ Med Sci. 2022; 24(1):56-65. [DOI:10.22088/jbums.24.1.56]
- Ataey A, Alipour A, Khodakarim S, Khosravi A. [Epidemiology of under-5 mortality rate in Ardabil Province, Iran 2011-2015 (Persian)]. J Mazandaran Univ Med Sci. 2019; 28(168):160-5. [Link]
- Ahmadi SD, Tajedini F, Ehdaievand F, Moghimi-Dehkordi B, Farsar AR, Nejad ST. [Review of injuries leading to death in children aged 1to59 months in the area covered by Shahid Beheshti University of Medical Sciences from March 2011-March 2013 (Persian)]. Safety Promot Inj Prevent. 2014; 1(4):205-11. [DOI:10.22037/meipm.v1i4.60966]
- Momenifar M, Vazirinejad R, Ahmadinia H, Rezaeian M. [Survey of the mortality trend of children under 5 years old and the economic and health status of their families during the years 2011-2020 in Rafsanjan City: A descriptive study (Persian)]. J Rafsanjan Univ Med Sci. 2023; 22(4):401-18. [DOI:10.61186/jrums.22.4.401]
- Motlagh ME, Kelishadi R, Barakati SH, Lornejad HR, Amiri M, Poursafa P. Distribution of mortality among 1–59 month-old children across Iranian provinces in 2009: The national mortality surveillance system. Arch Iran Med. 2013; 16(1):22. [DOI:10.12669/pjms.291(Suppl).3515]
- Penchaszadeh VB. Preventing congenital anomalies in developing countries. Public Health Genomics. 2002; 5(1):61-9. [DOI:10.1159/000064632]
- Koshida S, Yanagi T, Ono T, Tsuji S, Takahashi K. Possible prevention of neonatal death: A regional population-based study in Japan. Yonsei Med J. 2016; 57(2):426. [DOI:10.3349/ymj.2016.57.2.426]
- Allameh Y, Akrami FS, Mohammadi G, Molavi N, Babakhanian M. Methadone poisoning in children: A systematic review and meta-analysis in Iran. J Pediatr Rev. 2017; 5(2):1-8. [DOI:10.5812/jpr.10133]
- Ezzati F, Shabani M, Mohammadhoseini T, Karimi F, Khodayari-Zarnaq R. Factors affecting children’s mortality due to traffic accidents using haddon model and statistical process control in Ardabil Province, Iran. Health Scope. 2022; 11(3):e120953. [DOI:10.5812/jhealthscope-120953]
- Kamianowska M, Kamianowska A, Wasilewska A. Causes of death in neonates, infants, children, and adolescents at the university children’s clinical hospital of Białystok between 2018 and 2021. Med Sci Monit. 2023; 29:e939915-1. [DOI:10.12659/MSM.939915]
- Harvey A, Towner E, Peden M, Soori H, Bartolomeos K. Injury prevention and the attainment of child and adolescent health. Bull World Health Organ. 2009; 87(5):390-4. [DOI:10.2471/BLT.08.059808]
- Emami A, Javanmardi F, Pirbonyeh N, Akbari A. Prevalence of underlying diseases in hospitalized patients with COVID-19: A systematic review and meta-analysis. Arch Acad Emerg Med. 2020; 8(1):e35. [PMID]
- Strong KL, Pedersen J, Johansson EW, Cao B, Diaz T, Guthold R, et al. Patterns and trends in causes of child and adolescent mortality 2000-2016: Setting the scene for child health redesign. BMJ Glob Health. 2021; 6(3):e004760. [DOI:10.1136/bmjgh-2020-004760]
- Odejimi A, Quinley J, Eluwa GI, Kunnuji M, Wammanda RD, Weiss W, et al. Causes of deaths in neonates and children aged 1-59 months in Nigeria: Verbal autopsy findings of 2019 Verbal and Social Autopsy study. BMC Public Health. 2022; 22(1):1130. [DOI:10.1186/s12889-022-13507-z]
Type of Study: Meta-analysis Review |
Subject:
Pediatrics
Received: 2024/06/30 | Accepted: 2024/09/1 | Published: 2024/07/1
Received: 2024/06/30 | Accepted: 2024/09/1 | Published: 2024/07/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC),
which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
